
Abstract
Background:
Hiatal hernia repair (HHR) is a complex surgical procedure and its management is not standardized. Several meta-analyses have compared cruroplasty with hiatus reinforcement with mesh, and crura augmentation appears to have better outcomes. However, heterogeneity in type of mesh and placement techniques has differed significantly.
Materials and Methods:
A systematic review and network meta-analysis were carried out. An electronic systematic research was carried out throughout Pubmed, CENTRAL, and Web of Science, of articles analyzing HHR with cruroplasty, nonabsorbable mesh (NAM), and absorbable mesh (AM) reinforcement.
Results:
Seventeen articles based on 1857 patients were enrolled in this article. The point estimation showed that when compared against the control group (NAM), the HH recurrence risk in AM and cruroplasty group was higher (relative ratio [RR] 2.3; CrI 0.8–6.3, RR 3.6; CrI 2.0–8.3, respectively). Postoperative complication rates were alike in all groups. The prevalence of mesh erosion after HHR is low.
Conclusions:
This network meta-analysis showed that prosthetic reinforcement significantly reduced HH recurrence when compared with cruroplasty alone. However, there is not enough evidence to compare different mesh compositions.
Introduction
Gastroesophageal reflux disease is complex disorder and in select cases requires surgical management. 1 For complex hiatal hernia, laparoscopic hiatal hernia repair (HHR) with concomitant fundoplication is often needed. HHR is a highly technical procedure and is best performed by someone with advanced upper gastrointestinal training. 2 The common long-term complication after HHR is recurrence, with rates ranging from 12% to 42%. 3 For this reason, several randomized controlled trials (RCTs) attempted to clarify whether reinforcing cruroplasty with a mesh could significantly reduce recurrence. To date, some early trials produced promising results.4–6 In addition, several meta-analyses have confirmed the superiority of the prosthetic reinforcement over cruroplasty.7,8 But, the nonabsorbable mesh (NAM) placement was related with serious complications, such as mesh erosion into the esophagus or stomach. 9 Therefore, surgeons started using absorbable meshes (AM) as an alternative option. 10 AMs could be either synthetic such as Vicryl® (Ethicon, Somerville, NJ) and Bio-A® (Gore Medical, Newark, DE), or biological mesh such as AlloDerm® (Allergan PLC, Dublin, Ireland), Strattice™ (Allergan PLC) or Surgisis® (Cook Medical, Bloomington, IN). Although several studies showed that AM placement is both feasible and effective, there remains inconsistent data on their long-term efficacy, especially as they are associated with higher costs. 10 This review aimed to compare through network meta-analysis the short- and long-term surgical complications after HHR with NAM and AM reinforcement.
Materials and Methods
Search strategy
A systematic review was carried out following the guidelines from the preferred reporting items for systematic reviews and meta-analyses checklist (PRISMA-NMA). 11 We performed an electronic systematic research throughout MEDLINE, CENTRAL and Web of Science in keeping with Goossen et al. 12 We retrieved articles published in English up to February 2020. We used the following search headings: (“hiatal hernia repair” [tiab]) AND (“mesh reinforcement” [tiab] OR “mesh placing” [tiab] OR “prosthetic reinforcement” [tiab]) AND (“cruroplasty” [tiab] OR “crura augmentation” [tiab]) AND (“nonabsorbable mesh” [tiab] OR “absorbable mesh” [tiab] OR “synthetic mesh” [tiab] OR “biological mesh” [tiab]). All titles were screened and relevant abstracts were reviewed. Ultimately, each of the acceptable publication reference section was checked for other possible articles. The protocol of this study is available at the National Institute for Health Research/Prospero website, registration number CRD42020176008.
Inclusion/exclusion criteria
In agreement with Stroup et al. only RTCs or non-controlled clinical trials (non-RCTs) were enrolled in this research. 13 The studies had to meet the following criteria to be enrolled: (1) patients have had HHR; (2) studies have compared one or more HHR surgical technique with mesh (AM or NAM) or cruroplasty alone; (3) COMPOSITE meshes were excluded; and (4) studies have clear research methodology.
Data extraction
The enrolled data were extracted from the selected articles and entered in two independent databases form by 2 investigators (F.B. and E.R.): author, study year, country, study design, patients, gender, age, body mass index (BMI), and follow-up data. The databases were compared at the end of the reviewing process to decrease the selection bias. Finally, a third author (A.B.) reviewed all data.
Study quality assessment
The Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool 14 was use to appraise the risk of bias. It categorizes risk of bias as low, moderate, serious, critical, and unclear. In case a study was categorized with a risk of bias serious, critical, or unclear, the effect of erasing this article was tested and the significant outcome(s) recorded. RCTs were assessed using the Cochrane risk-of-bias tool. 15 Trials were categorized as L = low risk, H = high risk, and U = unclear risk. The quality of studies is illustrated in Table 1.
Quality Assessment of the Included Studies
Each domain is evaluated with one of the following: y “yes,” py “probably yes,” pn “probably no,” and n “no.” The categories of judgment for each study are low, moderate, serious, and critical risk of bias.
The quality of observational studies was performed using ROBINS-I tool.
The quality of the randomized clinical trials was assessed by Cochrane risk of bias tool (L = low risk, H = high risk, U = unclear risk). 1 = random sequence generation; 2 = allocation concealment; 3 = blinding of participants and researches; 4 = blinding of outcome assessment; 5 = incomplete outcome data; 6 = selective reporting; 7 = other bias.
ROBINS-I, Risk of Bias In Non-randomized Studies of Interventions.
Statistical analysis
This fully Bayesian random effect contrast-based network meta-analysis used relative ratio (RR) as pooled measure. A consistency generalized linear model as described in the NICE-DSU technical support document 2 was fitted. 16 We used a vague prior distribution for the RR. 17 For the between-study variability (τ) we adopted an informative half-normal prior distribution with mean and scale equal to 0 and 1 (scale = 0.5 as prior sensitivity analysis), respectively, assuming a common heterogeneity across the various treatment comparisons. 18 The local inconsistencies was investigated using the node split. We used median and relative 95% credible intervals (CrI), based on draws from marginal posterior distribution in Monte Carlo Markov chain, simulating 350,000 iterations after a burn-in period of 30,000 iterations. We judge statistically significant when the 95% CrI encompasses null hypothesis value. The convergence of Markov chain Monte Carlo (MCMC) algorithm was checked using running means, MCMC-error, and statistics included into R/Boa package. 19 To assess transitivity, we computed descriptive statistics and compared the distributions of baseline characteristics across studies. We also adopted the confidence in network meta-analysis (CINeMA). 20 All statistics analysis were computed using Jags and R-Cran softwars.21,22
Outcomes of interest
The outcomes of interest to assess and compare NAM with AM in patients undergoing HHR were overall postoperative surgical complications, mesh erosion, and HH recurrence.
Results
Literature search and study characteristics
Seven hundred eighty-six articles were retrieved. Once the duplicates were removed, 178 articles were further examined. Ultimately, 17 articles4–6,23–36 met the study's inclusion criteria. Six studies were prospective,23,24,26,27,30,31 three studies were retrospective,25,28,29 and eight studies were randomized control trials (Fig. 1).4–6,32–36
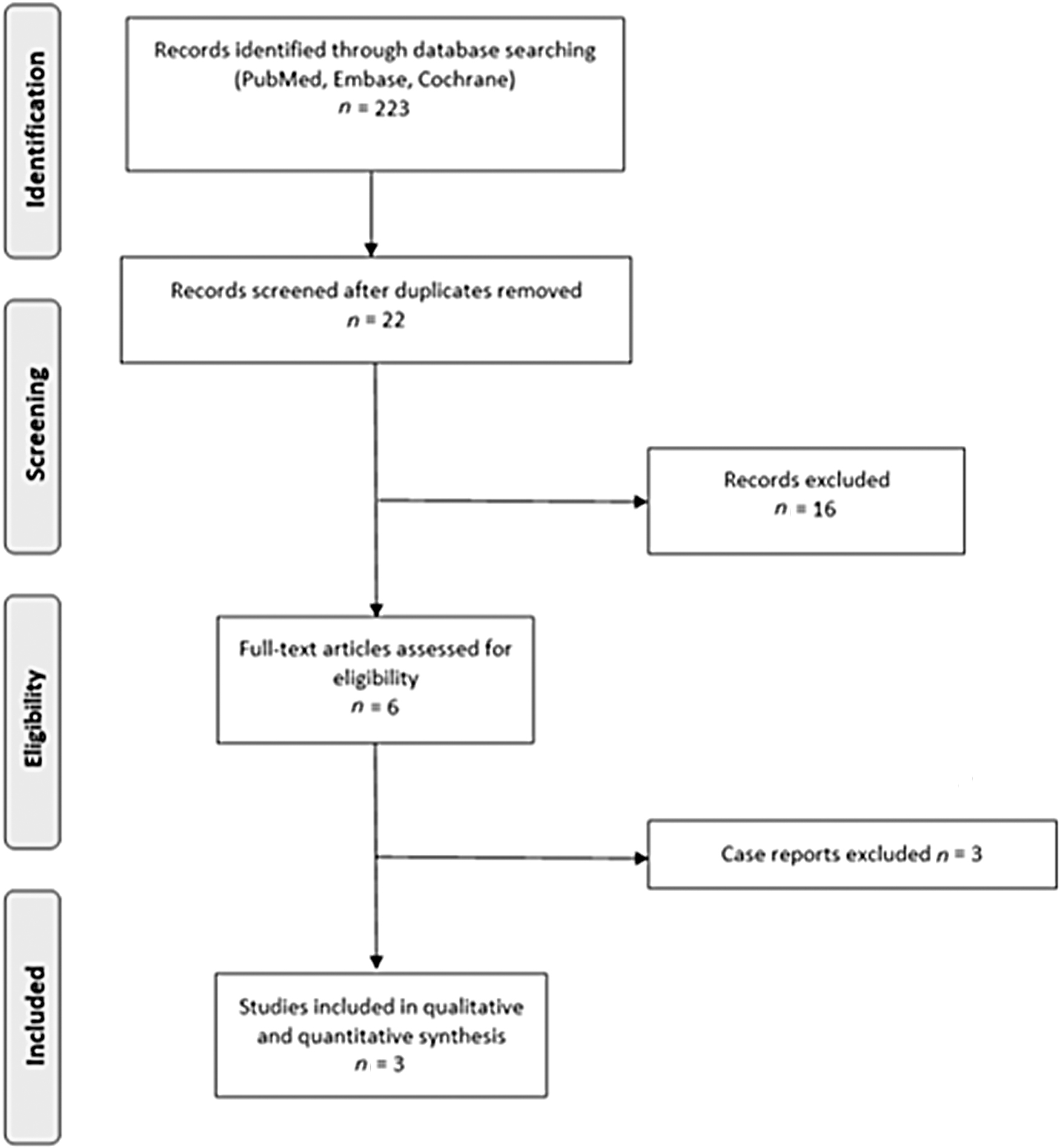
Flowchart of studies retrieved from literature search.
Patient characteristics
One thousand eight hundred fifty-seven patients were included. Nine hundred sixty-four patients (51.9%) were in the cruroplasty group, 582 patients (31.3%) in NAM, and 311 patients (16.8%) in AM group. Six hundred eighty-five (46.7%) were male and 781 (53.3%) were female. The median age was 58.2 years (range 48–72 years) and the median BMI 28.5 kg/m2 (range 26–31 kg/m2). Median follow-up was 19 months (range 9–54 months) (Table 2). Hernia recurrence was proven by both endoscopy and barium meal in seven studies,4,6,26,27,29,35,36 only barium meal in five,5,24,25,28,31 only endoscopy in four,30,32–34 and in one 23 the examination was not outlined.
Demographic Characteristics of Patients in the Three Groups
AM, absorbable mesh; NAM, nonabsorbable mesh.
Hiatal hernia recurrence
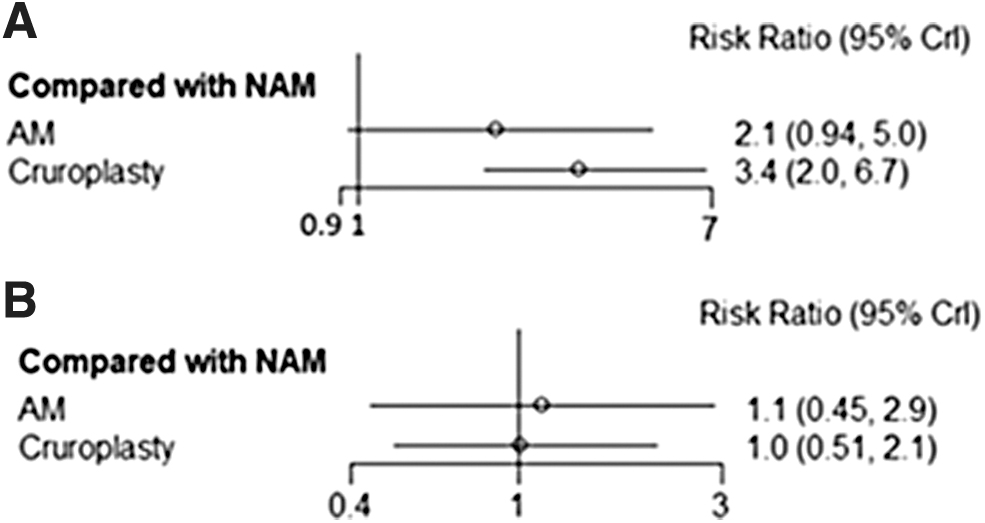
The point estimation showed that when compared with the control group (NAM), the HH recurrence risk in AM and cruroplasty group was higher (RR 2.3; Crl 0.8–6.3, RR 3.6; Crl 2.0–8.3, respectively) (Fig. 2a). A rank plot illustrating empirical probabilities for NAM with each assessment ranked first through third (left to right) is provided in Figure 3a. Table 3 is a league table showing all pairwise comparisons in the network meta-analysis. The global heterogeneity was zero (range 0.0%–32.4%). The node split did not show evidence against inconsistency.
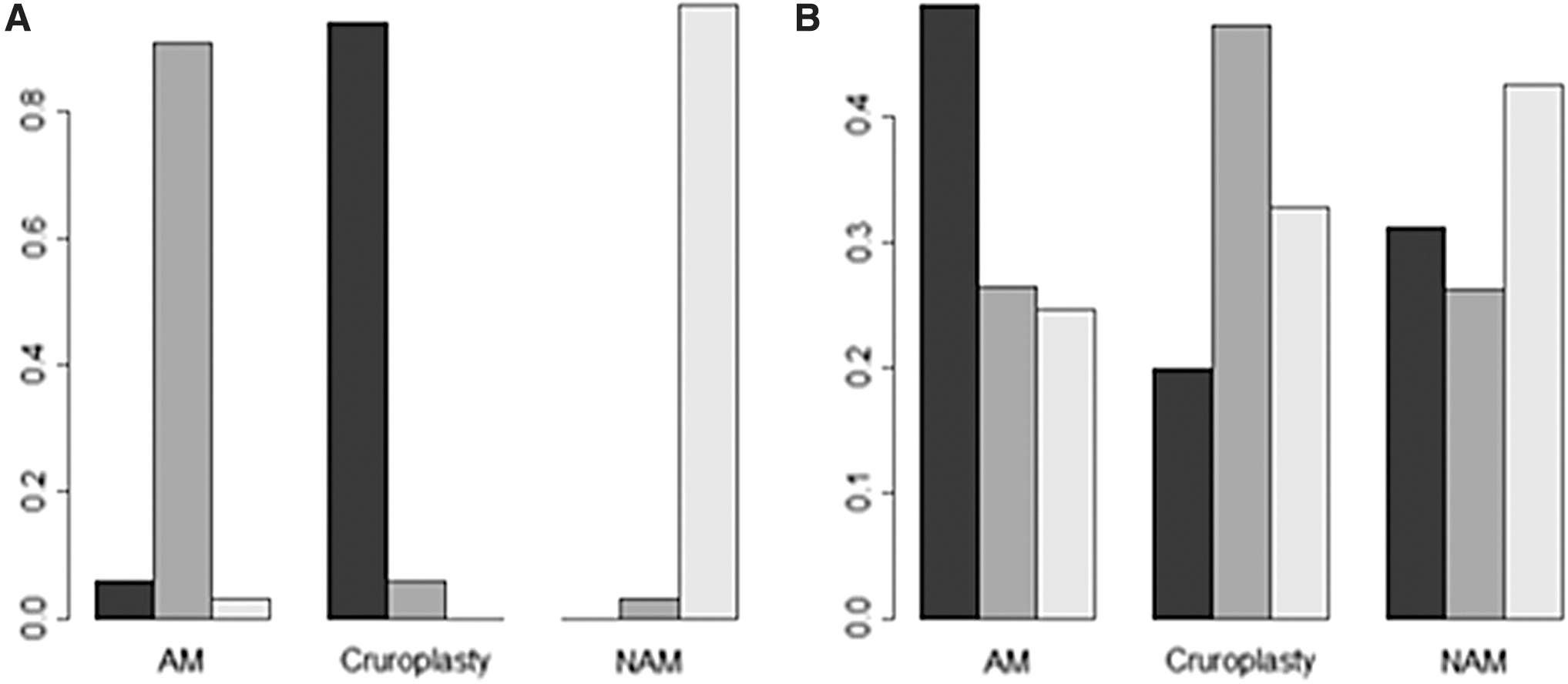
Rank plot created using the rankogram function from the gemtc R package applied to the three groups illustrating empirical probabilities that each treatment is ranked first through third (left to right) for
League Table for HH Recurrence
HH, hiatal hernia; AM, absorbable mesh; NAM, nonabsorbable mesh.
Overall complication rate
The point estimation showed that when compared with the control group (NAM), the postoperative complication rate was similar to both AM (RR 0.9; Crl 0.3–2.3) and cruroplasty group (RR 0.8; Crl 0.4–1.7) (Fig. 2b). A rank plot illustrating empirical probabilities for NAM with each assessment ranked first through third (left to right) is provided in Figure 3b. Table 4 is a league table showing all pairwise comparisons in the network meta-analysis. The global heterogeneity was zero (range 0.0%–35.2%). The node split did not show evidence against inconsistency.
League Table for Overall Complication Rate
AM, absorbable mesh; NAM, nonabsorbable mesh.
Mesh erosion
To date, there are not enough data for a quantitative analysis. Among the articles screened from the quantitative analysis, only Carlson and Turkcapar27,32 described a mesh erosion in their series. Both cases occurred after HHR with polypropylene mesh and both meshes had a keyhole shape. In 1 patient erosion led to dysphagia. Interval from HHR to onset of symptoms ranged from 7 days to 29 months.
Discussion
To date, five meta-analyses were published comparing HHR with cruroplasty and mesh reinforcement.7,8,37–39 Four studies included all the different types of mesh (i.e., AM and NAM),7,8,37,38 whereas Campos et al. only compared NAM versus cruroplasty. 39 In all these meta-analyses, the mesh group seems to slightly reduce HH recurrence, while maintaining a similar postoperative complication rate. This is the first network meta-analysis that both directly and indirectly compares AM and NAM reinforcement during HHR. To the best of our knowledge, only Watson et al. offered data on postoperative surgical outcomes directly comparing two different types of mesh. This study showed that there were no differences between AM and NAM in terms of HH recurrence and postoperative complication rate. The results from this study are similar to those of Watson et al. 6 ; in fact, we found that NAM group had the lowest recurrence rate in terms of HH recurrence when compared with the other two surgical techniques. However, the network meta-analysis did not show any differences among the three surgical techniques in terms of overall surgical complications. Specifically, we attempted to meta-analyze if specific meshes have higher postoperative complications such as erosion, but the numbers are low in incidence for meaningful analysis.
From a qualitative analysis, it seems that mesh erosions are more common with NAMs. Examining the literature, Li and Cheng carried out an interesting systematic review whose search was predominantly based on case series and case reports. They found 50 cases of mesh erosions and noted that it was more likely to happen after redo surgery, or with the use of polytetrafluoroethylene (PTFE) and polypropylene meshes. 9
Ultimately, the real incidence of mesh erosion after HHR is rare, and factors such as patient characteristics (adiposity), surgical skills and mesh material seem confounding factors. These factors also play a role in other mesh-related complications such as shrinkage, infection, or stenosis of the esophageal hiatus.
HHR technique remains poorly standardized, due to the variations in HH conformation, size, and patient-related factors. In this context, the NAMs, which were more widely available than AMs, were initially used to reinforce the hiatus. However, first model of NAMs were stiff and not malleable especially in abnormal HH anatomy. More modern NAMs are lighter and more flexible, facilitating easier placement. It has been postulated that dysphagia after mesh placement is another problem, and is likely due to esophageal dysmotility. Concomitant fundoplication during HHR may be a causative factor. Nason et al. found that dysphagia was highly related to the esophageal angulation and, particularly, to Collis gastroplasty, which was more commonly performed in patients with mesh reinforcement. 40
This review has some limitations. First, we only included abstracts in English and that the overall numbers regarding recurrence and morbidity are low in incidence. Second, there is heterogeneity regarding hiatal hernia size and skillset of operator experience. However, this is the first network meta-analysis to show that prosthetic reinforcement (both NAM and AM) significantly reduced HH recurrence when compared with cruroplasty alone, without considerable increased morbidity.
Disclaimer
This article is containing original research and has not been submitted/published earlier in any journal and is not being considered for publication elsewhere.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.