
Abstract
Introduction:
Laparoscopic sleeve gastrectomy (LSG) is now the most common bariatric procedure to treat morbidly obese patients. The main concern of LSG lies in the long-term weight regain, which is reported to happen in up to 75.6% of patients after 6 years. In this study, we report our overall experience with Laparoscopic Banded Sleeve Gastrectomy (LBSG) using the MiniMizer® over a 6-year period.
Materials and Methods:
We performed a retrospective review of data from a prospectively collected database. All patients submitted to primary LBSG were examined. Patients were submitted to LBSG between February 2014 and January 2020. Collected data included demographic factors, preoperative body mass index (BMI), operative time, surgical complications, and clinical outcomes.
Results:
Two hundred nine patients were submitted to primary LBSG in the study period. They were 136 females (65%) and 73 males (35%) with a median age of 43.0 years (range, 18–65 years). Median preoperative BMI was 48.4 kg/m2 (range, 36.2–65.5 kg/m2). Median operative time was 72.0 minutes (range, 40–142 minutes). Median time for ring placement was 8.0 minutes. Median postoperative hospital stay was 2.8 days. Seven major complications occurred in the postoperative period (3.3%): five gastric leaks (2.3%) and two major bleedings (0.9%). There was no postoperative mortality in the 209 patients. Long-term major complications occurred in 2 patients (0.9%). Median follow-up was 49.2 months (range, 2–72 months). Median postoperative BMI was 29.6 kg/m2 (range, 22–42 kg/m2). Median %excess weight loss (%EWL) at 1 year after surgery was 52.0%. Median %EWL at last follow-up visit was 64.0%.
Conclusion:
LBSG is as safe as standard LSG with excellent results in terms of postoperative morbidity and weight loss outcomes. Whether this procedure may result superior to standard LSG in the long-term period needs to be evaluated in randomized trials. Clinical Study Registration Number: NCT04354532.
Introduction
Laparoscopic sleeve gastrectomy (LSG) has gained worldwide popularity in the scientific community over the last years and is now the most common bariatric procedure to treat morbidly obese patients. 1 Its relative simplicity, the technical standardization, and excellent results have made this procedure popular in most bariatric institutions.
The main concern of LSG lies in the long-term weight regain, which is reported to happen in up to 75.6% of patients after 6 years. 2 A recently published large meta-analysis reports a weight recidivism rate of 28%, with an overall revision rate of 19.9% mostly due to weight regain. 3
The idea of banding the gastric stump after LSG arose from the reported evidence of an improved postoperative weight loss after banded Roux-en-Y gastric bypass (RYGB) compared to standard RYGB.4,5 Surgeons started to speculate about the chance of offering similar results to patients affected by morbid obesity with the banding of the upper portion of the gastric stump after LSG. It was thought that a silicon device might prevent the dilation of the stomach in the long-term without narrowing it in the early postoperative period. 6
Since then, many reports started to emerge in the literature with promising results.7,8 We reported early results of a randomized trial comparing banded versus standard sleeve gastrectomy, which showed a similar complication rate of the two procedures. 9
In this report, we report our overall experience with Laparoscopic Banded Sleeve Gastrectomy (LBSG) using the Minimizer® over a 6-year period at our institution.
Materials and Methods
We performed a retrospective review of data from a prospectively collected database. The study was approve by the Local Ethics Committee. All patients submitted to primary LBSG for morbid obesity were examined and analysis of results was performed. Patients were submitted to LBSG at our institution between February 2014 and January 2020. Follow-up took place at the institution's outpatient center at 1, 6, and 12 months with yearly visits thereafter. Collected data included demographic factors, preoperative weight, preoperative body mass index (BMI), operative time, surgical complications, and clinical outcomes in terms of short- and mid-term weight loss. Preoperative workup was completed in all patients and included multidisciplinary counseling, 10 laboratory tests, endoscopy, ultrasonography, pulmonary function assessment, and psychosocial-behavioral evaluation.11,12 Specific diagnostic tests were performed when required in single patients. A specific contraindication to LBSG was a preoperative diagnosis of gastroesophageal reflux disease (GERD) obtained with endoscopy, X-Ray swallow study, and pH-manometry.
Perioperative management was based on an enhanced recovery after surgery (ERAS) protocol in use at our institution since 2014. Postoperative follow-up was performed with both outpatient visits and phone calls when needed. The onset of “De Novo GERD” after LBSG was evaluated, but the analysis of the results is not finished yet. We are waiting for the long-term postoperative results. In addition, patients with preoperative GERD were excluded from LSBG.
In all patients, we used the MiniMizer Ring (Bariatric Solutions), a radiopaque silicone ring with four closing positions (8, 7.5, 7, and 6.5 cm). The ring has a blue color, and for this reason, it can easily be found back in revision surgery. The pulling lid is left in place with all closing positions to be adjusted postoperatively without having to place a new ring. The ring is slightly elastic and the fixation loops provide an anchor point to fix the ring in place, which prevents it from slipping.
As for the operative technique, LSG was performed as described previously. 13 When performing LBSG, a correct technique of gastric resection is mandatory with the complete removal of the gastric fundus to allow the ring to be put in place without narrowing the gastric lumen. At end of the procedure, a routine methylene blue test was performed in all cases and the Bougie removed. A silicone ring (MiniMizer; Bariatric Solutions) was then implanted (Fig. 1).

MiniMizer® Ring (Bariatric Solutions). Color images are available online.
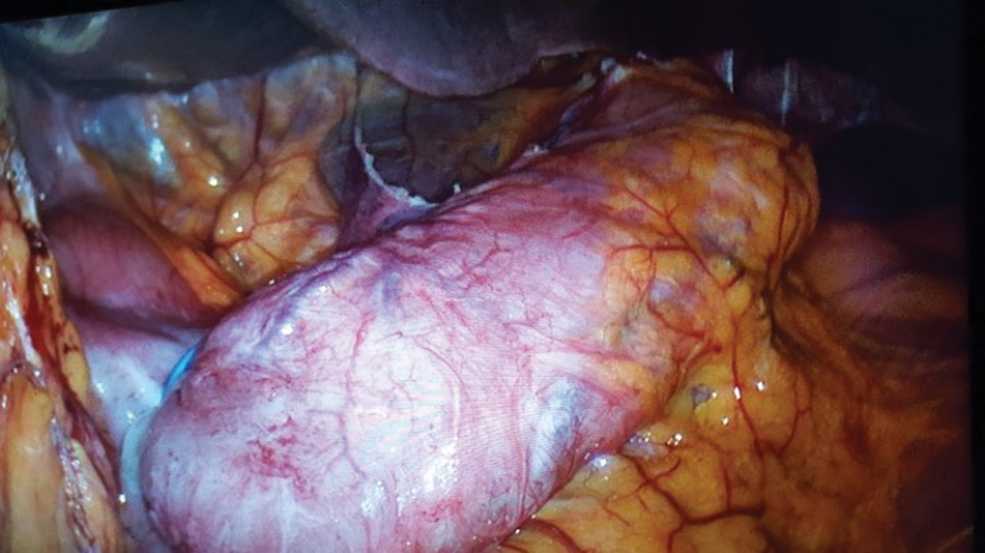
First, the ring was introduced into the abdomen through the left-sided trocar. A small opening was made in the peritoneum covering the lesser curvature of the stomach ∼4 cm from the gastroesophageal junction. The silicone ring is therefore pushed through the incision and guided along the posterior gastric wall. We closed the ring at the second closing position (7.5 cm, 24 mm of internal diameter) in all patients. The idea was to prevent future dilation rather than narrowing the gastric stump. This is the reason why the ring was left in place in a floppy way around the stomach (Fig. 2). The ring was then secured using silk 3/0 suture.

Intraoperative image of MiniMizer Ring (Bariatric Solutions). Color images are available online.
Results
A total of 209 patients were submitted to primary LBSG in the study period. They were 136 females (65%) and 73 males (35%) with a median age of 43.0 years (range, 18–65 years). Median preoperative BMI was 48.4 kg/m2 (range, 36.2–65.5 kg/m2). Median operative time was 72.0 minutes (range, 40–142 minutes). Median time for ring placement was 8.0 minutes (range, 5–22 minutes). Median postoperative hospital stay was 2.8 days (range, 2–14 days).
Seven major complications occurred in the postoperative period (3.3%): five gastric leaks (2.3%) and two major bleedings (0.9%). All leaks occurred at the gastroesophageal junction. Four patients with gastric leak were treated by laparoscopic drainage, ring removal, and esophagogastric stenting. The remaining patients with gastric leak were treated by laparoscopic drainage and esophagogastric stenting (Fig. 3).

X-Ray shows the esophagogastric stenting in a banded patient.
In this patient, the ring was left in place because the leak was minor as well as the peritoneal contamination. All (5/5) patients healed with stenting and recovered after stent removal. Major bleedings occurred at the staple line in one case and at trocar insertion in the second case. Both required laparoscopic revision. There was no conversion to open surgery in the study period. There was no postoperative mortality in the 209 patients. Long-term major complications occurred in 2 patients (0.9%): one ring erosion 2 years after surgery treated by endoscopic removal and one gastric stump dilation with ring slippage (Fig. 4) treated by laparoscopic ring removal.
Gastric stump dilation with ring slippage. Color images are available online.
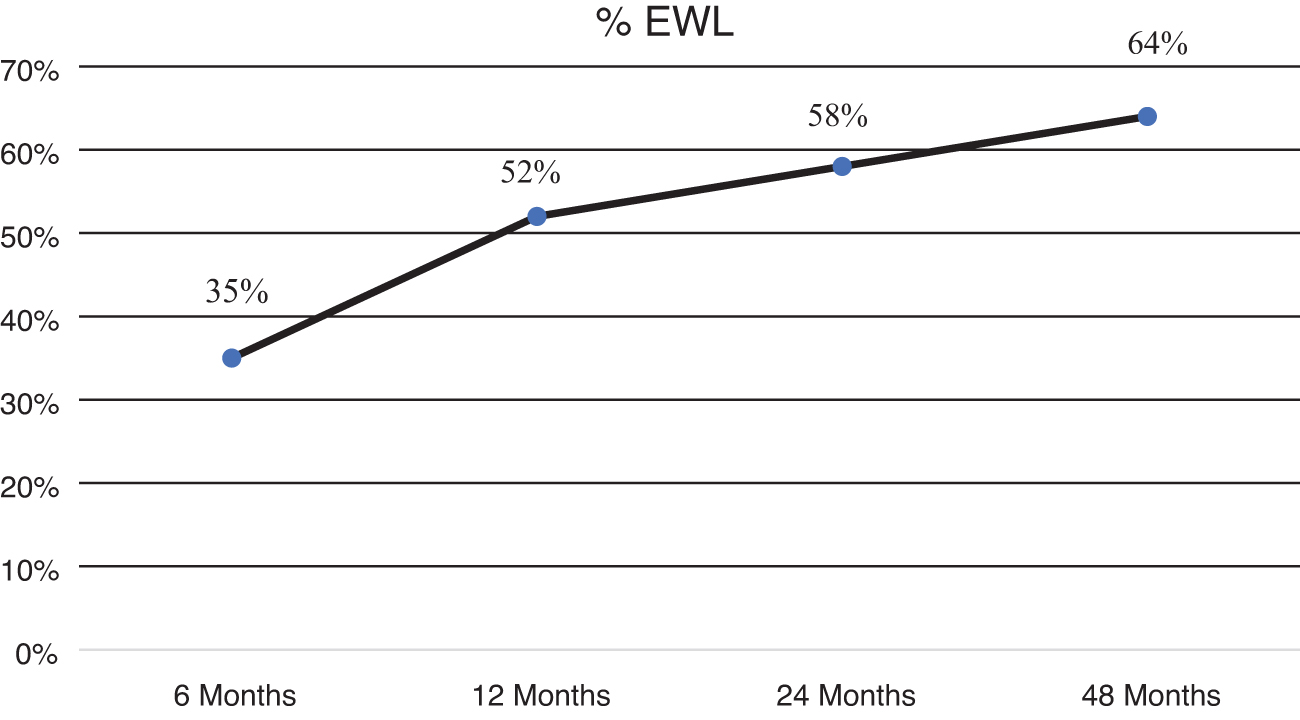
Mid-term follow-up was completed in 207/209 patients (99%), with 2 patients lost to either outpatient visit or phone call. Median follow-up was 49.2 months (range, 2–72 months). Median postoperative BMI was 29.6 kg/m2 (range, 22–42 kg/m2). Median %excess weight loss (%EWL) at 1 year after surgery was 52.0%. Median %EWL at last follow-up visit was 64.0% (Fig. 5).
Discussion
Although LSG is able to achieve excellent weight loss in the short term, sleeve dilatation and subsequent weight regain is a relevant issue in the mid-term period3,14; furthermore, long-term data are limited, with a successful EWL (defined as >50%) in only 55% of patients 8–9 years after surgery. About one-third of patients require revision due to insufficient weight loss. 3
With the aim to improve postoperative results in RYGB, surgeons have been implanting silicone rings on the gastric pouch just above the gastrojejunostomy.4,5 Various reports indicate significantly better results compared with nonbanded RYGB at 5 years postoperatively.4,5 These considerations prompted our group to start the experience with LBSG in 2014. Since then, a prospective database was created and all cases of LBSG were registered. We also performed a randomized trial comparing LBSG versus LSG and preliminary data at 2-year follow-up were published. 9 Mid-term results were also analyzed. Basically, we observed a better weight loss at mid-term follow-up (4 years) with a similar rate of postoperative and long-term complications; After a median follow-up of 4 years, the mean BMI in group of LBSG was significantly lower than group of LSG (24.10 ± 4.52 kg/m2 versus 28.80 ± 4.62 kg/m2; P = .00199). 14
The main concept of banding the sleeve in our opinion is based on the maintenance of restriction by preventing dilation. Our overall experience with LBSG, hereby reported, proves that LBSG using the MiniMizer Ring is a safe procedure and needs further investigations to establish its superiority to standard LSG. 15
On the other hand, LBSG is a novel procedure with limited reported series.6–8,16 A strong need for outcome reports is considered a priority for obesity surgeons. As a consequence, LBSG is increasingly performed in several centers. Although the actual number of performed LBSGs is difficult to estimate because national registers do not record these data, various published studies are being reported in the recent literature.6–8,16
The hypothesis that weight loss after nonbanded sleeves may be due to pouch dilation is reinforced by the number of re-sleeve cases reported in bariatric surgery journals. 17 Given the high frequency of long-term weight regain after a standard LSG, various authors have documented their approach to failed sleeves. Patients are usually studied with Barium swallow tests and computed tomography (CT) gastric volume three-dimensional (3D) reconstruction. 18 Surgical options for redo include re-sleeve, RYGB, one-anastomosis gastric bypass, biliopancreatic diversion with duodenal switch, or single anastomosis duodeno–ileal bypass with sleeve gastrectomy (SADI-S). 19 The presence of a ring does not prevent the surgeon from doing these procedures and the ring does not need to be removed. In this report, we did not present our cases of revision in banded sleeves because the number is extremely small (seven cases). We are starting to study with 3D CT reconstruction the volume of banded sleeves in the long term and will be able, in the near future, to report on these data. Obviously, we expect a minor dilation of the gastric stump due to the presence of the silicone ring, but this phenomenon is still under evaluation. We speculate that ring placement prevents gastric tube dilation below the ring and look forward to investigating CT imaging in banded patients.
Postoperative major complications in banded patients in our series (3.3%) are similar to those observed in reported experiences with primary standard sleeves.6–8,16 We observed five gastric leaks (2.3%), which were successfully treated in all cases with esophagogastric stenting. We previously reported our technique and management of gastric leaks after LSG, 20 which were easily performed in banded patients. Also, the patient in whom the ring was left in place could be stented with no technical complications. We supposed that the presence of the ring would not be a risk factor for staple line dehiscence because it was implanted in a floppy manner without creating a narrowing of the gastric stump and increased gastric pressure at the esophagogastric junction. Once again, the reason that prompted us to use the ring in sleeve gastrectomies was to create a barrier to gastric dilatation, mainly in the distal part of the sleeve.
Median EWL after LBSG in our series 1 year after surgery (52.0%) was as expected and comparable to our preliminary report of conventional LSG.13,21 Since then, patients with LBSG showed gradually a continuous decrease in BMI, which was unexpected and reached a %EWL of 64.0% at follow-up. Comparing results with standard sleeves was not the purpose of this study, having performed a randomized trial on it. Nevertheless, LBSG patients maintained stable body weight and BMI regain was a rare phenomenon. 22 A longer follow-up is needed to assess the real impact of the ring on sleeve gastrectomy, given that weight regain is an issue after this procedure as demonstrated by the study of Sarela et al. 3 In this work, the authors reported weight regain after conventional LSG with a concordant drop of EWL from 78% at 2 years to 60% at 8 or 9 years. Finally, we could have explored if the possible psychiatric comorbidities play a role in weight regain. 23
Conclusion
Our experience confirms the safety of LBSG with a low complication rate and equal to standard LSG. There is an increasing evidence that ring placement might be a useful tool for long-term weight control, a relevant issue after LSG. Extra restriction must be documented with imaging CT studies, which might demonstrate that LBSG is an option to consider in morbidly obese patients seeking surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.