
Abstract
Introduction:
Boerhaave's syndrome is a life-threatening spontaneous perforation of the esophagus associated with significant morbidity and mortality. Historically, thoracotomy has been the mainstay of treatment, but is associated with high morbidity and pain. Minimally invasive approaches provide alternative treatment possibilities. This systematic review together with inclusion of a case series from a tertiary esophagogastric unit assesses current evidence focused on minimally invasive surgical management of this condition.
Methods:
A systematic review was conducted in line with MOOSE (Meta-analyses Of Observational Studies in Epidemiology) guidelines. Electronic databases PubMed, MEDLINE, and Cochrane Library were searched, and articles focusing on the minimally invasive management of Boerhaave's syndrome were identified and scrutinized. We also report demographics and outcomes for a consecutive case series of patients with acute Boerhaave's syndrome managed via thoracoscopy.
Results:
Fifteen studies were included comprising 5 retrospective cohort studies and 10 case reports. Management strategies were divided into three categories: thoracoscopic, endoscopic, and laparoscopic. Overall mortality rates for each treatment modality were 2%, 13%, and 33%, and treatment success rates 98%, 38%, and 67%, respectively. Postoperative infective complications were seen in 79% of patients, with only 2 patients requiring salvage thoracotomy. In our local case series, we report 4 consecutive patients managed with thoracoscopy, with a 100% treatment success rate.
Conclusion:
Minimally invasive approaches in the management of Boerhaave's syndrome are safe and effective. We propose a selective management algorithm involving a minimally invasive approach to management of this life-threatening condition. Registered with local clinical outcomes team as service evaluation. (Approval number sev/0171).
Introduction
Boerhaave'
The classically described Mackler's triad of vomiting, retrosternal chest pain, and subcutaneous emphysema is present in only 14% of patients, leading to difficulties in diagnosis due to the nonspecific nature of presenting symptoms. 2 Boerhaave's syndrome ranges from small gas- or fluid-filled perforations, which remain contained within the mediastinum, to large esophageal defects with frank soiling of mediastinum and pleural cavity with food and enteral secretions resulting in life-threatening inflammatory response and sepsis. Pleural and mediastinal contamination by gastric content, often including undigested food matter, means that reported mortality rates are as high as 20%–40%, rising to 100% in patients where urgent surgery is not pursued.4,5
The fundamental principles of management of Boerhaave's syndrome include early recognition, elimination of septic foci, and nutritional support.5–7 Reports on the adjunctive use of endoscopic stents or clips have been published, although the impact of these on clinical outcomes is unclear.1,2,4,5 Current literature suggests that the proportion of nonseptic patients with well-contained perforations, who may be amenable to conservative management through the use of selective radiological drainage, is small.4,8 Septic patients, or those failing to progress on conservative management, must be reconsidered for surgical intervention. 5
Historically, the surgical approach to Boerhaave's syndrome comprised lateral thoracotomy to control the primary defect and laparotomy to address any abdominal contamination and secure nutritional access via gastrostomy or jejunostomy. 9 Thoracotomy, however, is associated with significant morbidity.10,11 Pulmonary complications following thoracotomy are reported in as many as 60% of cases. Thoracotomy is also known to result in a significant impact on long-term quality of life, with chronic pain reported in up to 40% of patients.11,12
Thoracoscopy has been shown in elective thoracic procedures to result in significantly improved outcomes. A Swedish national cohort study (n = 1601) demonstrated reduced morbidity rates and lengths of stay following thoracoscopic lobectomy compared to an open approach. 13 Reductions in postoperative pain and improvements in quality of life with a minimally invasive thoracic approach are also well documented.14–16 In Boerhaave's syndrome, only very limited data are available on the efficacy of minimally invasive surgery. A small observational study comparing 7 thoracoscopically managed patients to a group of traditionally managed (thoracotomy) patients by Cho et al. demonstrated reduced operation times (3.7 hours versus 5.3 hours, P = .005), reduced complication rates, and reduced incidence of postoperative pulmonary infections. 10
We conducted a systematic review of current literature for the minimally invasive surgical management of Boerhaave's syndrome, supplemented with our own data. We aim to outline current best evidence and propose a management algorithm regarding the use of minimally invasive surgical strategies in the management of Boerhaave's syndrome.
Materials and Methods
Search strategy and data synthesis
A systematic review was conducted in line with Meta-analyses Of Observational Studies in Epidemiology (MOOSE) reporting guidelines. 17 PubMed, MEDLINE, and Cochrane Library databases were searched from database inception up to the end of January 2020. The search strategy combined (“boerhaave” OR “esophageal rupture” OR “ruptured esophagus”) AND “minimally invasive” OR “thoracoscop*” OR “VATS” OR “endoscop*” (incorporating Boolean operands “AND” and “OR” as shown).
Initial screening of titles and abstracts identified articles of interest, which then underwent full-text analysis and data extraction. Reference lists of retrieved articles were hand-searched for additional relevant references. The search was conducted by 2 researchers (P.H.P. and O.P.) with any discrepancies resolved following discussion and consensus.
Demographic, surgical, and outcome data were extracted and collated in Microsoft Excel (Microsoft Corp., Redmond, WA). Treatment success, defined as patient recovery without further surgical intervention, was assessed across the reported modalities.
Selection criteria
Studies considered for inclusion were those which reported outcomes for minimally invasive management of Boerhaave's syndrome, defined as spontaneous esophageal perforation not related to foreign bodies, iatrogenic injury, recent surgery, malignancy, or trauma. Minimally invasive was defined for the purposes of this search as any management strategy or surgical approach other than thoracotomy. As our aim was to capture data for septic patients requiring operative management of Boerhaave's syndrome, studies reporting patients with delayed presentation (>48 hours) or incidental finding of perforation were excluded.
Methodological quality
Study quality was assessed using the Newcastle-Ottawa Scale for cohort studies. Scores ranging from 0 to 9 are assigned based on a number of methodological factors. These include the study sample's representativeness of the exposed cohort as well as methods used to confirm exposure, selection methods for the nonexposed cohort, comparability of the cohorts, and attempts to control for potential confounding factors, appropriateness of outcomes measured, and adequacy of follow-up duration. 18
Local technique and case series
Following local institutional approval (approval number sev/0171), anonymized demographic details and outcomes for patients presenting with Boerhaave's syndrome were retrospectively retrieved from a local electronic database. All patients were investigated and managed in a standardized manner. Postoperative morbidities were graded according to the Clavien-Dindo classification system. 19
Initial investigation included a full panel of blood tests, plain chest radiograph, and computed tomography scan with oral and intravenous contrast. Patients with sepsis and confirmed Boerhaave's perforation with contamination of pleural cavity or mediastinum proceeded to urgent surgery within 48 hours of symptom onset under the care of a subspecialist upper gastrointestinal surgeon at our tertiary esophagogastric center. All the patients reported here underwent left-sided thoracoscopy in the right lateral decubitus position, with intubation using a dual-lumen endotracheal tube. Initial gastroscopy was performed to confirm the diagnosis and assess the defect. Following desufflation of the lung, three-port thoracoscopy was performed, with thorough irrigation until clear. Two chest drains were positioned (one basal, one mediastinal) and secured. No attempt was made at closure of the esophageal defect. Finally, two endoscopically placed gastrostomy tubes were inserted, one to facilitate gastric decompression and a second tube with jejunal extension placed for enteral feeding. Regular intravenous antibiotics and proton pump inhibitors were administered.
Our institutional practice for surgical management of esophageal perforation has been washout debridement and drainage of esophageal perforation for several years. The rationale for adopting this strategy has been that primary repair with or without T-tube often results in incomplete control of leakage. Our current video-assisted thoracoscopic surgery (VATS) approach to esophageal perforation is a logical minimally invasive development of our prior practice with the same local measures for sepsis control as achieved at open surgery.
Results
Literature search results
The initial database search returned 208 results. After inspection of titles and abstracts, 41 articles were then retrieved in full-text form for further analysis. Following application of the inclusion criteria, a total of 15 studies comprising 49 patients were included in the final dataset (Fig. 1).

MOOSE flow diagram. MOOSE, Meta-analyses Of Observational Studies in Epidemiology.
Study demographics
The included studies comprised 5 retrospective cohort studies and 10 case reports. Four articles described operative management with endoscopic stents, one which also included a laparoscopic washout of abdominal contamination, seven studies reported outcomes for thoracoscopic repairs, three studies focused on laparoscopic approaches to perforation management, and one study used conservative measures with drainage of sepsis only (Table 1).
Demographic Details of Included Studies
NOS scores for cohort studies only.
NOS, Newcastle-Ottawa scale; VATS, video-assisted thoracoscopic surgery.
Local case series
Our local case series included 4 patients treated between June 2018 and December 2019. Patients had a mean age of 61 years (range 54–72 years) with 3 males and 1 female patient (Table 2). Two patients had known alcohol dependency with 1 having a background of atrial fibrillation. The remaining 2 patients had no significant comorbidities.
Patient Demographics and Outcomes for Minimally Invasive Thorascopic Approach at Our Center
ASA, American Society of Anaesthesiologists; ITU, intensive therapy unit; LOS, length of stay.
Median operative time was 180 minutes (range 160–285 minutes), with a median length of stay in intensive therapy unit of 10 days (range 1–18 days) and an overall median hospital length of stay of 26 days (range 20–35 days). The overall morbidity rate was 50%, both of which were Clavien-Dindo grade II—1 patient was diagnosed with a myocardial infarction on day 2 postoperatively, a further patient suffered a postoperative brachiocephalic vein thrombosis, both were treated medically. There were no reported mortalities and overall treatment success rate was 100% with no further surgical intervention required.
Endoscopic repair
Three articles described endoscopic repairs of esophageal perforations in 7 patients with the use of self-expanding stents placed across the identified esophageal defects during gastroscopy.5,20,21 A single case report described the use of endoscopic clips to close the identified esophageal defect. 6
Darrien and Kasem reported a case series of 5 patients treated between 2008 and 2010 who, having been assessed as being too frail or unwell for the authors' preferred approach of thoracotomy, were managed endoscopically with stents or via VATS. 5 In this series, none of the 5 patients achieved success with the initial treatment strategy, with 1 in-hospital mortality. Two patients underwent VATS drainage of unresolving sepsis, and 1 underwent a laparotomy for management of persistent mediastinal collection.
The three remaining studies were single case reports, with Cayci et al. describing a successful case of endoscopic stenting and simultaneous laparoscopic exploration with washout of abdominal contamination in a 59-year-old female patient. 20 Postoperatively the patient required further percutaneous drainage of bilateral pleural effusions but recovered.
Pinto et al. report the successful endoscopic stenting of an esophageal perforation in a 94-year-old male. A postoperative pleural effusion was managed with antibiotics. 21
Rokszin et al. describe the use of endoscopic clips and feeding jejunostomy in a 53-year-old gentleman diagnosed with a spontaneous esophageal perforation following forceful emesis. 6 There were no reported complications, and the patient was discharged on day 14 postendoscopic intervention.
Thoracoscopic repair
Thoracoscopic repair was reported in 7 articles with outcomes for a total of 37 patients. Cho et al. and Nakano et al. presented retrospective cohort studies comparing thoracoscopic and thoracotomy management strategies.10,22 Okamoto et al. reported a retrospective cohort study comparing outcomes for thoracoscopic management with the addition of perioperative administration of sivelestat sodium hydrate. 23 Elliott et al. presented the results of a retrospective cohort study of patients managed thoracoscopically with either primary defect closure or use of a T-tube. 24
The remaining three articles were single case reports. While techniques were similar throughout the studies, involving washout and primary suture repair of the esophageal defect, Fiscon et al. reinforced their suture line with a pleural flap in the management of their included patient. 25
Cho et al. describe thoracoscopic closure in 7 patients presenting over a 6-year period. 10 Thoracoscopic closure was the treatment of choice for included patients, but they were required to be hemodynamically stable, otherwise thoracotomy was performed. Morbidity rate was 29% with 1 patient found to have a postoperative leak on gastroscopy, which was managed conservatively. Treatment success rate was 100% with a median length of stay of 37 days (range 13–73 days).
Nakano et al. report outcomes for 6 patients who underwent successful thoracoscopic management between 2002 and 2014. 26 Morbidity rate was 67%, with 3 patients having postoperative pneumonias managed with antibiotics and 1 patient having a persistent leak, managed conservatively with resumption of oral intake delayed for a further 7 days until defect closure was confirmed.
Okamoto et al. present outcomes for 11 patients who underwent thoracoscopic closure with thoracoscopic drainage over a 12-year period (2002–2014). 23 Six of these patients also received postoperative intravenous sivelestat sodium hydrate. Morbidity rate was 82% with 4 patients having pneumonias, 4 patients have postoperative collections, and 1 patient having a suture line leak. Treatment success was 100% with a median length of stay of 22 days (range 10–75).
Elliott et al. discuss results of 10 patients managed thoracoscopically at a single center between 2012 and 2018. 24 Eight patients underwent thoracoscopic closure of the esophageal defect and 2 patients with large defects had closure over a T-tube. Morbidity rate was 100% with 6 patients (60%) requiring radiological drainage of postoperative pleural effusions, 5 patients developing pneumonia and atrial fibrillation, and 1 patient developing an esophageal stricture requiring dilation during the follow-up period. There was one mortality from a patient who developed nonocclusive mesenteric ischemia.
Case reports by Fiscon et al., Nakano et al., and Scott and Rosin described successful thoracoscopic single-patient case reports in 79-year-old, 57-year-old, and 77-year-old males, respectively.22,25,27
Laparoscopic repair
Laparoscopic repair was reported in three case reports. Repair was performed through dissection of the left crus of the diaphragm allowing access to the intrathoracic esophagus followed by laparoscopic suturing of the identified defect.
Landen and El Nakadi reported the use of laparoscopic repair in 3 patients, but 2 patients were excluded as these were for delayed presentations. 28 The included patient was a 74-year-old male who required further VATS procedure for extensive debridement and drainage of sepsis, but failed to recover despite aggressive intervention and subsequently died due to multiorgan failure (Tables 3 and 4).
Patient Demographics and Outcomes for Treatment Modalities
LOS, length of stay.
Posttreatment Complications
The case reports by Kimberley et al. and Prosperi et al. present the successful laparoscopic managements of a 35-year-old female and a 53-year-old male, respectively.7,29. Kimberley et al. report a postoperative pleural effusion managed with further antibiotics in their included patient (Table 4).
Study quality
The overall quality of the included studies was very low. Median Newcastle-Ottawa scores for the five included cohort studies was 6 (range 4–7) with the remaining studies being case reports.
Discussion
This systematic review and case series suggest that the use of minimally invasive techniques for the operative management Boerhaave's syndrome may have advantages over traditional thoracotomy. While previous reviews have reported a 20%–40% mortality and high morbidity rate for Boerhaave's syndrome, the limited data presented here demonstrate a significant (68%) morbidity rate, with only one mortality and a 98% treatment success rate with a thoracoscopic approach to achieve debridement and toilet, thoracic drainage, and enteral nutrition. 4 These outcomes must be considered in the context of the low quality of evidence presented here, but suggest that, at a minimum, such an approach is potentially safe and feasible.
Compared to open surgery, it has been suggested that minimally invasive emergency surgery may demonstrate improvements in postoperative pain and surgical inflammatory response, with improved outcomes, as has been demonstrated in elective surgery.30–32
Published accounts of managing Boerhaave's syndrome reflect the wide spectrum with which this condition may present, ranging from a small contained perforation, to a large defect with gross contamination and profound sepsis. A number of publications describe the conservative or solely endoscopic management of Boerhaave's syndrome, including the use of over-the-scope-clips, stents, or endoscopically sutured closure.1,4,33 In almost all cases, however, these reports describe patients with locally contained perforations, with minimal contamination or systemic septic response, and where nonsurgical management was therefore deemed appropriate. For patients with uncontained perforations or systemic signs of sepsis, early diagnosis and surgery with source control remains the primary principle for management.
The treatment success seen in our small cohort without the need to perform primary closure of the esophageal defect reinforces the primary aim of sepsis drainage in management of these patients. This is supported by Vogel et al., who reported on a cohort of 47 spontaneous esophageal perforations, with 100% success rate in esophageal defect healing in patients managed without primary closure. 34 The postoperative leak rate from the included studies reporting on thoracoscopic repair of the esophageal defect was 11% (4/37), with all leaks successfully managed without further surgical intervention, supporting our approach of sepsis drainage without defect closure.
The severe contamination and septic response, which is often present in Boerhaave's syndrome, means that there was a significant rate of postoperative infective complication (53%, 23/43). In most reports, identified collections were managed conservatively with antibiotics (40%, 4/10), or with further drainage procedures or thoracoscopic washout (40%, 4/10). Only 2 patients (20%, 2/10) required salvage thoracotomy, suggesting that initial treatment failure can potentially be treated with further minimally invasive attempts. Where this fails, formal thoracotomy may still be required.
Selection of patients for treatment modality was variable in the reports included in this review. Establishing thoracoscopic access can be achieved in less time than it takes to perform a thoracotomy and is achieved with the patient in the same left lateral position. Low or very low thoracoscopic pressures (≤5 mmHg) should be used, with either isolated single-lung ventilation or low tidal volume dual-lung ventilation, in discussion with anesthetists and their preferred practice. The lack of thoracotomy and reduced postoperative pain mean that routine analgesic adjuncts such as epidurals or paravertebral catheters may be omitted, aiding postoperative mobilization and recovery. 14 Initial patients in our unit were also discussed preoperatively with a thoracic surgeon, and we would encourage a similarly multidisciplinary approach for units considering a transition from open to thoracoscopic approach in such cases.
de Schipper et al. proposed a treatment algorithm for Boerhaave's syndrome based on a 2009 systematic review. This included endoscopic and conservative management approaches for patients with delayed presentations. For acute presentations, this algorithm proposed thoracotomy with washout, with laparotomy and hemifundoplication. 4 Given the evidence presented in this review, we propose an updated version of this algorithm (Fig. 2), which prioritizes a thoracoscopic approach for surgical management. Treatment approaches should take into account patient comorbidities, available surgical and anesthetic skills, and local hospital resources, which are not discussed in the algorithm.
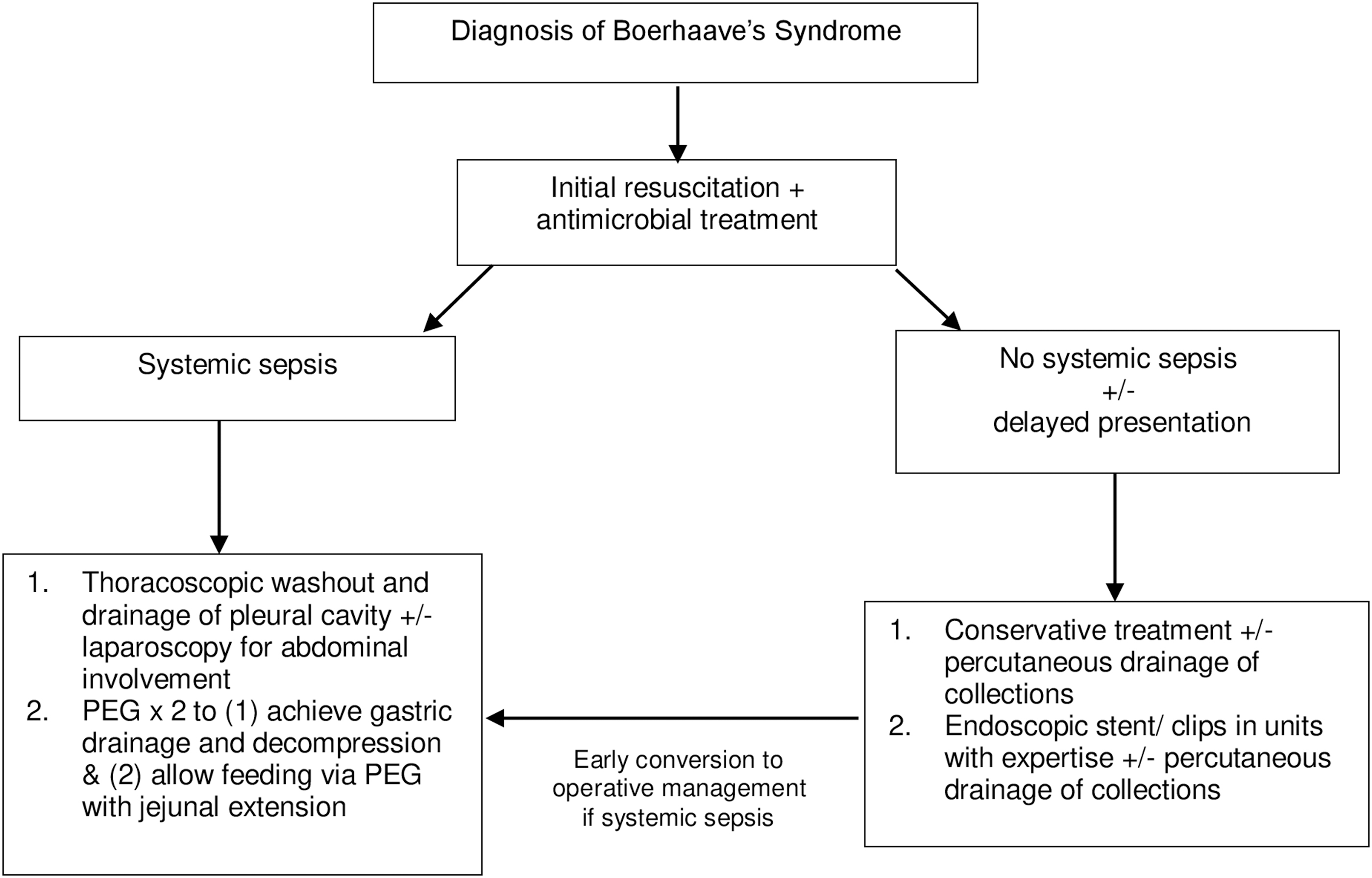
Proposed treatment algorithm for Boerhaave's syndrome.
While the recent World Society of Emergency Surgery (WSES) guidelines suggest reserving a nonoperative approach to patients without systemic sepsis diagnosed within 24 hours, there is evidence that delayed presentations can be managed without surgery.34–36 Vogel et al. were able to perform successful conservative management in 68% of patients, including both early and delayed presentations, with a mortality rate of 6%. 34 Cameron et al. concluded that for patients with minimal signs of sepsis when contamination is well drained, nonoperative management with antibiotics can be a treatment of choice. 37 This has since been debated in a number of more recent studies showing high mortality rates for nonoperative approaches.38,39
Successful endoscopic repair with stents or clips together with drainage of pleural contamination has been reported in patients with contained collections and minimal signs of sepsis, but current guidelines suggest caution with this approach.1,35,40 Laparoscopic approaches may be considered in management of a free perforation of the abdominal esophagus to allow adequate debridement of necrotic tissue. This approach also allows formation of a feeding jejunostomy, although a percutaneous endoscopic gastrostomy with jejunal extension was the preferred method of feeding at our unit. 35
The findings of this review must be interpreted in the context of its limitations. The uncommon nature of Boerhaave's syndrome is reflected in the paucity of data on the topic. Given that currently less than 10% of all emergency laparotomies in the United Kingdom are performed laparoscopically, it is unsurprising that the data on minimally invasive emergency thoracotomy for Boerhaave's syndrome are sparse. 41 The evidence reviewed here represents low-quality retrospective case series or single case reports. Inherent publication bias should be presumed, and it is likely that true success rates for thoracoscopy are lower, and morbidity rates higher, than presented here. However, we believe that these data are sufficient to establish thoracoscopy as a feasible and safe consideration, and have adopted it as a viable treatment option in our unit, with excellent results in a limited number of patients. Prospective trials and disease registries would aid future treatment of this patient group and should be considered and long-term patient results monitored.
In summary, we believe that this systematic review of observational studies illustrates the safety and potential efficacy of minimal invasive approaches in the management of Boerhaave's syndrome.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.