
Abstract
Background:
The transoral endoscopic approach to the central neck has rapidly become one of the most widely utilized remote-access approaches for thyroid and parathyroid surgery in the world. The approach involves three small incisions inside the lower lip and has an optimal cosmetic outcome with no visible scar. However, the technique is quite difficult and poses several challenges that limit its widespread adoption. To overcome these issues, a novel lateral vestibular approach (LaVA) was explored in cadavers.
Methods:
Study using 7 fresh human cadavers that were dissected using open and endoscopic techniques to explore the feasibility of a transoral vestibular approach to the central neck without gas insufflation.
Results:
This novel approach resulted in wide access to the central neck and allowed for a total thyroidectomy and central neck dissection while preserving the marginal mandibular and mental nerves.
Conclusions:
LaVA permits excellent access to the central neck with a wide working space without the need for gas insufflation and overcomes many of the limitations of current transoral endoscopic approaches to the central neck.
Introduction
The first remote-access approach to the central neck was reported in 1996 to remove a parathyroid. 1 Since that time, there has been a rapid evolution of myriad techniques to achieve the safe removal of the thyroid, parathyroid, and/or central neck dissection without leaving a visible cutaneous scar. An increasing detection of thyroid nodules2–4 coupled with an increasing appreciation of the potential quality-of-life impact of a visible scar5–11 has made remote-access thyroidectomy more accepted and sought by patients and their surgeons.
Currently, the most utilized remote-access approach worldwide is transoral endoscopic thyroidectomy, vestibular approach (TOETVA). 12 This approach can also be performed with robotic instrumentation.13–16 The approach involves three small incisions inside the lower lip while tunneling narrow instrumentation into the central neck to create a working space maintained with insufflation. TOETVA has been shown to have excellent outcomes and be safe and feasible in numerous studies with thousands of patients. 17 However, there are challenges to this approach, which have prevented its widespread adoption, especially in the West. These include a steep learning curve, limited working space, need for CO2 insufflation with its inherent risks, inability to remove large specimens intact through the central incision, and difficult access in patients with prominent chins. A novel lateral vestibular approach (LaVA) was conceived to overcome these issues and will be described in this article.
Materials and Methods
Seven human cadavers were obtained from Massachusetts Eye and Ear between May 2018 and January 2020. This study was exempt from Internal Review Board approval. Cadavers were fresh frozen and thawed before dissection. Each cadaver consisted of at least a head and neck that was stabilized to an operative table with the neck slightly flexed and turned such that the body of the mandible was rotated to the midline of the patient (Fig. 1). An incision is made in the lateral vestibule through the buccal mucosa along the body of the mandible from the canine to just anterior to the retromolar trigone (Fig. 2). A cuff of mucosa is preserved and dissection continues to the periosteom of the mandible, similar to the approach for a fracture of the mandibular body. Anteriorly, the mental nerve is identified at the foramen and preserved (Fig. 3). The facial vessels mark the posterior aspect of dissection as they cross over the mandible. Along the inferior aspect of the mandible dissection proceeds in a deep plane to the platysma. With the platysma identified superiorly, a wide subplatysmal plane can be elevated with endoscopic assistance (Fig. 4). This is done between the sternocleidomastoid muscles laterally and to the sternal notch inferiorly. A custom-made external retractor is then placed under the platysmal and elevated to maintain the working space without CO2 insufflation (Fig. 5). At this point, the central neck is fully exposed and thyroidectomy and central neck dissection were performed with laparoscopic instrumentation in a similar manner to TOETVA. 18 Once released, the specimen can be easily retrieved through the oral incision without compromise of its structural integrity.

Position of the neck rotated and slightly flexed.

Incision in the lateral vestibule through the buccal mucosa along the body of the mandible from the canine to just anterior to the retromolar trigone.

Elevation of the soft tissue off the body of the mandible with preservation of the mental nerve.

Development of the working space with endoscopic instruments.

Maintenance of the working space with an external retractor.
Results
Seven human cadavers were used to explore this novel technique. Various approaches, including placement of intraoral incisions and supra- and subplatysmal dissections, were performed. At the completion of the endoscopic procedure, external dissections were performed to confirm integrity of the marginal mandibular nerve and recurrent laryngeal nerves. The approach described earlier resulted in an unfettered endoscopic view of the central neck with preservation of the mental, marginal mandibular (Fig. 6), and recurrent laryngeal nerves (Fig. 7). See Supplementary Video S1.
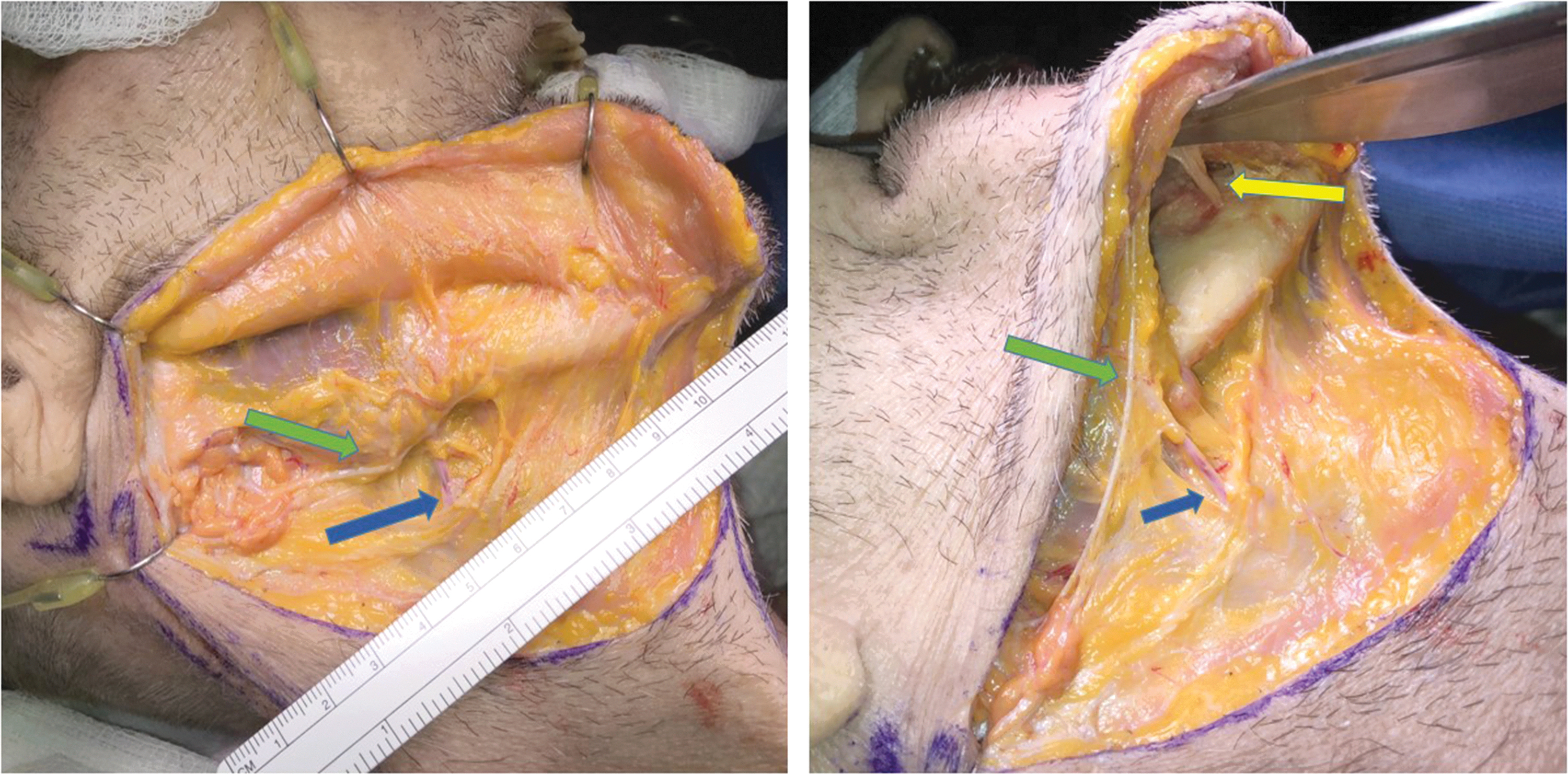
External dissection after LaVA thyroidectomy demonstrating integrity of the mental (yellow arrow) and marginal mandibular (green arrow) nerves. Facial vein identified by blue arrow. LaVA, lateral vestibular approach.

External dissection after LaVA thyroidectomy demonstrating integrity of the recurrent laryngeal nerve (green arrow).
Discussion
Remote-access thyroid surgery remains a topic of great interest and controversy. The past two decades have seen the introduction of multiple techniques with access points in the chest, axilla, lateral neck, and mouth. Various surgeons and institutions have adopted one or more technique; each with its own profile of advantages, disadvantages, and complications.
Proponents of remote-access thyroid surgery cite the growing body of evidence that a visible cervical scar can significantly impact a patient's quality of life and self-perception.5–11 If this can be avoided, and if the attendant risks and complication profile are commensurate with traditional transcervical thyroid surgery, then adoption of these techniques are a worthwhile endeavor. However, many of these techniques involve significantly longer operating times, steep learning curves, and new complications while failing to demonstrate cost-effectiveness. For this reason, many surgeons have remained skeptical of the safety and utility of remote-access thyroid surgery and/or abandoned these procedures altogether.19–21 Adoption of these techniques has been especially slow in the United States.
Recently, the transoral endoscopic approach has become the dominant procedure performed worldwide. The initial transoral vestibular approach was described in 2011. 22 In 2014, Dr. Anuwong published his landmark article describing the initial experience with TOETVA. 23 Since this time, it has been adopted by >50 centers across the globe (personal communication). In contrast to some of the other techniques, it can be performed endoscopically, as well as robotically, and has been shown to be similar to traditional transcervical thyroid surgery in terms of operative time, risk profile, complications, and outcomes in experienced hands.17,24,25 This approach involves three small incisions in the lower lip through which trocars are placed and advanced into the subplatysmal plane in the neck. A working space is created with CO2 insufflation and instrumentation (e.g., either laparoscopic, robotic, or both) are used to dissect the thyroid, parathyroid, and/or central neck contents. The specimen is then placed in an endoscopic retrieval bag and extracted through the central (1.5–2 cm) incision. The three incisions heal rapidly without any evidence of scarring.
Although TOETVA has proven successful for both benign and malignant conditions, 25 there are several noteworthy drawbacks. First and foremost is that the procedure involves small incisions and the requirement of CO2 insufflation to maintain a working space. There is a steep learning curve to using laparoscopic instrumentation and insufflation with this novel approach, especially for otolaryngologists who do not have training in fundamentals of laparoscopic surgery. CO2 insufflation poses an inherent risk of life-threatening embolization. 26 There can be difficulties with maintaining an airtight seal and the need to increase insufflation pressure. Working in the narrow space poses challenges manipulating the instrumentation. Furthermore, the energy devices produce aerosolization and fogging that obstructs the endoscopic view and requires venting of gas and frequent removal and cleaning of the scope. This interferes with the smooth progression of surgery and can make for a frustrating experience.
Another major concern with TOETVA is that the narrow central incision makes intact retrieval of larger specimens (>4 cm) very difficult. This issue is more challenging in non-Asian populations with more prominent chins. The specimen requires a good deal of manipulation to pass over the mandible that may jeopardize its structural integrity. This is particularly concerning in follicular neoplasms in which a crushed or torn specimen may render definitive diagnosis difficult. 27 Larger specimens have been morcellized or have the capsule incised to extract them, which again, jeopardizes the ultimate pathological interpretation.
The ideal “scarless” approach to thyroid surgery remains elusive. Such an approach would involve minimal tissue dissection, a wide working space, excellent visualization, avoid insufflation, access both sides of the neck, and allow for intact extraction of large specimens. The LaVA was conceived with these goals in mind. The incision is similar to that made for a transoral approach to a mandibular body fracture. The head is rotated and a subplatysmal plane is elevated and maintained with an external retractor. Access to both sides of the central neck is afforded and dissection can proceed in a wide working space either with laparoscopic or robotic instrumentation. The wide incision should accommodate retrieval of most specimens without compromise to the pathological analysis.
The actual dissection of the thyroid and central neck would proceed identical to that of TOETVA. Insufflation would not be necessary and blurring of the visual field should not be a problem given the large incision to vent through and evacuate vapor. However, the technique does require the head to be rotated to one side, which may medialize the ipsilateral sternocleidomastoid muscle and potentially restrict the working space. This approach also poses potential greater injury to the ipsilateral mental nerve, which is identified and partially dissected. In contrast, the TOETVA technique poses risk to both mental nerves with the lateral port sites although they are not isolated and dissected.
There may be an additional cosmetic benefit of LaVA. The passage of the laparoscopic instruments over the mentum in TOETVA can result in soft tissue thickening, puckering, and submental banding, which usually resolves. However, in LaVA the soft tissue elevated along the mandibular body would likely have less of an impact and would be in a less sensitive cosmetic area.
The greatest concern with LaVA is potential injury to the marginal mandibular nerve branches with dissection from the oral vestibule to the neck. Branches of the marginal mandibular nerve (there are typically two to three) run immediately deep to the deep facial fascia, which is continuous with the parotidomasseteric fascia in the lateral face, and continuous with the investing layer of the deep cervical fascia in the neck. Traversing from the periosteum of the mandible heading superficial to the immediate subplatysmal space (i.e., immediately deep to the superficial cervical fascia) poses a theoretical risk of marginal mandibular nerve injury as the investing layer of the deep cervical fascia is crossed. However, in Dingman and Grabb's landmark study, 28 they described that anterior to the facial artery, all of the branches of the marginal mandibular nerve are above the inferior border of the mandible and should, therefore, be protected in this approach. Any small branches identified anterior to the facial artery and inferior to the border of the mandible innervate the platysma muscle and not the depressor muscles of the lip.
Remote-access and “scarless” approaches to the thyroid gland continue to evolve. To date, each approach has its various constraints that make them appropriate only in select patients. The LaVA was conceived to avoid some of these limitations and be suitable to a wider range of patients. Ultimately, the safety and feasibility of this novel technique has to be further evaluated in live human patients.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.