
Abstract
Introduction:
Data on subtotal cholecystectomy (STC) as an alternative to conventional cholecystectomy in difficult surgical situations are limited. This multiaspectual report aims to reduce the STC-specific knowledge gap and inform clinical decision-making strategies.
Materials and Methods:
All 180 patients who underwent STC at a single center between 2011 and 2017 were assessed in this retrospective cohort study. Their outcomes were followed up until March 23, 2018. Six subgroups stratified by surgical setting (elective/nonelective), surgical approach used (open/laparoscopic), and type of STC (reconstituting/fenestrating) were compared.
Results:
The ratio of conventional to STC procedures was 13:1. Of the 180 patients, 150 had a history of hospitalization for the acute biliary disease. The proportion of all cholecystectomies that were STC ranged from 1% to 71% between individual surgeons; similarly, laparoscopic STC comprised 0%–97% of all STCs. STC was associated with high intraoperative (n = 19; 10.6%) and short-term postoperative (n = 159; 88.3%) complication rates. There were three significant intraoperative complications—bleeding (n = 8; 4.4%), bile duct injury (n = 7; 3.9%), and intestinal injury (n = 4; 2.2%). The most common postoperative surgical site complications were external bile leak (21%), wound infection (17%), and biloma (10%). Associations between fenestrating STC and the rates of postoperative bile leak and retained gallstones, mainly in the main bile duct, were detected.
Conclusions:
STC-associated perioperative morbidity is significant. There is a substantial investigation burden. Injuries can be avoided when conversion to STC is timely, and its technical variant is correctly selected. The STC rate is a potential key performance indicator monitoring gallbladder surgery practice.
Introduction
Cholecystectomy is a standard treatment for symptomatic cholecystolithiasis. However, the management of patients with this disease is variable, even in countries with good access to quality health care.1,2 The reasons for this inconsistency are complex and multifactorial. However, the following contributing factors have been identified: lax acute biliary disease management standards; unwillingness to recognize the importance of nonelective index admission cholecystectomy; traditional emphasis on complete removal of a diseased gallbladder; and lack of a convincing description of the effects of gallbladder damage control surgery, in particular, subtotal cholecystectomy (STC). 3
The risks of conventional laparoscopic cholecystectomy are well known and have not changed over time. They include a 30-day cholecystectomy site-related perioperative complication rate of 2% and a systemic complication rate of 2.1%. 4 Given the substantial burden of cholecystectomy-related adverse events, 5 alternatives to conventional cholecystectomy that do not involve complete gallbladder removal in difficult operative conditions have long been sought.
The history of STC dates back to 1898 when a method of partial (subtotal) cholecystectomy without ligature of the cystic duct was suggested for rare situations where dissection of the cystic artery and duct is hazardous or the gallbladder is densely adherent to the liver parenchyma.6–8 Seventy-two scientific articles on STC were published between 1985 and 2017; they included 67 case series (n ≥ 5), two cohort studies, and three reviews (DOI: 10.17632/khv3b7b6wf.1). However, almost all of these studies were limited by small cohorts of patients or the inclusion of a narrow range of primary institutional data. Consequently, STC as a damage control procedure in challenging circumstances remains poorly understood. The concept of STC, especially when laparoscopic, is not universally accepted by general surgeons.3,9
Institutional analyses of demographics, preoperative conditions, perioperative morbidity patterns, long-term sequelae, investigation burden across the perioperative and postdischarge care continuum, and long-term survival in large cohorts of patients with the biliary disease who have undergone STC would show trends in overall and subgroup-specific STC rates over time. These data are needed as a basis for discussion of institutional practices regionally, nationally, and internationally.
In 2018, the authors formally launched an institutional analysis of a cohort of 180 patients who underwent STC between 2011 and 2017 and were followed up until March 23, 2018. The first objective of this study was to characterize this STC cohort. The second objective was to perform a subgroup analysis that would generate a set of STC tables and figures for surgical care providers considering STC as an alternative to conventional cholecystectomy in difficult surgical situations. The third objective was to describe the global and subgroup-specific effects of STC as a contribution to procedure-specific surgical epidemiology. 10
Materials and Methods
Study design, adherence, and repository data
This retrospective cohort study adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement and its checklist. 11 The Data Repository includes 109 tables and 53 figures and is organized into sections that follow the structure of the article (See Supplementary Material S1).
Identification of patients and analysis strategy
The STC cases were identified using Classification of Interventions and Procedures OPCS-4 codes. First, we investigated the preoperative status of each patient, indications for surgery, a technical variant of STC used, the incidence of perioperative complications according to the Clavien–Dindo classification system, 12 and the results of microbiological and histological assessments of the gallbladder. Second, we stratified the patients according to the setting of surgery (elective versus nonelective), surgical approach used (open versus laparoscopic), and type of procedure (reconstituting versus fenestrating). The same analytical framework was used to compare the individual variables in each subgroup. The third, fourth, and fifth tasks of this study were to determine the investigation burden, long-term consequences, and overall survival rates following STC.
Clinical informatics and statistical analysis
The hospital and patient-specific data were extracted and abstracted from electronic hospital data and document management systems. The results of radiological and endoscopic investigations were reviewed and taken into account as per the discretion of the specialist. The medical and survival status of all patients was checked on March 23, 2018. The initial data were collected in prepopulated paper forms, entered into an Excel (version 2011 for Mac®) database, and scrutinized for completeness and plausibility before statistical analysis. In total, 601 variables grouped into 70 clusters were analyzed.
GraphPad Prism versions 8.0.1 (145) and 8.3.1 (332) for macOS (GraphPad Software, Inc., La Jolla, CA, USA) were used to calculate the results. Conventional descriptive statistics for categorical variables were expressed as observed random events and percentage proportions with 95% confidence intervals (CIs). We used a fraction of total analysis to calculate the Wilson–Brown CI for a proportion. Binary regressions were utilized for subgroup analyses. Contingency tables were used to compute P values through two-sided Fisher's exact test and odds ratio point estimates with 95% CIs (by the Baptista–Pike method) for binomial proportions. Forest plots with a base-10 logarithmic scale on the x-axis were used for selected statistically significant odds ratio point estimates with 95% CIs to show the statistically significant associations between subgroups. The cumulative distributions of two sets of continuous one-dimensional data (age, body mass index [BMI], and others) were compared using the Kolmogorov–Smirnov test.
The survival analysis included patient factors and different levels of treatment. To construct the survival curves, Kaplan–Meier analysis was performed for pairs of subgroups using SPSS for Windows version 23 (IBM Corp., Armonk, NY, USA). Deaths from any cause were treated as censored observations for cumulative survival. The log-rank (Mantel–Cox) test was used to measure whether or not there was a significant difference in survival distribution between two subgroups of patients within a pair. The difference between subgroups was considered substantial at an α level of 5% (0.05).
Terminology
The term difficult gallbladder is used when there is a high risk of injury to the main bile duct or an extrahepatic bile duct, major blood vessel, or gastrointestinal tract if the gallbladder were to be completely removed. The term subtotal cholecystectomy is used to denote incomplete gallbladder removal (i.e., cholecystectomy characterized as subtotal when a portion of the gallbladder of any size was left in its anatomical site). The term original (Liverpool) classification of STC is used to encompass four variants (i.e., STC-1, STC-2, STC-3, and STC-4) and five subvariants (i.e., STC-1A, STC-1B, STC-1C, STC-2A, and STC-2B) of gallbladder resection. 13 The STC is defined as reconstituting when the remnant of the gallbladder or the cystic duct is closed off, and occlusion of this portion of the biliary tract is achieved (“closed-tract STC” is the equivalent term). Vice versa, the procedure is named as fenestrating when the continuity of this portion of the biliary tract remains (it is an open-tract STC).
Registration and ethics
The Institutional Clinical Audit Management Board reviewed, approved, and registered the project as a no-risk observational cohort study No. 6583.
Results
Trends and patterns
A total of 2501 patients underwent cholecystectomy (conventional, n = 2321; subtotal, n = 180) during the study period. Seven and 36 STCs were performed in 2011 and 2017, respectively (rate of increase, 59.2%; percentage change, 414.3). Figure 1 highlights a significant shift in the provision of surgical care for patients with benign gallbladder disease between 2011 and 2017 with respect to the completeness of cholecystectomy. Hepatobiliary, general emergency, upper gastrointestinal tract, colorectal, and endocrine organs' surgeons carried out 90, 70, 12, 6, and 2 STCs, respectively. Figure 2 shows variations in cholecystectomy practice among individual consultant surgeons. Substantial differences in laparoscopic STC practice in the range of 0%–97% were detected, too.

Number of conventional and subtotal cholecystectomies performed according to the setting of surgery, surgical approach, and type of procedure.
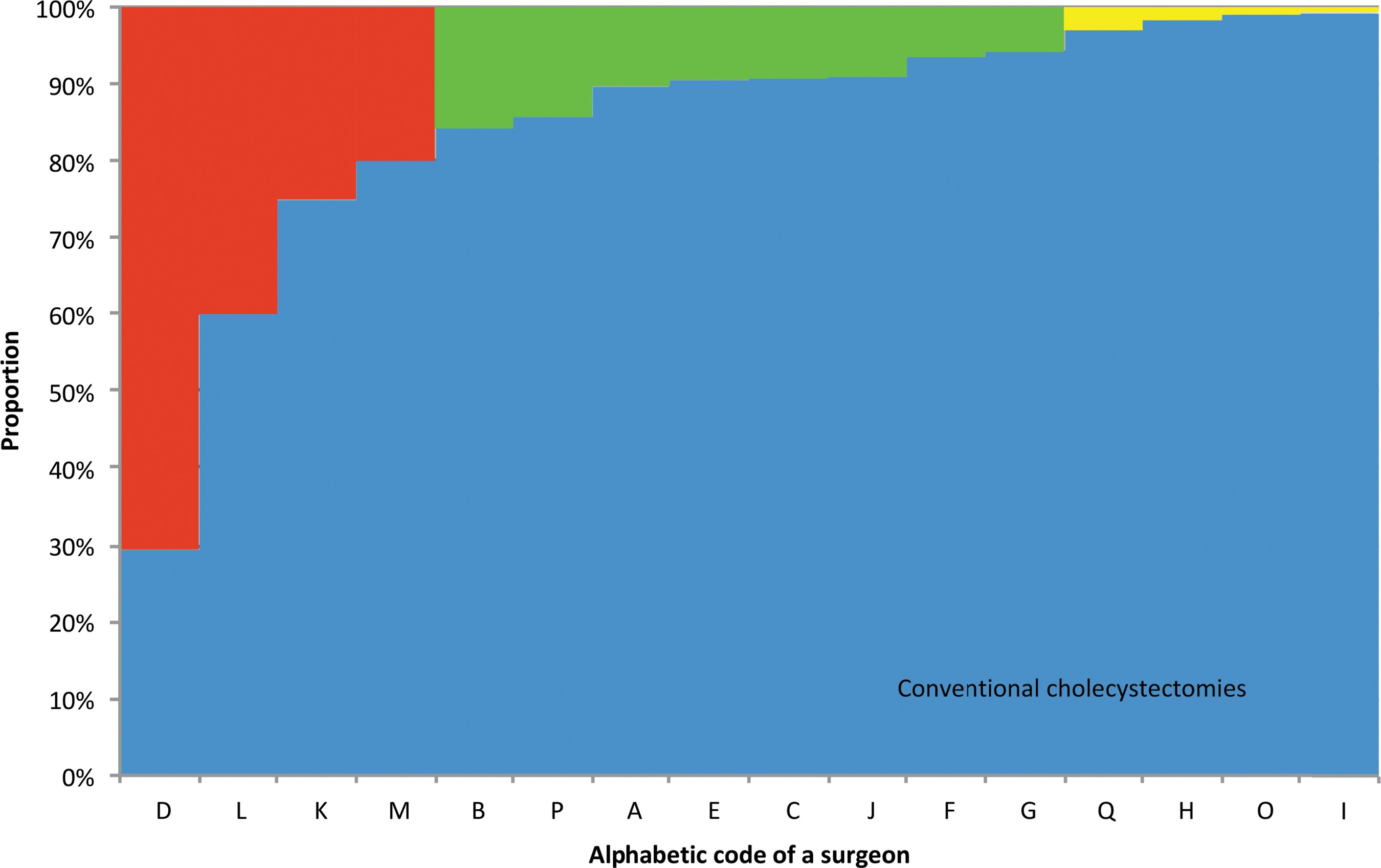
Proportions of conventional and subtotal cholecystectomies performed by individual surgeons. Sixteen consultant surgeons (coded by a random letter of the alphabet) in a 100% stacked column graph that highlights two percentage fractions from the total number of cholecystectomies. Conventional cholecystectomies performed by an individual surgeon are coded in blue columns and subtotal cholecystectomies are coded in red (high rates, 71.6%–20%), green (moderate rates, 15.8%–5.8%), and yellow (low rates, 3%–0.7%) columns. One case was excluded (one surgeon = one subtotal cholecystectomy, no conventional cholecystectomies registered).
Multiaspectual characterization of the cohort
Table 1 summarizes the characteristics of the study cohort. On average, men were 10 years older than women (64.3 years versus 54.4 years). Of note, 17 patients had a BMI ≥40; 92 patients had a Charlson age comorbidity index ≥3; 39 patients were taking a coagulation modifier; 150 patients had a history of hospitalization for the acute biliary disease.
Baseline, Clinical, Surgical, and Investigation Burden Characteristics of 180 Patients Who Underwent Subtotal Cholecystectomy
Previous emergency admissions with acute biliary disease.
95% CI limits, 95 percent confidence interval lower and upper limits; ASA, American Society of Anesthesiologists; BMI, body mass index; CACI, Charlson age comorbidity index; CT, computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; NA, not applicable; PMH, past medical history; STC, subtotal cholecystectomy.
A total of 113 patients (62.8%) underwent circular gallbladder resection (STC-1) and 58 (32.2%) patients underwent longitudinal resection of the gallbladder visceral wall (STC-2). Nineteen patients had intraoperative complications. Bile duct injury of type C (n = 4) or D (n = 3) during gallbladder surgery was documented in 7 patients. Five of them underwent postoperative endoscopic retrograde cholangiopancreatographies (ERCPs). The intestine was damaged in 4 patients (2.2%). Clinically significant bleeding occurred in 8 patients (4.4%). Histopathological tissue analysis revealed adenocarcinoma of the gallbladder in 3 patients.
Among the 180 patients, 159 had postoperative complications. Of these patients, 59 experienced a complication categorized as severe according to the Clavien–Dindo system. On aggregate, 56 patients had either external bile leak controlled by a drain inserted intraoperatively (38 patients, 21.1%) or localized biloma (18 patients, 10%). Some 11 patients had perihepatic collections not proven to be biliary in origin (6.1%). The rate of secondary surgical procedures during the same hospitalization was 22.2% (40 patients). ERCP was performed in 17 patients, percutaneous intervention in 11, relaparoscopy in 6, and laparotomy/relaparotomy in 6 patients. One patient (0.6%) died from biliary sepsis on postoperative day 1.
Investigation burden
A total of 532 computed tomography scans (n = 304), ERCPs (n = 153), magnetic resonance cholangiopancreatographies (n = 50), and endoscopic ultrasound scans (n = 25) were performed in these 180 patients between 2011 and March 23, 2018. Eighty-two ERCPs were performed in 61 patients (33.9%) before STC. The number of patients with post-STC ERCP, both predischarge (17 patients, 9.4%) and postdischarge (27 patients, 15.1%), constituted a substantial fraction of the cohort (24.4% [95% CI 18.7–31.2]). The overall global ERCP pattern over 4200 days is depicted in Figure 3.
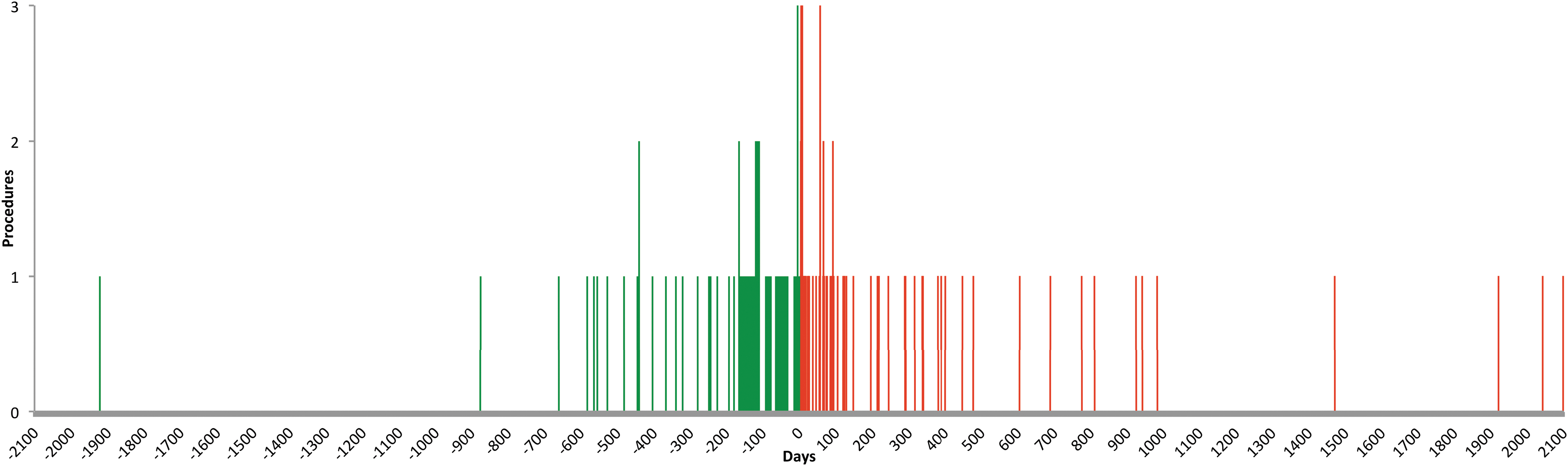
Distribution of 153 ERCP examinations performed at 2100 days before (82 ERCPs coded in green) and 2100 days after (71 ERCPs coded in red) subtotal cholecystectomy. An inverted parabola shape with STC at its vertex indicates that most ERCPs were performed at 100 days before and after STC; 13.4% of ERCPs were performed in 11 patients within 20 preoperative days, and 28.1% ERCPs were performed in 23 patients between preoperative days 21 and 100. The proportion of ERCP examinations was 26.8% (n = 19) within the first 20 postoperative days; the proportion of ERCPs performed between postoperative days 21 and 100 was similar at 29.6% (n = 21). In summary, 41.5% of all preoperative ERCPs (n = 34) were documented within 100 days before STC and 56.3% of all postoperative ERCPs (n = 40) were documented within 100 postoperative days. The figure shows advanced bile duct stone disease and postoperative bile leak in patients who underwent STC. ERCP, endoscopic retrograde cholangiopancreatography; STC, subtotal cholecystectomy.
Long-term results
The median follow-up duration was 2.5 years (880 days) with a maximum of 7.1 years (2543 days). During this period, calculi retained within the biliary tree were diagnosed in 29 out of 171 patients with gallstone disease (17%, 95% CI 12.1–23.3). Of these 29 patients, 17 (9.9%, 95% CI 6.3–15.3) had symptomatic choledocholithiasis and 12 (7%, 95% CI 4.1–11.9) had radiological evidence of gallstones within the gallbladder remnant. Extrahepatic bile duct strictures were detected in 7 patients (3.9%, 95% CI 1.9–7.8). Two patients (1.2%, 95% CI 0.2–4.2) underwent completion cholecystectomy.
The overall all-cause mortality rate was 7.2% (13 deaths) by March 23, 2018. Kaplan–Meier survival analysis showed significant differences in survival by age group (P = .039), Charlson comorbidity index (P = .013), Charlson age comorbidity index (P = .002), and positive oncological status (P < .0001). Six patients died from prostate, gallbladder, or lung cancer. No other variable was associated with a reduced survival rate (Fig. 4).
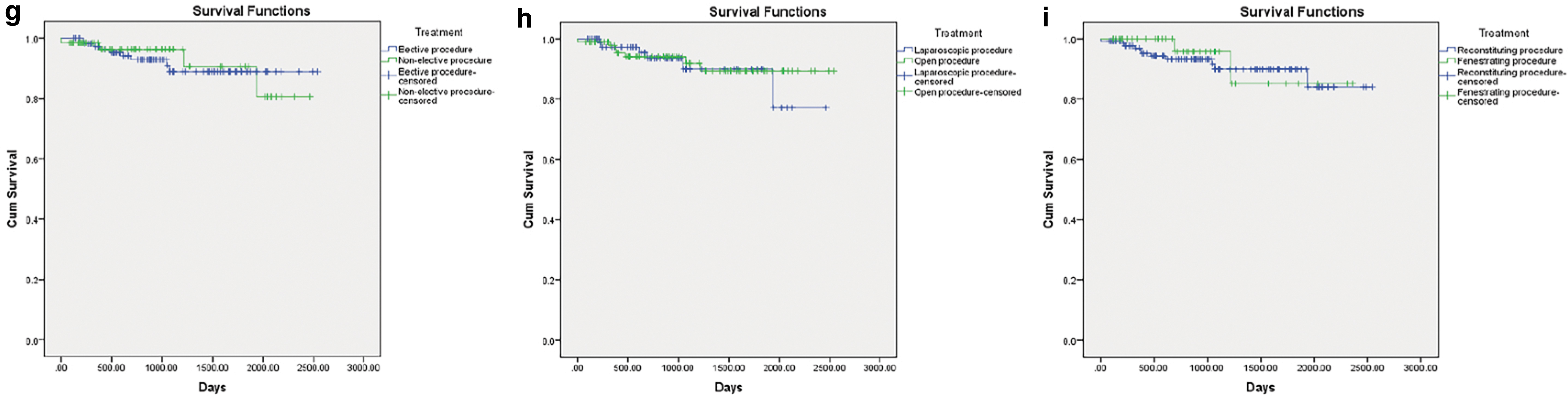
Cumulative survival (Kaplan–Meier) of all patients who underwent cholecystectomy stratified by
Subgroup analysis
Figures 5–7 show the statistically significant results of bivariate analyses carried out between the elective and nonelective, laparoscopic and open, reconstituting and fenestrating subgroups of patients according to individual preoperative, intraoperative, and postoperative factors. Forest plots revealed subgroup-specific patterns and trends. An example of an interpretation of Figure 5 is as follows: multiple previous hospitalizations for an acute biliary problem (a preoperative factor) predispose elective STC to the technical subvariant STC-2A (i.e., excision of the gallbladder visceral wall). Details of the subgroup analysis are presented in the Data Repository (see Supplementary Material S1).

Odds ratios for elective versus nonelective subtotal cholecystectomy according to preoperative, intraoperative, and postoperative factors. The odds ratio is displayed as a log scale on the x-axis. Comparison of six other variables revealed statistically significant differences associated with infinities within the odds ratio estimates. They were as follows: ASA class 4 (no elective patients), abandoned cholecystectomy, mainly due to an inflammatory mass (no cases in the nonelective subgroup; 24 of 25 cases were laparoscopic), repair of cholecystoduodenal fistula (no cases in the nonelective subgroup), xanthogranulomatous cholecystitis (15% of patients in the elective subgroup), patients hemotransfused on the day of surgery (8% of patients in the nonelective subgroup), and Escherichia coli as a single pathogen identified in fluid aspirated from the gallbladder (9 of 33 samples taken during nonelective surgery). The hospital stay was significantly longer in the nonelective STC subgroup. ASA, American Society of Anesthesiologists; STC, subtotal cholecystectomy.
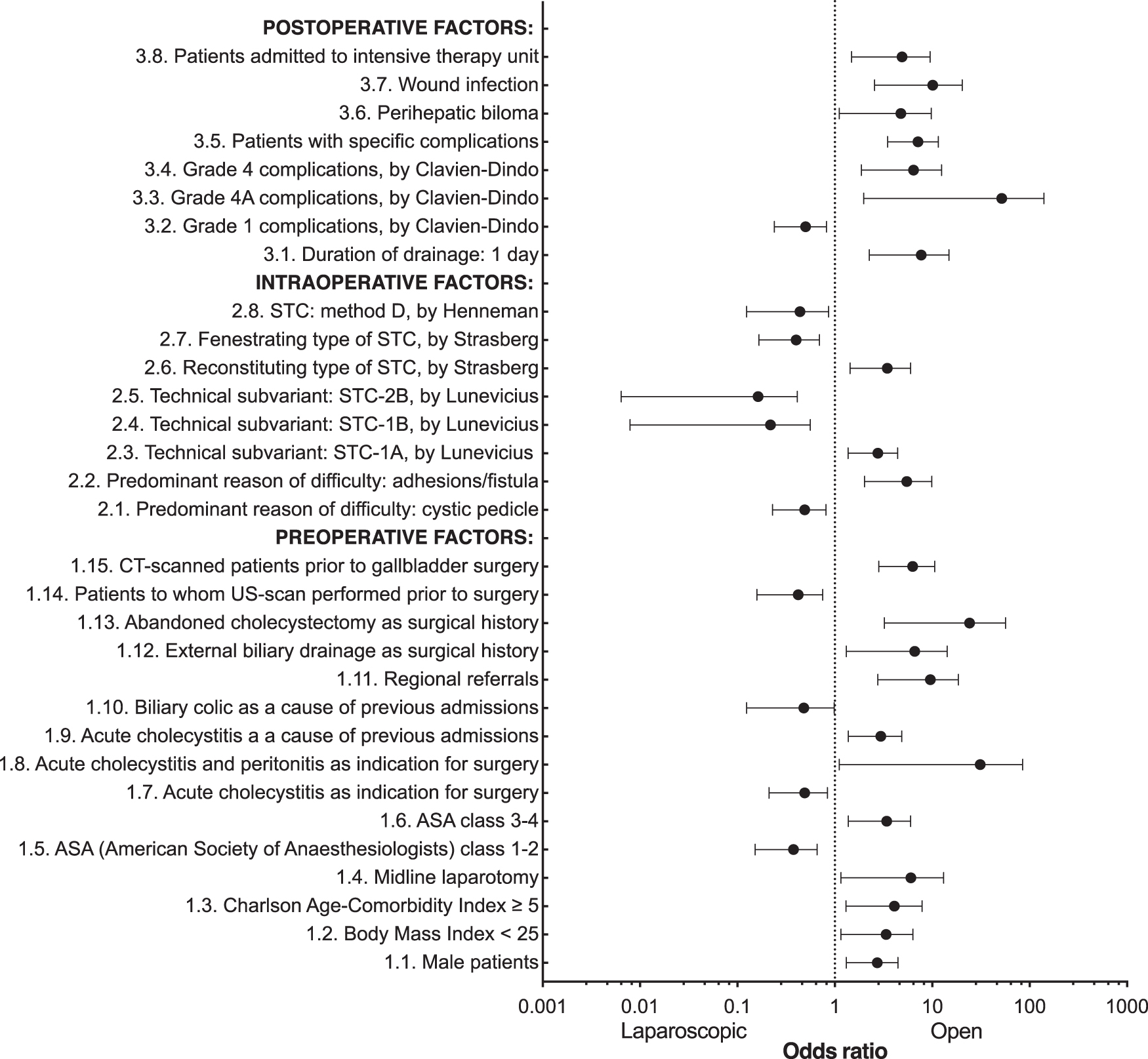
Odds ratios for laparoscopic versus open subtotal cholecystectomy according to preoperative, intraoperative, and postoperative factors. The odds ratio is displayed as a log scale on the x-axis. Comparison of three other variables revealed statistically significant differences associated with the infinities within the odds ratio estimates—insertion of the abdominal drain into perihepatic space (favors open STC, 100%), relaparotomy (observed only in the open STC subgroup), relaparoscopy (for laparoscopic STC subgroup only). The hospital stay was significantly longer after open surgery. STC, subtotal cholecystectomy.
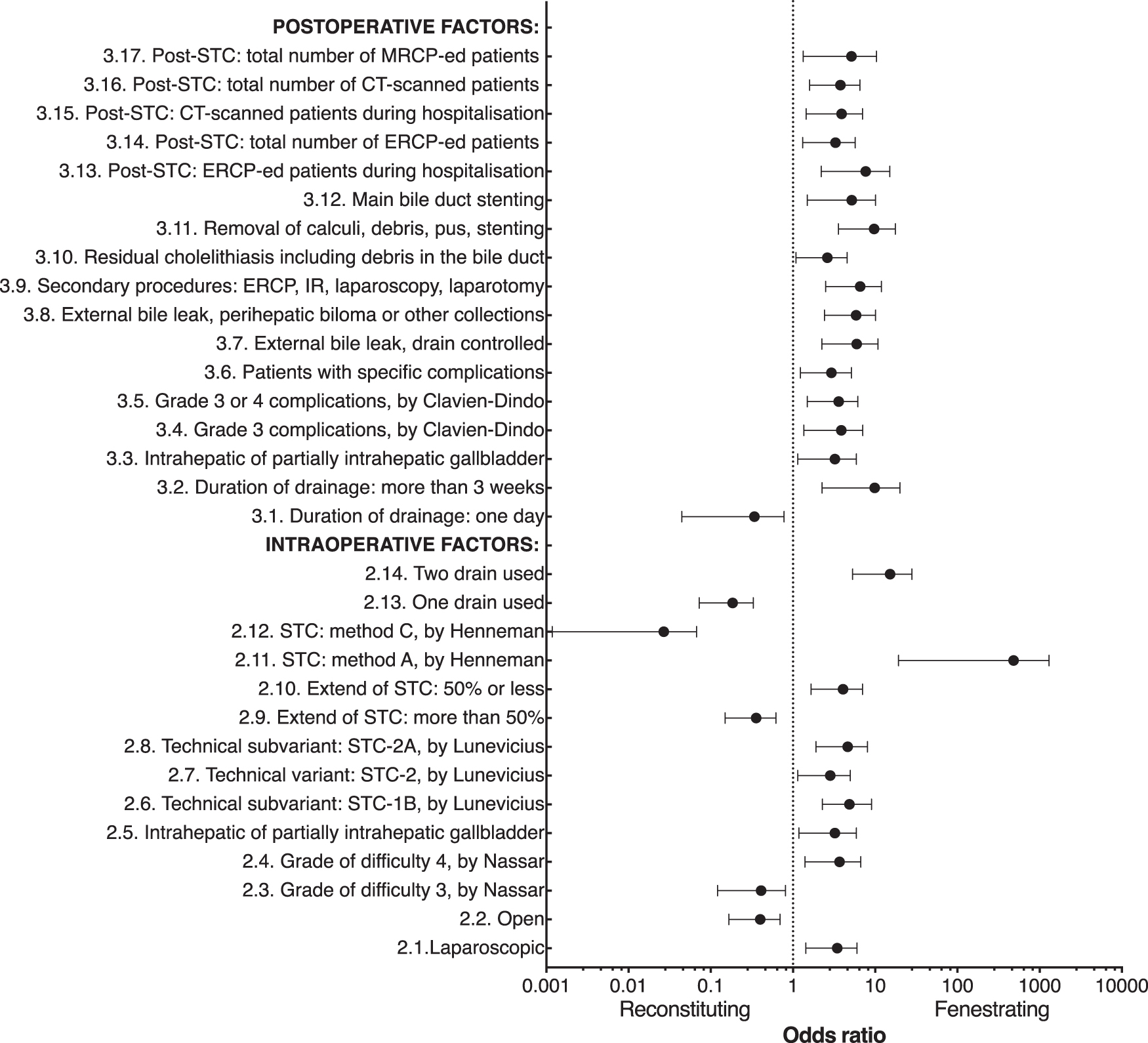
Odds ratios for reconstituting versus fenestrating subtotal cholecystectomy according to preoperative, intraoperative, and postoperative factors. The odds ratio is displayed as a log scale on the x-axis. Comparison of five other variables revealed statistically significant differences associated with the infinities within the odds ratio estimates, as follows: STC method B, by Henneman (reconstituting STC only), STC method D, by Henneman (observed only in the fenestrating STC subgroup), patients with Clavien–Dindo complications (100% in the fenestrating subgroup, 85% in the reconstituting subgroup), grade 3B Clavien–Dindo complications (observed only in the fenestrating STC subgroup), and repeat laparoscopy (not performed in patients who had undergone reconstituting STC). The hospital stay was significantly longer after fenestrating STC. STC, subtotal cholecystectomy.
Discussion
This study provides comprehensive information on the time trends and patterns of STC, preoperative characteristics, investigation burden, clinical outcomes, and survival of patients from one institution. We detected inconsistencies in the distribution of perioperative complication-specific morbidity and secondary surgeries performed in subgroups of patients stratified by the setting of surgery, surgical approach used, and type of procedure. Several findings of this study provide useful insights into STC.
STC was performed in 7.2% of all patients who underwent cholecystectomy during the study period, whereas other authors have reported substantially lower STC rates of 0.39% and 0.37%.14,15 There are two possible explanations for the difference in rates reported by different institutions. First, the patient population requiring cholecystectomy is regionally specific due to systematic delays in the provision of definitive treatment for symptomatic gallstone disease. Second, the institutional approach regarding cholecystectomy varies from institution to institution. Furthermore, in the present study, the proportion of all cholecystectomies that were performed as STC varied from 0.7% and 71.6% among individual surgeons, and rates of laparoscopic STC showed a more-than-seven-fold variation across all surgeons.
Perioperative complications and the investigation burden on patients need to be considered in terms of overall and complication-specific rates as well as the absolute number of complications and secondary procedures carried out to diagnose and control these complications. Focusing only on complication-specific rates (although there was a significant proven bile leak rate of 31.1%) can obscure the overall morbidity and investigation burden related to STC. In our study, analysis of 532 noninvasive and invasive procedures performed before and after STC confirmed that the main risks in patients who underwent STC were post-STC bile leak and need for a secondary intervention (e.g., ERCP, percutaneous drainage, relaparoscopy, or laparotomy). 14 One in 5 patients (22% of the cohort) underwent a secondary surgical procedure during the index admission.
STC is specifically designed to avoid bile duct injury in challenging surgical circumstances. However, there have been a few reports of STC-associated bile duct injury, which is the most feared complication of cholecystectomy.16–18 The STC-associated bile duct injury rate was 3.9% in the present study. Although the causation of these injuries needs to be investigated further, we associate them with STC for the purposes of this analysis. The finding that the majority of bile duct injuries and strictures were above the confluence of the common hepatic and cystic ducts confirms the assumption that the majority of extrahepatic bile duct injuries originate from attempts to channelize a proximal portion of the inflamed cystic plate above the cystic pedicle. Therefore, there is a need for more detailed investigation of the origin of the main bile duct strictures.
The results of this study are, to some degree, inconsistent with those of other STC studies with respect to perioperative complication rates.19–22 Our study shows that STC is a burdensome surgical procedure for patients with an intraoperative complication rate of 10.6% and postoperative complication rate of 88.3%. These rates are high and, therefore, STC cannot be comparable with conventional laparoscopic or open cholecystectomy. On the other hand, they also must be put in a different context as the morbidity from a lobar, common hepatic, or common bile duct injury far outweighs any morbidity that may arise from leaving a portion of the gallbladder in situ. 18 Strategies for the reduction of perioperative morbidity related to STC should be implemented. Examples would include early decision to convert from total to SCTs under challenging circumstances, the introduction of argon beam coagulation for the remnant mucosa of the gallbladder, and regular collaborative meetings, discussions, audits, and research.
The technical challenges when performing STC are well known. Several technical variants and types of STC have already been proposed.8,14,19,23–25 However, after a review of 180 STCs and personal laparoscopic STC files, we suggest a new STC nomenclature and classification, which encompasses the variants, technical modalities, and extent of resection of the gallbladder. 13 The type of completion of STC and patterns of perihepatic drainage are not features of this classification. It includes only the resection component of the procedure. The decision to close the remnant (reconstituting STC) or leave it open (fenestrating surgery) depends on the geometric features of the remnant of the resected gallbladder.
In our series, incidental gallbladder cancer after STC was detected in 1.7% of patients (i.e., in 1 out of 60 patients). This finding is alarming as the detection rate for incidental gallbladder cancer was reported to be 0.19% with any type of cholecystectomy, 0.05% with laparoscopic cholecystectomy, 0.6% with laparoscopic cholecystectomy converted to open cholecystectomy, and 1.13% with open cholecystectomy. 26 Furthermore, incidental gallbladder cancer (0.9%) was reported in another STC series. 27
The question regarding the risk of malignant transformation in the mucosa of the remnant gallbladder remains open. The cause and effect relationship for carcinoma in the remnant gallbladder is not expected to be higher than the risk of gallbladder carcinoma in the general population. Therefore, the remote chance of malignancy in a gallbladder remnant should not deter a surgeon from performing STC in an unusual situation. Patients with evidence of xanthogranulomatous cholecystitis in the resected portion of the gallbladder should be discussed in multidisciplinary team meetings and followed up regularly. 28
In the elective STC subgroup, 98% of patients had a history of hospitalization for an acute biliary event, and nearly 30% of these patients were admitted to the hospital three times before elective surgery. Most of them waited for elective cholecystectomy for more than 8 weeks after the last discharge from the hospital. Therefore, the likelihood of STC increases when patients with symptomatic gallstone disease are not managed in compliance with nationally and internationally recognized guidelines that recommend early cholecystectomy during the first index admission with acute calculous cholecystitis.29–31
The results of this study show a trend toward higher rates of perioperative complications, transfusions, and 30-day unplanned readmissions in patients who underwent open STC. This finding is in line with a previous report of poorer short-term outcomes after open STC than after laparoscopic STC. 15 We do admit that STC should be borne in mind as a last-resort temporizing maneuver to safely guide a patient through surgery. We also admit that there is currently no expert consensus on the selection of the surgical approach for STC when managing the most difficult gallbladders. 32 Likely, it will never be published as the very nature of the decision to perform a STC assumes that the biliary tract anatomy and complexity of the disease for a particular case is difficult and the management of it is dependent on a vast number of individual and institutional factors such as surgeon's experience in biliary surgery, decision making regarding timing to convert from total to STC, established departmental policies, and propagated operative procedures. However, results of this study suggest that surgical care providers should avoid conversions from laparoscopic to open gallbladder surgery if a failed attempt to complete a total cholecystectomy and save the patient from the reported morbidities of a STC would be predicted.
A reconstituting procedure (if applicable) is the first choice when STC is inevitable. In this series, the ratio of reconstituting to fenestrating STC was 3:1. Furthermore, fenestrating STC was associated with a higher intraoperative complication rate, postoperative bile leak, and recurrent biliary events. These results do not support the assumption that fenestrating STC is associated with a higher rate of postoperative bile leak, whereas reconstituting STC is associated with a higher rate of recurrent biliary events. 8 Moreover, our findings contradict the theory that there is a closer relationship between retained gallstones and reconstituting STC.9,10,14 We found no significant association between type of STC and residual calculi within the gallbladder remnant (6.2% for reconstituting STC and 9.5% for fenestrating STC). A twofold higher rate of gallstones in the main bile duct was found after fenestrating STC (17% versus 8%).
Overall survival was shorter in older patients (those ≥60 years) and in patients with positive cancer status. No significant association was found between the survival rate and the setting, approach, or type of STC. Furthermore, no significant associations with the survival rate were found in the specific subgroups (bile duct injury versus no bile duct injury, bile leak versus no bile leak, postoperative ERCP versus no postoperative ERCP).
This study has several limitations in terms of methodology and data. First, there was significant variation in the use of STC by individual surgeons. Therefore, we cannot exclude the possibility that STC procedures were undercoded owing to the inaccurate description of some of the operations performed. Second, the retrospective design of this study and the uncertainties arising within the data collation process are inevitable limitations, despite the use of a preplanned form for data collection and the quantity of data available from electronic systems at the institution. Therefore, we provide a 95% CI for each percentage fraction. A prospectively compiled database would mitigate these drawbacks.
In conclusion, this study is the most comprehensive assessment of STC to date and provides a tool for the characterization and conceptualization of STC with a higher level of detail than has been reported previously. It captures local variations in STC practice and may reflect current practice in biliary surgery across the country. STC rates increased at our institution between 2011 and 2017. Perioperative morbidity following STC was substantial. A laparoscopic approach and reconstituting type of STC were associated with lower perioperative event rates. A well-planned multicenter prospective evaluation of the epidemiology, merits, risks, and investigation burden of STC and the postoperative quality of life is needed to justify STC in unusual and hazardous surgical circumstances. The STC rate can be considered as one of the key performance indicators for gallbladder surgery for monitoring and appraising individual and collective cholecystectomy practice.
Footnotes
Acknowledgments
The authors thank Rebecca Roylance, Matthew J. Manton, and Marija Skirmantienė (deceased) for the time and effort they put into providing technical assistance.
Author Contributions
R.L. conceived and planned the study; summarized the references for the article; identified, extracted, and abstracted the data; performed statistical analysis; created the figures and tables; wrote the article and supplementary material (Mendeley Data). J.A.H. performed statistical survival analyses. Both authors provided intellectual input into various aspects of this study and contributed to subsequent revisions. The corresponding author had full access to all data in the study and had the final responsibility for the decision to submit for publication.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.