
Abstract
Background:
Laparoscopic partial splenectomy (LPS) may allow avoiding total splenectomy (TS) complications and maximizing the advantages of mini-invasive approach. The objective of this review is to assess feasibility and safety of LPS, to compare this approach with alternative options.
Materials and Methods:
A literature review of articles reporting LPS is performed. Several parameters, including age, indication, surgical technique, devices used for splenic section/hemostasis, adverse outcomes, including morbidity/mortality, conversions to open surgery, conversions to TS, operative time (OT), and hospital stay (HS), are analyzed. Articles comparing LPS' results with those of open partial splenectomy and laparoscopic TS are also analyzed.
Results:
Fifty-nine articles reporting 457 LPS were included. Patients' characteristics varied widely, concerning age and indications, including hematological disease (hereditary spherocytosis, drepanocytosis), splenic focal masses, and trauma. Several technical options are reported. Mean OT and HS are 128 ± 43.7 minutes and 4.9 ± 3.8 days, respectively. No mortality and 5.7% morbidity are reported. Conversion rates to open surgery and to TS are 3.9% and 3.7%, respectively.
Conclusions:
In conclusion LPS is feasible and safe, with no mortality, low morbidity, and low conversion rates to laparotomy and to TS. LPS may be accomplished by various techniques and tools. Major complications are sporadically reported, thus potential risks should not be underestimated.
Introduction
Since the late 1960s, partial splenectomy (PS) has been introduced1–5 in selected patients to avoid the nonnegligible drawbacks of total splenectomy (TS), including 3.2% rate of severe infections, 6 overwhelming postsplenectomy sepsis, and 0.2%–1.4% mortality.6–8 Since, PS has been proposed for various conditions whenever splenectomy was nonmandatory for oncological or hemostatic reasons, including hematological disease,2,3,9–11 portal hypertension, 12 trauma,13–15 benign,16–18 and malignant19,20 focal lesions.
Although there is the obvious advantage of spleen partial preservation, PS has only slowly spread through the 1990s, and it is still not recognized as an option by most general surgeons.1,21–26 Several factors might have played a role in such a slow spreading of this procedure, including the rarity of conditions suitable of PS, the suboptimal effectiveness of surgical technique/tools used for splenic parenchyma transection/hemostasis, and other technical issues of surgery, including the need of a large laparotomy to obtain an optimal vision of the operating field.
The introduction of laparoscopy and the development of new devices allowing for enhanced visibility and effective splenic parenchyma transection/hemostasis has had a pivotal role in the diffusion of PS during the 1990s and 2000s, as witnessed by the increasing number of performed procedures and published articles on the subject 27 First introduced by Poulin in 1995, who reported the laparoscopic resection of spleen superior pole for trauma after preoperative embolization. 15 Since the early 2000's, laparoscopic partial splenectomy (LPS) is widely spreading and extending its indications.28–30 In 2010, the first robotic PSs were reported by Vasilescu et al. 31
Present literature about LPS procedures is extremely heterogeneous, considering patients, indications, surgical technique, and used devices/tools. Unfortunately, the scientific quality of articles reporting LPS, mostly consisting of case reports and small retrospective case series, is low, with IIIb to V grade of evidence. With the primary aim to allow for a first assessment of technique's feasibility and safety and to give the reader any possible useful information of a spreading but heterogeneously performed technique, in this study, we propose a comprehensive review of the 457 published cases. Secondary aim of the article is to report the comparison between LPS and alternative techniques for splenic resection, namely laparoscopic TS and open PS.
Materials and Methods
Ethics approval
As a narrative review, according to Institutional Review Board approval guidelines, ethics approval is not required.
An extensive bibliographic research of literature according to PRISMA criteria was performed (Fig. 1). Medline, Embase, and PubMed were consulted to identify articles reporting the following items: hemisplenectomy, hemi-splenectomy, polar splenectomy, PS, subtotal splenectomy, and near TS up to December 2018. Those items were then meshed with the Boolean operator “AND” and “OR” with the following mesh terms: laparoscopic, minimally invasive, video-laparoscopic, and mini-invasive. Additional articles were searched by manual identification from the key articles.

Prisma 2009 flow diagram. 106
Inclusion criteria
Articles in English language, reporting LPS in humans and articles reporting laparoscopic procedures together with open or robotic ones were included, but only patients undergoing LPS were considered; in case of multiple articles from the same group of authors, an effort was made to identify duplicate article (LPS procedures were included only one time).
Exclusion criteria
Articles not in English language reporting selectively open or robotic PSs and/or procedures performed in animals.
All articles were reviewed by three different reviewers; any disagreement was debated until a unanimous decision about including or not including the article was reached (Fig. 1).
Several pre-, intra-, and postoperative parameters were recorded and analyzed, including mean age of patients at surgery, indication for LPS (hematologic disease, trauma, etc.), type of resection (upper/lower pole, other resection), type of splenic vessels dissection (main splenic vessels, collateral vessels—see below), type of device used for splenic section/hemostasis, additional procedures performed, intraoperative conversion to laparotomy, conversion to TS (by splenic remnant extirpation), operative time (OT), morbidity/mortality, adverse outcomes (AOs), intraoperative adverse outcomes (IAOs), hospital stay (HS), and follow-up.
Perioperative morbidity/mortality is defined according to Clavien-Dindo. 32 IAOs are defined as any intraoperative event that represents a deviation from the “normal” operative procedure, including conversion to laparotomy for any reason (technical difficulty, bleeding, difficult specimen extraction, etc.), blood transfusion, and intraoperative conversion to TS. AOs include IAOs, perioperative morbidity, and reoperations within 90 days from LPS due to surgical complications. Patients undergoing conversion from LPS to open surgery as well as those eventually needing salvage TS were analyzed in detail separately.
Articles comparing the results of LPS and those of alternative mini-invasive options, namely open PS and laparoscopic TS, are also analyzed separately.
Results
All gathered information about 457 patients undergoing LPS is reported in Table 1.
Characteristics of the Studied Population (457 Patients, 59 Articles)
Reporting the use of stapler alone (two cases) or in association with other devices.
AOs and IAOs include morbidity, mortality, conversion to laparotomy, and conversion to total splenectomy; AOs are intended as occurring perioperatively within 90 days from surgery.
Including hamartoma, hemangioma and other benign lesions.
Including: Epstein-Barr virus associated inflammatory pseudotumor, 75 sclerosing angiomatoid nodular transformation, 72 ovarian metastasis (two cases) and two of splenic schwannoma (two cases)7,86 and one metastatis lesion from unknown origin. 38
Including ultrasound, radiofrequency and microwave devices.
Conversions to laparotomy and conversions to total splenectomy are reported in detail in Tables 2 and 3, respectively.
AO, adverse outcome; HS, hospital stay; IAO, intraoperative adverse outcome; OT, operative time; NQ, not quantified; NR, not reported.
Association Between Selected Criteria and Main Surgical Outcomes
AOs, including IAO and 90 days morbidity/mortality, 32 total splenectomy and conversion to laparotomy within 90 days from surgery due surgical complications;
IAOs, including intraoperative bleeding, iatrogenic lesion (including visceral perforation, etc.), intraoperative splenic totalization and laparotomic conversion.
AO, adverse outcome; HS, hospital stay; IAO, intraoperative adverse outcome; NQ, not quantified; NR, not reported; OT, operative time.
Details of Procedures Converted from Laparoscopy to Laparotomy (n = 18)
The indication for splenectomy in patients converted to open approach is not reported.
NR, not reported.
Patients and indications
Mean reported age at surgery is 24.8 years (standard deviation ±15.3) overall. The indication for surgery is hematologic disease in 219 patients; of them, 169 patients had hereditary spherocytosis (36.9% of the whole studied population) and 19 (4.2%) had sickle cell disease. LPS is reported in 238 patients for nonhematological disease, including symptomatic splenic cyst in 103 patients (22.5%), other benign splenic neoplasm (hemangioma, hamartoma, etc.) in 54 cases (11.8%), and trauma in 26 patients (5.7%). In 7 (1.5%) patients, LPS is performed for neoplasm of malignant/uncertain nature, including 5 cases of distant metastasis (2 from ovarian cancer, 2 from Schwannoma, 1 from unknow primary).
Technique
Details regarding the type of performed resection, spleen devascularization techniques, and used devices for parenchymal section/hemostasis are reported in Table 2.
Placement
A variable number of trocars is reported to perform LPS. Four trocars are reported in 170 procedures,31,33–51 3 in 53,7,52–56 and 5 in 47.15,41,42,57–61 Two-port-LPS (4 patients44,62), single port (2 cases63,64), and hand-assisted LPS (1 case 65 ) are also reported.
Two types of settings are mostly reported: the so-called French position and American position (Fig. 2). According to the French position, the patient is placed in supine position (0° lateral, 20° reversed Trendelemburg position) and the leading surgeon is placed between patient's legs.44,56,59,66–68 According to the American position, the patient is placed in a left side-up position (30°–70° right-lateral semidecubitus position, 20° reversed Trendelemburg position) 66 with the operating surgeon on his right side7,43,62,63,66,69–72
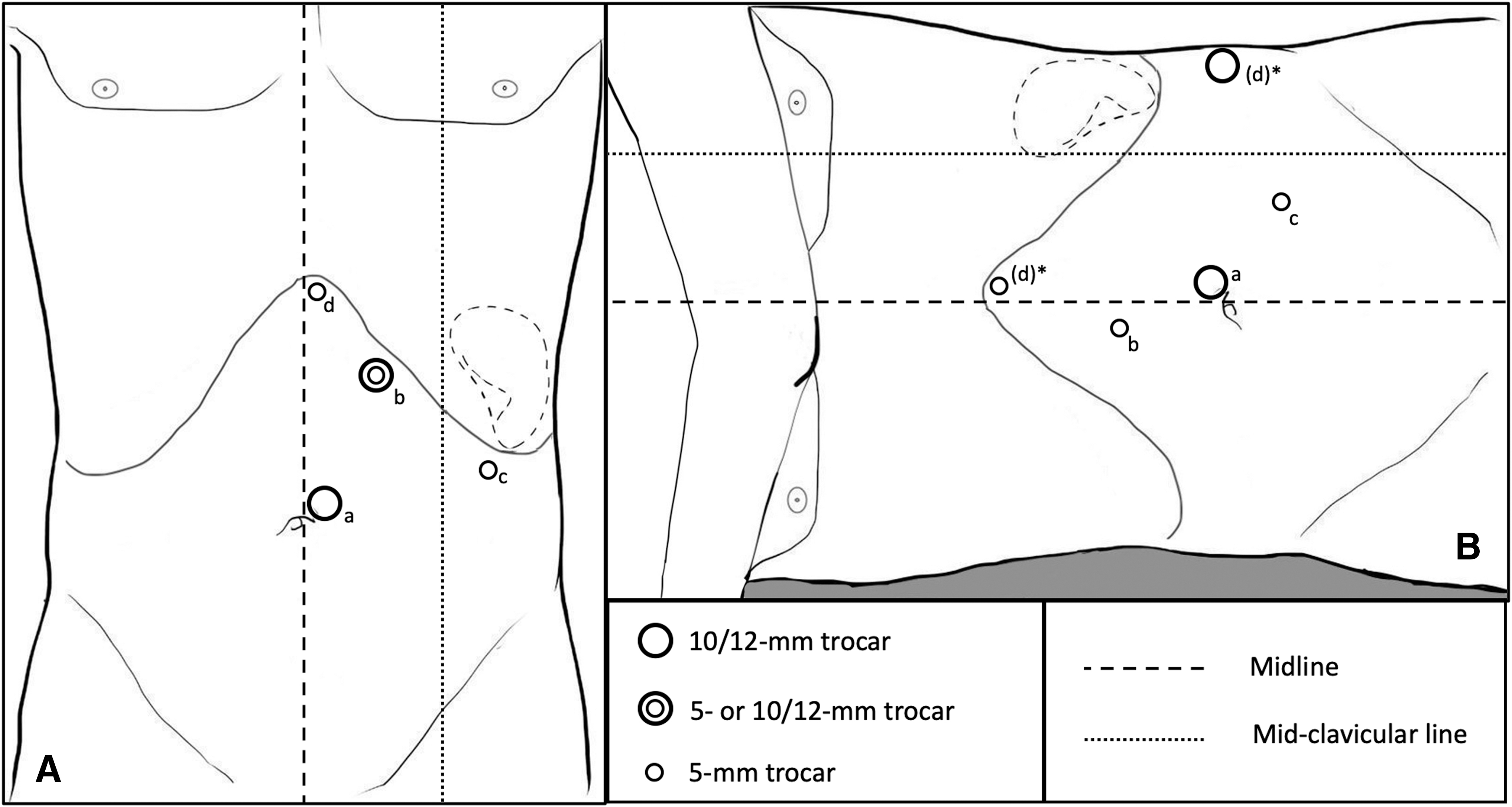
Trocars' position.
Two types of trocar placement are mainly reported: the “left-subcostal” one and “semicircular” one (Fig. 2).
Left-subcostal trocar placement 66 is reported in Figure 2A. A periumbilical optic trocar is placed, and other ports can be inserted in the left upper quadrant or in the epigastric region. Trocars' number varies according to surgeon preference (see below), including an additional trocar placed in right hypochondrium if cholecystectomy is performed contextually. 73
Semicircular trocar placement43,71 is reported in Figure 2B. The optic trocar is placed in the umbilical or periumbilical region, while remaining ports can be placed on the median line in the upper umbilical and epigastric region, for spleen elevation and retraction, or along the left rib cage. Some authors report in their series procedures performed with both French and American positions. 66
Dissection, resection, and hemostasis
After trocar placement, spleno-gastro-colic ligament is severed to expose the splenic hilum. Two approaches regarding vessels' dissection/devascularization are mainly reported: (i). division of splenic artery and vein42,48,70,74–77 and (ii) division of splenic vessels' collateral branches at the hilum of the spleen.7,15,33,34,36–38,40,41,43–47,49,50,53–56,58–62,65–68,71–73,78–88
To limit bleeding during splenic parenchyma transection, some authors propose the preoperative embolization of the spleen,15,44 or the intraoperative temporary clamping, both by clamping of main splenic vessels,7,44,62,66,86 or by compression of splenic parenchyma at the resection margin, by Lin's clamps. 7
In most cases, splenic resection consists in a polar resection, either the upper or the lower pole. The upper pole is resected in 39 patients (8.5%),15,46,48,50,54,58–60,62,65,66,68,72,74,78–80,82,85,88–90 whereas lower pole resection is performed in 81 cases (17.7%).34,40–43,49,52,53,55,56,73,75–77,81 In 337 cases (73.7%), the information concerning the resected pole is not reported or not possible to retrieve. Upper spleen pole resection is never performed for hematological disease, while 69/81 cases undergoing lower spleen pole resection are affected by hematological disease.
As reported in Table 1, various devices, including mechanical stapler, harmonic scalpel, radiofrequency, unipolar/bipolar electrocautery, and argon are used for the dissection of splenic vessel and the transection/hemostasis of splenic parenchyma.7,15,33,34,36–38,40–43,45–50,52–56,58–61,66,67,70–74,76–86,88,89 Mechanical stapler is the most frequently used device for parenchymal transection (Table 1). Some authors report the successful accomplishment of spleen section by means of unipolar and bipolar electrocautery only.15,49,55,82
Several articles report the use of various hemostatic means/agents with the purpose of improving the hemostasis of splenic raw surface after section, including fibrin glue, fibrillar hemostatic products, and so on.7,15,33,34,36–38,40–45,47–50,52–54,56,58–62,65–68,70–74,76–89,91
Results of LPS procedure
IAOs, blood loss, and OT
Among IAOs, major complications requiring conversion to laparotomy are colonic perforation during specimen extraction, 56 massive intraoperative bleeding,45,92 and pneumothorax by diaphragmatic tear due to technical difficulty by massive adhesions with the spleen. 37
Thirty-nine articles report intraoperative blood loss,15,31,33–47,49–52,54,56–65,67,68,71,75,78,89,92 ranging from 0 to 1200 cc. 45 Blood transfusion is reported by 10 articles in 22 patients.7,38,47,56,67,77,85,86,92,93 Reported reasons for transfusion are intraoperative bleeding during LPS procedure,38,45,47,56,92 cronic anemia due primary illness,67,77 or both reasons. 56 The reason for blood transfusion is not reported by four articles.7,85,86,93
Mean OT to accomplish LPS is 128 minutes (standard deviation ±43.7) overall. Specific IAO-rate and mean OTs with respect of selected criteria are reported in Table 2.
Morbidity, AOs, and HS
No mortality for LPS is reported, and morbidity rate is 5.7% overall.
Perioperative AOs include three major postoperative complications (Claven-Dindo Score III), including bleeding requiring laparoscopic hemostasis on eighth postoperative day 83 and fluid collection needing percutaneous drainage.37,40 Minor complications, including atelectasis, postoperative hyperpirexia, and pleural effusion managed conservatively, are observed in 27 patients.7,36–38,42,47,77,86,88,94 HS ranges between 1 and 26 days. Specific AO-rate and mean HS with respect of selected criteria are reported in Table 2.
Conversion from laparoscopy to laparotomy
Details of the 18 cases (3.9%) requiring intraoperative conversion from laparoscopy to laparotomy7,37,41,67,77,86,92,94 are reported in Table 3. Conversion to laparotomy is needed in patients undergoing LPS performed for hematological disease in 11 cases77,92,94 and for nonhematological disease in 37,37 (it is not reported in 4 cases). Bleeding (4 cases)7,92 and difficult specimen extraction (3 cases)41,67 are the most frequently reported causes of conversion to open access.
Conversion from PS to TS
Details of the 17 cases (3.7%) eventually needing TS by spleen remnant extirpation36,37,42,47,56,70,71,77,83,85,86 are reported in Table 4. In 4 cases,36,37,47,85 TS is performed intraoperatively owing to massive bleeding (2 cases),36,85 hemodynamic instability by hemoperitoneum due to traumatic shuttered spleen (1 case) 47 and suspicion of spleen malignancy at intraoperative histology 37 Overall, 8 patients42,56,70,71,77,85 with hematological disorder underwent TS and 9 with a nonhematological disease.36,37,47,83,86 Among patients with hematological disease, 1 patient underwent conversion to TS intraoperatively, 85 whereas in the remaining cases TS was performed 3–129 months postoperatively.
Reported Conversions from Partial Splenectomy to Total Splenectomy
Interquartile range (first–third interquartile score 15°–75°).
NR, not reported.
Comparison between LPS and other approaches to splenic resection
LPS versus open PS
Two articles compare the short outcomes of LPS and open PS.84,87 In a hematology-oriented article, Buesing et al. 87 analyze long postoperative outcomes (postoperative laboratory examinations, pre-/postoperative splenic size, blood transfusion, infective complications, and TS) of 62 children undergoing PS for hereditary spherocytosis, 24 by open approach, and 38 by LPS. LPS presents higher intraoperative blood loss (mL 195.6 ± 224.0 versus 70.6 ± 48.3, P < .05) and higher reticulocyte count 1 year postoperatively (7.0% ± 6.0 versus 3.7 ± 1.8, P < .05), but splenic regeneration 1 year after PS is not significantly different between the two groups. Most symptoms' recurrences (5 versus 1) and all completion TSs (3) are performed in patients undergoing open PS. Potential selection bias are aknowledged, as patients undergoing open PS present longer follow-up (47.8 versus 19.3 months, P < .05), greater preoperative splenic size (17.4 versus 13.4 cm maximum diameter; P < .05), and greater splenic size reduction (12.1% versus 23%, P < .05). 87
Reporting the results of PS in 17 patients affected by splenic focal masses (hemangioma or cyst), Wang et al. 84 compare nine LPS procedures and eight open PSs, showing longer OT (170 minutes ±56.4 versus 100.6 minutes ±20.6, P < .005) and shorter HS (7.1 days ±1.8 versus 9.1 days ±1.6) in LPS group. Blood loss results as being nondifferent in the two groups. Most hemangiomas (7 out of 10) are treated by open surgery. 84
LPS versus laparoscopic TS
Three articles compare the surgical outcomes of LPS and laparoscopic TS38,41,47 Morinis et al. 41 compare the results of LPS and laparoscopic TS in two groups of 9 children affected by hereditary spherocytosis. Intraoperatively, LPS procedure is associated with longer OT (215.6 ± 20.6 versus 156.6 ± 11.4, P = .021) and greater blood loss (189 ± 159 versus 67 ± 50 mL; P = .016) than laparoscopic TS perioperatively, although morbidity is similar in the two groups. LPS is associated with higher morphine use (4.1 ± 0.6 versus 2.4 ± 0.2 days; P = .03), greater time to oral intake (4.4 ± 0.7 versus 2.0 ± 0.2 days; P = .01), and longer HS (6.3 ± 1.0 versus 2.7 ± 0.3 days; P = .005). Nuclear scan 6–8 weeks postoperatively shows residual perfused splenic tissue in all LPS patients, and there is no significant difference between groups with respect to rise in hemoglobin level. Although there is a trend toward a smaller decrease in reticulocyte count in the LPS group, this difference is not statistically significant.
Lee et al., 38 comparing the results of surgery in 22 patients undergoing laparoscopic TS and 15 undergoing LPS for various focal splenic lesions, do not report any difference in terms of OT (laparoscopic TS 151.5 ± 98.5 minutes versus LPS 168.6 ± 46.8 minutes, P = .483), intraoperative blood loss (laparoscopic TS 337.3 ± 188.4 mL versus LPS 422.6 ± 187.4 mL, P = .185), and transfusion rate (laparoscopic TS 13.6% versus LPS 20.0%, P = .606). However, they report significant differences in specific postoperative complications, such as pleural effusion (laparoscopic TS 40.9%, LPS 0%, P = .005) and splenic vein thrombosis (laparoscopic TS 45.5% versus LPS 0%, P = .002), and postoperative HS (laparoscopic TS 5.4 ± 1.8 days, LPS 4.2 ± 0.8 days, P = .027). 38
Analyzing the results of surgery in 41 selected patients with spleen trauma (single splenic pole injury, no spleen pedicle injury, or hemodynamic instability), Li et al. 47 report no difference between 21 LPS procedures and 20 laparoscopic TS in OT (122.6 ± 17.2 minutes versus 110.5 ± 18.7 minutes, P = .117) and intraoperative blood loss (174 ± 22 mL versus 169 ± 29 mL, P = .331). During LPS, conversion to TS is eventually needed (due to worsening vital signs unstability) and laparoscopically successfully completed in 2 cases (9.52%). Although no patient suffered postoperative overwhelming post-splenectomy infection or thrombocytosis at 6-month follow-up overall, mean platelets and leukocyte count are reported as significantly lower in LPS group.
Discussion
LPS is seemingly feasible and safe, as it is reported to be associated with no mortality, low morbidity, and low rate of conversion of the access from laparoscopy to laparotomy as well as low rate of conversion from partial to TS (Tables 2–4).
Literature on LPS is extremely heterogeneous considering patients, indications, and surgical procedure, which is reportedly accomplished with evolving techniques and tools through last quarter of a century. Such a heterogeneous variety of indications for LPS7,15,36,39,41,47,54,67 eventually led to different approaches to LPS, since the purpose of surgery changes with the affection needing spleen resection. LPS, in fact, consists in a massive, 85%–95% spleen resection70,95,96 aimed to decrease erythrophagocytosis and symptoms such as fatigue and anemia of patients affected by hematological disease; on the contrary, LPS is a limited, parenchyma-preserving resection of focal lesions, 36 as well as in the case of splattered spleen, where tissue debriding is aimed to achieve the hemostasis after traumatic injury. 47 Moreover, the indication for LPS intrinsically affects patient outcome too, as it is in the case of LPS performed for trauma, where results of surgery are related to multivisceral trauma other than LPS.47,66 Hematological disease, also present peculiar outcome, as it is mostly performed in children with a sistemic disease undergoing surgery with all the technical implications of performing a massive resection of a large spleen in a small-sized body, and where a poor perioperative outcome may be also due to a nonvital, small splenic remnant or an early recurrence of hematological disease.
Although the intrinsic bias is associated with such a heterogeneous literature, we finally included most articles describing LPS, regardless of surgical indication, patients' population size, or article intrinsic scientific quality, to give the reader all the possible information regarding this procedure.
Several technical details of LPS procedure are worth a commentary. Similarly to the approach described for other upper-abdomen, one-side-directed procedures (cholecistectomy, surrenalectomy), two main options for surgeons' placement are reported, the French,44,56,59,66–68 and the American position,7,43,62,63,66,69–72,86 according to surgeons' background and preference. A variable number of trocars is reported to carry out LPS, ranging from one to five, four being the preferred option overall.44,56,59,66–68 Also trocars' position varied consistently through the series, being the “semicircular” and “lef-subcostal” the most popular (Fig. 2).
Similarly to the open PS procedure, two main approaches to spleen devascularization, aimed to identify the transection line (the line of demarcation between the vascularized parenchyma and the devascularized remainder) and to reduce bleeding, are reported. The main splenic vessels ligation42,48,70,74–77 relies on spleen blood supply from gastric short vessels/phrenic collaterals or left gastroepiploic artery, depending on the splenic pole, which is intended to be resected, while the selective segmental splenic devascularization implies the collateral branches division at the hilum.7,15,33,34,36–38,40,41,43–47,49,50,53–56,58–62,65–68,71–73,78–88 The first approach is the laparoscopic version of the original procedure described by Morgenstern in 1966 by ligating the splenic artery proximal to the origin of the superior polar artery, 1 thus preserving the blood supply to the superior pole by the gastric vasa brevia and the phrenic collaterals. Although few authors still prefere such an approach,34,40–43,49,52,53,55,56,73,75–77,81 the segmental vessels' dissection and division at the hilum has become the most diffused approach by laparoscopy,7,15,33,34,36–38,40,41,43–46,49,50,53–56,58–62,65–68,71–73,78–88 as it is by open approach. To reduce bleeding when transecting the spleen, splenic vessels' temporary clamping is reported.7,44,62,66,86 Alternatively, preoperative arterial embolization15,44 and spleen parenchyma compression by clamps 7 have been reported for a safer parenchymal section. Although many biases may definitely hamper our analysis' results, less AOs are associated with the periferal vessel dissection (Table 2) and may suggest this latter as the technique to be preferred.
Although in the majority of cases it was not possible to identify which portion of the spleen was resected, the lower pole of the spleen resulted as more often resected34,40–43,49,52,53,55,56,73,75–77,81 than the upper one.15,46,48,50,54,58–60,62,65,66,68,72,74,78–80,82,85,88–90 Since focal masses may be thought to harbor (and traumatic lesions to occurr) randomly in splenic parenchyma, thus leading to the resection of the affected pole with the same frequency, such a trend toward a more frequent resection of the inferior pole of the spleen is due to surgeon's preference when performing LPS for hematological disease. This is in fact the only situation where the operating surgeon actually has the choice between resecting the upper or the lower pole, as the purpose of surgery in this setting is just to reduce spleen size. The reason why lower pole resection is preferred is probably that the lower pole is nearer to laparoscope and instruments, thus it is considered easier to reach. In the case of selective segmental splenic devascularization, the mobilization of colonic splenic flexure and the dissection of the lower pole is seemingly perceived as an easier task than dissecting the upper pole of the spleen from gastric fundus and diaphragm. When the main vessels' dissection is preferred, the collateral vascularization by gastric short vessels is probably considered as more effective than gastroepiploic vascular anastomosis in preventing splenic ischaemia/infarction. In our opinion, selection bias plays a major role in the reported higher rate of AOs after lower pole resection, as it is frequently performed for hematological disease, where reoperations and completation TS are more often needed and follow-up is usually longer.
Although retrospective nature, heterogeneity of procedures, and small numbers do not allow for any statistical analysis, the present series may allow for an overview of means of parenchymal section and hemostasis. Since 1995, a variety of techniques/devices has been proposed, including mechanical staplers,7,38,41,42,47,48,53,56,61,73,77,80,83,84,86,87,91 various types of electrocoagulation,15,33,36–38,43,44,47–49,53–56,59–62,65,68,70–73,78,79,81–83,85–87 and ultrasonic dissectors.34,36–38,41–43,45–47,50,56,58–62,66–68,71–73,78,80,81,84–87,89
Since the mid-2000's, new energies' cutting/coagulating devices (harmonic scalpel),34,36–38,41–43,45–47,50,56,58–63,66–68,71–73,78,80,81,84–89,97–99 radiofrequency,7,33,40,44–46,53,59,71,72,74,76,79,86,90,100 and hemostatic agents (TachoComb®70 Tachosil®52 and FloSeal®)62,80,101 have been proposed for safer LPS. In general, during the studied period, the choice of section/hemostasis tools seems more to follow technology progress, surgeon's curiosity, and instrument availability in a specific environment than proven effectiveness.
Although LPS seems a safe procedure with no mortality, low morbidity/blood loss, and a 4.9-day-mean HS, nevertheless, major complications are also reported, including life-threatening situations, which may be challanging to manage laparoscopically, including three, namely colonic perforation, 56 massive bleeding, 92 and diaphragm perforation, 37 eventually needing emergency laparotomy. Although the rates of conversion to open surgery and to TS are low overall, being 3.9% (18 cases)7,37,41,67,77,86,92,94 and 3.7% (17),36,37,42,47,56,70,71,77,83,85,86 respectively, the risk of potentially life-threatening IAOs should not be underestimated. Our analysis of the oucomes of LPS in our series match the findings of a recent systematic review, 102 including 252 patients from 44 articles.
Considering TS, which may be considered one of the main concerns when performing LPS, it is worthwhile to point out that conversion from LPS to TS is reported to occur intraoperatively in only 5 cases36,37,47,85 (in 1 case owing to intraoperatively suspected malignancy 37 ), and in 5 cases perioperatively.36,47,83,85 In fact, the most frequently reported reason for completion TS is LPS's failure in managing symptoms (anemia, etc.) of hematologic disease or the early recurrence of this latter (Table 4).
Considering PS mortality, although the only three reported fatalities actually occurred after PS performed by open approach,103–105 those outcomes are worth being known by laparoscopic surgeons. Considering a 27-year-old patient dying from streptococcus meningitis 13 years after 2/5 PS for trauma, 105 interestingly, the patient underwent technetium liver-spleen scan 3 months, and 2, 3, and 5 years postoperatively, showing a normal pattern and did not receive pneumococcal vaccination at any time. 105 The record reported patient eventually died for fecal peritonitis by accidental colonic perforation. 104 The last one 103 was a 17-month-child with hematologic disease eventually dying of sepsis 8 months after PS was postoperatively converted to TS. Although this latter complication seems more an argument in favor than against PS, as the purpose of LPS is to avoid TS, these data should not be forgotten when planning LPS, as, in roughly 1/25 cases, LPS will end up in TS. The first reported fatality seems to suggest that pneumococcal vaccination is indicated even after successful PS with evidence of vital spleen remnant at long-term postoperative follow-up.
A comparison between the results of LPS and alternative mini-invasive surgical options, namely laparoscopic TS and open PS, is attempted by some groups,38,41,47,84,87 with variable results. Compared to laparoscopic TS, it is not clear whether longer OT or greater intraoperative bleeding are associated with LPS.38,41,47 Results concerning postoperative course are also conflicting, as LPS' HS is reported as being shorter 38 or longer 41 compared to laparoscopic TS. LPS and laparoscopic TS are reported to have similar morbidity overall,38,41,47 but, significantly, no pleural effusion nor splenic vein thrombosis are reported after LPS (versus 40.9% and 45.5%, respectively, in the laparoscopic TS group, P < .01 in both cases). Since significantly lower mean platelets and leukocyte count are reported 6 months after LPS, it may be argued that LPS may be associated with lesser thrombocytosis and its related complications.
Results of the comparison between LPS and open PS are also heterogeneous. In detail, they are conflicting regarding intraoperative blood loss,84,87 while, not surprisingly, LPS is associated with longer OT and shorter HS. 84 Although postoperative morbidity is similar,84,87 interestingly, most symptoms' recurrences and all completion TS are performed in patients undergoing open PS. 87 Such results, at times confirming some of recognized advantages of mini-invasive approach, definitely need validation in larger series, since retrospective nature, patients' selection bias and small size of studied populations limit the interest of such analyses.
Analyzing 59 articles reporting such heterogeneous population of 457 patients with various affections undergoing various procedures with low rates of complications and AOs prevented us from an analysis of LPS results and effectiveness.
The main drawback of the present series is the heterogeneity and retrospective nature of small-sized series/case reports through a quarter of a century. In such a series, surgical complications are probably underestimated, as they are not always reported by articles focused on hematology or trauma issues, or not collected by short follow-up. Since successful surgery is more likely to be retrospectively reported than bad outcome, good results of LPS may be overestimated. Nevertheless, such a review may allow surgeons to acknowledge LPS indications and techniques and to suggest how to perform it safely with the means potentially available in their environments.
Conclusion
LPS seems feasible and safe, with no mortality, low morbidity, and low rate of conversion to laparotomy and to TS. Present literature on the subject is extremely heterogeneous considering patients, indications and surgical resection, which may be accomplished with various techniques and tools. Major surgical complications are sporadically reported, thus potential risks of LPS should not be underestimated.
Availability of Data and Material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Authors Contributions
A.R.: study conception and design; acquisition of data analysis and interpretation of data; drafting the article; and critical revision of the article. A.A.: study conception and design; acquisition of data analysis and interpretation of data; and drafting the article. A.M.: acquisition of data analysis and interpretation of data and drafting the article. C.C.R.: acquisition of data analysis and interpretation of data. L.P.: acquisition of data analysis and interpretation of data. F.M.: acquisition of data analysis and interpretation of data and drafting the article; R.C.: study conception and design; drafting the article; and critical revision of the article.
Disclaimer
The following material has not been published or submitted for publication elsewhere.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.