
Abstract
Background:
This study aims to consolidate all available articles on this topic and evaluate MSA effectiveness in the management of gastroesophageal reflux disease (GERD).
Matherials and Methods:
We conducted an electronic systematic search using MEDLINE databases (PubMed), EMBASE, and Web of Science. An electronic systematic search of articles comparing preoperative and postoperative health-related quality of life (GERD-HRQL) scores in patients who underwent MSA placement for management of GERD following bariatric surgery was performed. Three retrospective studies totaling 33 patients met the inclusion criteria and were included in this meta-analysis.
Results:
The pooled mean difference in change from preoperative GERD-HRQL score was 17.5 (95% CrI; −22.88 to −12.20) and it was statistically significant. The between-study variability is 3.621 (95% HPD; 1.39 4.99) with low heterogeneity (I2 = 15%; 95% HPD; 2.1 26.2%).
Conclusions:
MSA for refractory GERD following bariatric surgery appears feasible. Prospective randomized controlled with standardized surgical technique and objective follow-up evaluation is needed to better assess short- and long-term efficacy
Introduction
Bariatric surgery has become crucial in the management of patients with obesity, given the effects on weight loss and reduction of obesity-related comorbidity rate. 1 To date, laparoscopic sleeve gastrectomy (LSG) and Roux-en-Y gastric bypass (RYGB) are the commonest bariatric surgical procedures performed worldwide, with acceptable morbidity. 2 Tai et al. showed that gastroesophageal reflux disease (GERD) prevalence is increased among bariatric populations. 3
While RYGB seems to control pre-existing GERD and mitigate further GERD symptoms, LSG appears to be less effective to mitigate those symptoms. 4 A recent systemic review showed both LSG and RYGB improved quality of life, but LSG had minimal effect on GERD. 5
Proton pump inhibitors and H2 blockers are the initial treatment for patients suffering from GERD following bariatric surgery; however, in a minority of them, medical therapy is ineffective and surgery may be necessary. 6 However, given that these patients have had prior gastric surgery, fundoplication is very often not technically possible. A possible option in some instances is converting an LSG to RYGB. 7 Alternatively, a magnetic sphincter augmentation (MSA) placement is a promising alternative. 8 Since the current evidence focusing on MSA for intractable GERD following bariatric surgery is limited, this study aims to assimilate the current evidence on the effectiveness of MSA.
Materials and Methods
Search strategy
A systematic review was carried out according to the guidelines from the preferred reporting items for systematic reviews and meta-analyses checklist (PRISMA). 9 Institutional review board approval was not required. We conducted an electronic systematic search using MEDLINE databases (PubMed), EMBASE, and Web of Science. Last date of research was April 25, 2020.
We used the following search headings: bariatric surgery, laparoscopic Roux-en-Y gastric bypass, laparoscopic sleeve gastrectomy, GERD, gastroesophageal reflux disease, GERD-health-related quality of life (GERD-HRQL), LINX, and magnetic lower esophageal sphincter augmentation.
Inclusion/exclusion criteria
The articles had to meet the following criteria publication and report to be included in the analysis: (a) LINX placement for treatment of refractory GERD following bariatric procedures, (b) preoperative and postoperative GERD-HRQL scores were reported, (c) written in English, (d) have clear research methodology, and (e) data overlapped with other studies included were excluded.
Data extraction
The following data were retrieved from the selected publications and entered in a data extraction form by two investigators (R.M. and E.R.): author, study year, period of study, country, study design, patients, gender, age, body mass index (BMI), comorbidities, and preoperative and postoperative GERD-HRQL score. All data were entered independently by both investigators in two separate databases and only compared at the end of the reviewing process to reduce the selection bias. Finally, a third person (A.L.) reviewed the database. Duplicates were erased and the discrepancies were clarified.
Study quality assessment
Assessment of risk of bias of included studies was performed using the risk of bias in nonrandomized studies of interventions (ROBINS-I) tool, 10 which categorizes risk of bias as low, moderate, serious, critical, and unclear, with the risk of bias category for each study being reported. If a study's risk of bias was categorized as serious, critical, or unclear, the effect of removing this study was tested and the relevant outcome(s) reported. The quality of all included studies is depicted in Table 1.
Quality Assessment of the Included Studies
The quality of observational studies was performed using ROBINS-I tool. Each domain is evaluated with one of the following: y “yes,” py “probably yes,” pn “probably no,” and n “no.” The categories of judgment for each study are low, moderate, serious, and critical risk of bias.
Statistical analysis
We performed fully Bayesian random-effect meta-analysis. Compared to the frequentist meta-analysis, the Bayesian approach considers all sources of variations, reflects these variations in the pooled result, can provide accurate estimates for small samples, and allows computation of predictive distribution. Besides, Bayesian posterior analysis should yield exact coverages, independent of sample size. 11 We fitted an adapted statistical model following Abrams et al., 12 considering single-arm study design, to estimate pooled mean difference in change from baseline (preoperative), relative to GERD HRQL score. For the overall mean difference in change (μ), we imposed a noninformative Normal (−21,10) prior, based on Schwameis. 13 For the between-study variability (τ) and for potential within-subject correlation (ρ), we considered a noninformative Uniform (0,5) 14 and a Uniform (0,1) priors, respectively, assuming a positive correlation. A noninformative positive half-Normal (0,10) prior has been used as prior sensitivity analysis. We considered the heterogeneity according to Higgins. 15 The inference was performed using median and relative 95% credible (CrI), 95% highest posterior density (HPD), and 95% prediction intervals, based on draws from marginal posterior distribution in Monte Carlo Markov chain, simulating 300,000 iterations after a burn-in period of 30,000 iterations. We consider the estimated parameter statistically significant when its 95% CrI (or HPD) encompasses null hypothesis value (0.00). The accuracy of the inference was assessed by convergence of MCMC algorithm, checked using graphical inspection of running means, MCMC error, and diagnostic statistics included into R/Boa package. 16 Statistical analyses were carried out using NIMBLE and R-Cran statistical packages.17,18
Outcomes of interest
The outcomes of interest to assess the effectiveness of MSA placement in patients with obesity suffering from GERD following a bariatric procedure were the comparison between preoperative and postoperative GERD-HRQL scores, the changes for GERD medical therapy, and the analysis of postoperative surgical complications.
GERD health-related quality of life
GERD-HRQL is a validated instrument to provide a quantitative measure of GERD symptoms. 19 It is one of the most frequently used and it has been recommended for use by the European Association for Endoscopic Surgery. 20 The primary purpose in the development of the GERD-HRQL was to measure symptomatic improvement of both medical and surgical treatment for GERD. The questionnaire has a total of 10 questions rating from 0 (absence of symptoms) to 5 (severe symptoms) for a total score that ranges from 0 to 50. Symptoms are defined as absent if the score is 0, mild from 1 to 15, moderate from 16 to 30, and severe from 31 to 50.
Results
Literature search and study characteristics
One hundred and twenty-three publications were found using the search criteria. After removing duplicates, 22 publications were further examined. Further screening revealed that only three retrospective articles8,21,22 met the predefined inclusion criteria (Fig. 1).
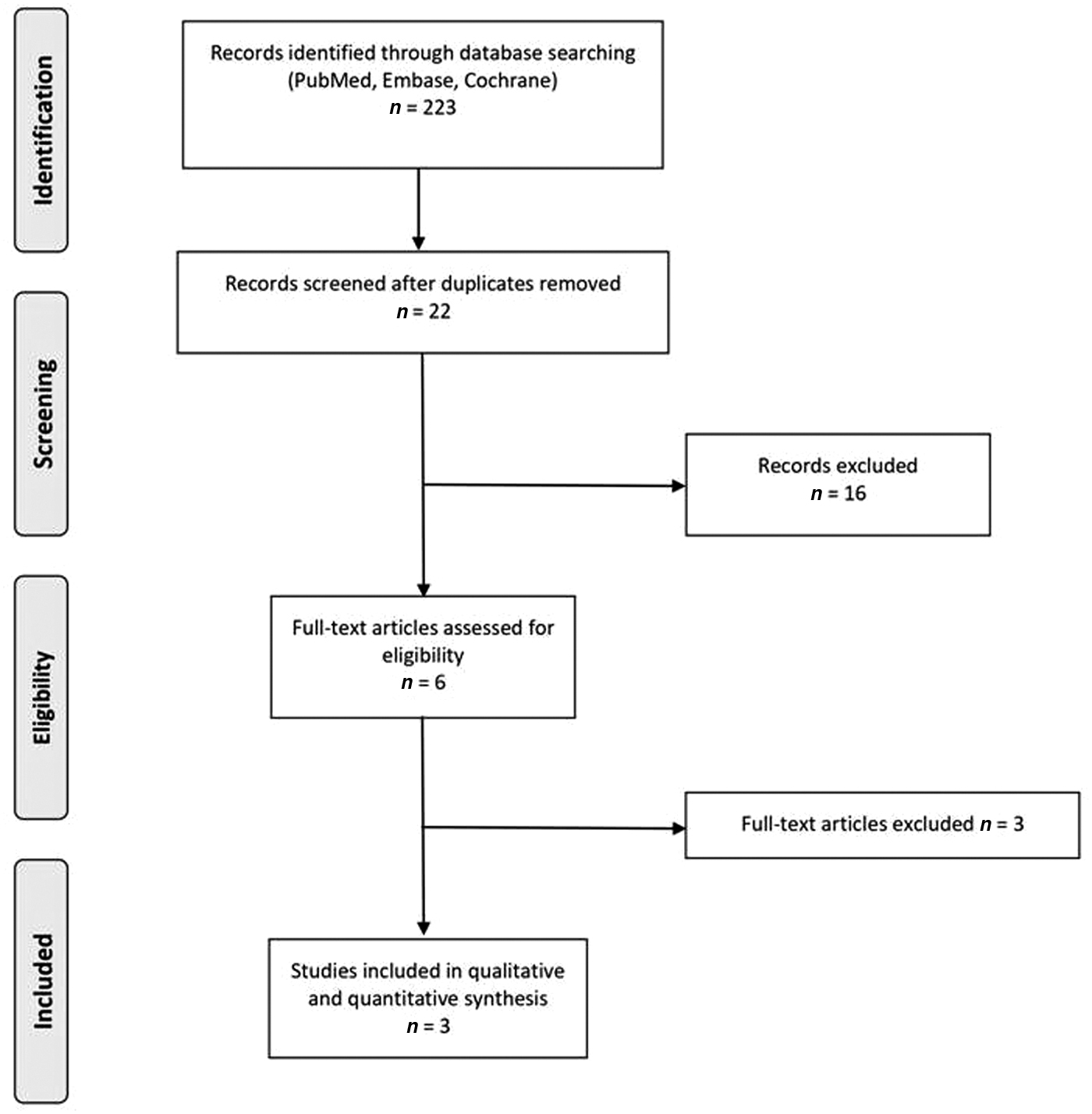
Flowchart of studies retrieved from literature search.
Patient characteristics
Thirty-three patients were included in this analysis. Twenty-nine (84%) underwent LSG, four patients (12%) had RYGB, and one patient (4%) had a duodenal switch. Eleven (33.3%) patients were male and 26 (66.7%) patients were female. The mean age was 48.3 years (IQR 48–72 years) and the mean was BMI 37.6 kg/m2 (IQR 26–31 kg/m2). The mean time between bariatric procedures and MSA placement was 30 months (IQR 18–43 months) (Table 2).
Demographic Characteristics of Patients
Meta-analysis
The pooled mean difference in change from preoperative GERD-HRQL score was 17.5 (95% CrI; −22.88 to −12.20) and it was statistically significant. The Bayesian Forrest-plot is depicted in Figure 2. The between-study variability (τ) is 3.621 (95% HPD; 1.39 4.99), which reflects low heterogeneity (I 2 = 15%; 95% HPD; 2.1 26.2%). The low heterogeneity was supported by the fact that 95% prediction intervals (−24.37 to −11.17) are close to mean difference in change CrI. The estimated within-subject correlation (ρ) was 0.45 (95% HPD; 0.0 0.86). The sensitivity analysis regarding the choice of prior distribution relative to between-study variability showed a small difference in mean difference −14.29 (95% CrI; −20.48 to −11.28). Besides, there was significant reduction of heterogeneity (τ = 0.56 95% HPD; 0.00 1.02; I2 = 0.5% 95% HPD; 2.1 26.2%).
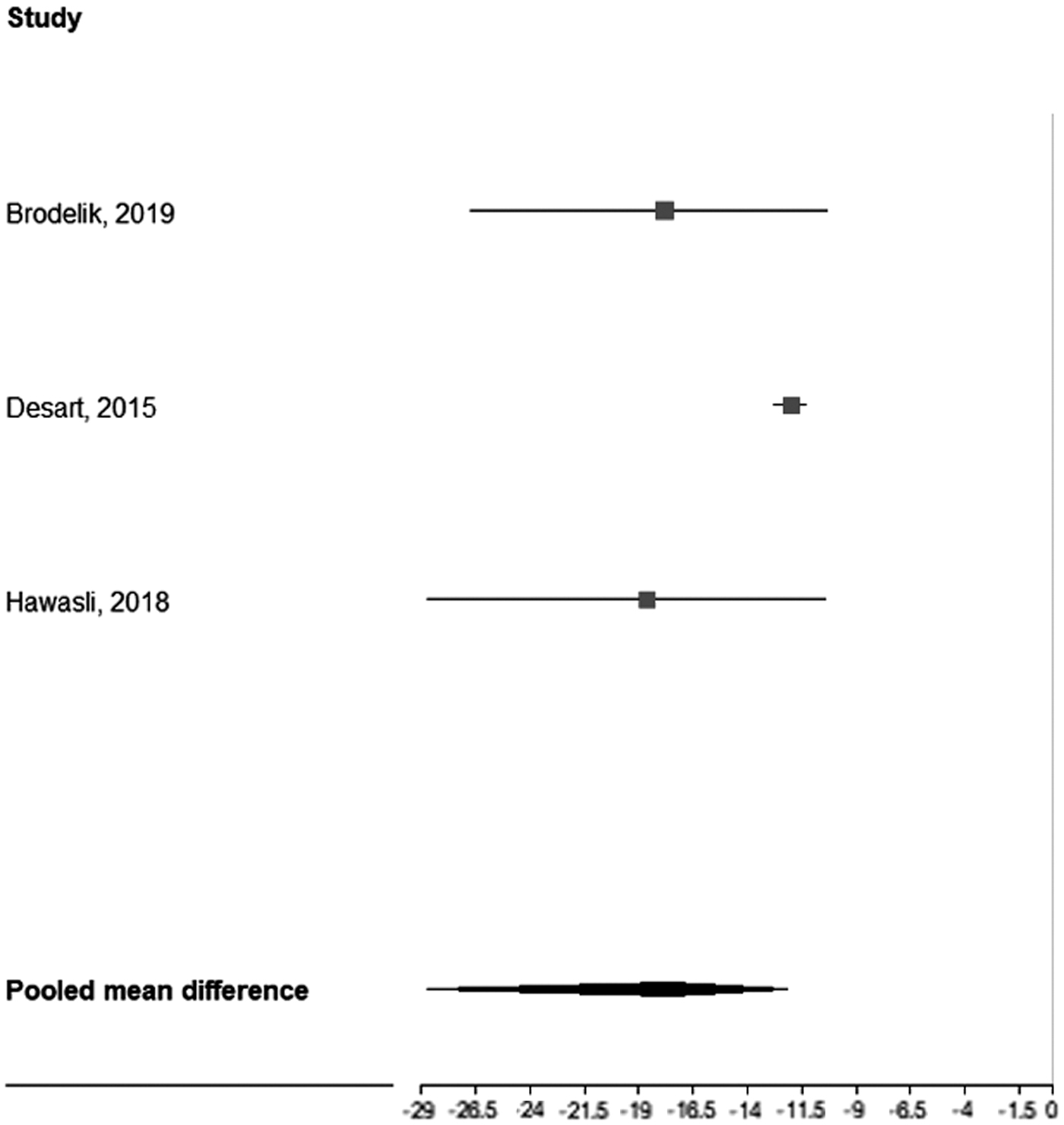
Bayesian Forrest-plot showing the mean difference in change from preoperative GERD-HRQL score with relative shrinkage interval for the study-specific effect. GERD-HRQL, gastroesophageal reflux disease–health-related quality of life.
Discussion
This study seems to support the placement of MSA in selected patients with intractable GERD following bariatric procedures. We observed that it is feasible and effective, resulting on average a reduction of 17 points of the GERD-HRQL score when compared to the preoperative one. GERD is a common comorbid condition seen in all patient populations, but appears to be pronounced in some patients following surgery for obesity management. 23 This finding is related to a spectrum of factors, including increased abdominal pressure, laxity of diaphragm, decreased lower esophageal sphincter pressures, potential esophageal motility disorders, and presence of hiatal hernia. 24 DuPree et al. confirmed the high prevalence of GERD symptoms among patients with obesity undergoing bariatric surgery, with roughly half of them having mild GERD and 25% having severe GERD. 25 Considering the increasing number of bariatric surgical procedures, GERD among patients with obesity cannot be ignored and should be incorporated in the decision-making process in deciding which bariatric surgery is most appropriate. To date, even though only several small studies have reported on GERD following LSG, it seems evident that LSG exacerbates GERD symptoms. In instances, GERD symptoms are intractable to medical treatment, leaving surgery as the only option (converting an LSG to RYGB).
Carter et al. showed that the incidence of developing symptoms of GERD postoperatively in patients with previous asymptomatic GERD ranged from 30% to 51%. 26 A comprehensive literature review recommended that preoperative manometry should be routinely carried out in all patients undergoing bariatric surgery. 27 In a study of 4832 patients having LSG, 70% of them had preoperative GERD. None had resolution of their GERD symptoms postoperatively. Conversely, in 33,867 patients undergoing RYGB, 95% had improvement or stabilization of their GERD symptoms. 25 Langer et al. observed that 11% of LSG patients required revisional surgery. 28
Given that the Food and Drug Administration (FDA) intends a positive response to treatment and a reduction of GERD-HRQL score ≥50% from baseline, 29 and that findings from this study showed a mean GERD-HRQL reduction of 17 points, it seems that MSA placement for recalcitrant GERD following bariatric procedures should be considered for patients preoperatively scoring between 35 and 25 to achieve a resolution of symptoms.
Although this study suggests that MSA placement improved QoL in patients with intractable GERD following bariatric surgery, there is a need for larger-volume data from either randomized controlled trials or international registries to assess mid- to longer-term efficacy, as well as morbidity. 30 The LINX® system (Torax Medical, Inc., Shoreview, MN) has been approved by the FDA from 2012 for the treatment of refractory reflux,31,32 but its role in managing patients with bariatric surgery is still not approved. A recent systematic review focusing on the use of MSA showed that its use in clinical practice is not standardized and its efficacy stills lack robust evidence. 33
We acknowledge that this meta-analysis has several limitations, but we also believe that these limitations reflect the lack of knowledge within the current literature. Current evidence on MSA in GERD following bariatric surgery is only based on preoperative and postoperative GERD-HRQL scores from small retrospective studies. These are limited by patient selection bias and short follow-up.
In conclusion, MSA may be considered in selected patients for intractable GERD following bariatric, particularly those with a GERD-HRQL up to 35. Despite this, initial data suggest that MSA should be considered in selected patients for the management of intractable GERD following bariatric. Prospective randomized controlled trials or multicenter studies with standardized preoperative studies (i.e., impedance-pH monitoring, gastroscopy, and manometry), combined with good QoL and postoperative evaluation, are needed to further assess their continued role in refractory GERD management.
Footnotes
Funding Information
No funding was received for this article.