
Abstract
Background:
Enhanced recovery after surgery (ERAS) pathways focus on decreasing surgical stress and promoting return to normal function for patients undergoing surgical procedures. The aim of our study was to evaluate the impact of an ERAS protocol on outcomes of patients undergoing primary sleeve gastrectomy and Roux-en-Y gastric bypass. Outcomes included hospital length of stay (LOS), and management of postoperative pain and postoperative nausea and vomiting (PONV) measured by pain medications and antiemetic use, respectively. Incidence of 90-day emergency department (ED) visits, readmissions, and complications were also analyzed.
Methods:
A retrospective review was performed from October 1, 2016 to October 31, 2018 of patients enrolled in the ERAS versus the conventional pathway. Patient baseline characteristics, pain and nausea scores, LOS, and postoperative outcome variables were collected.
Results:
Non-ERAS (n = 193) and ERAS (n = 173) groups had similar patient characteristics. Fewer ERAS patients required postoperative opioids and antiemetics (P < .01), with a significant difference in postoperative nausea control in favor of ERAS patients (P < .05). There was a decreasing trend in median LOS (2 versus 1, P = .28), 90-day postoperative readmissions (10.4% versus 8.1%, P = .47), and major adverse events (5.2% versus 1.7%, P = .07) after ERAS implementation. The ED visits and postoperative need for intravenous fluid for dehydration were significantly lower in the ERAS group (P = .01).
Conclusion:
Implementation of ERAS pathway for bariatric surgery was associated with less opioid usage, PONV, ED visits, and postoperative need for intravenous fluids, without increasing LOS, 90-day readmission or rates of adverse effects.
Introduction
Enhanced recovery after surgery (ERAS) protocols have been recommended as standard of care by multiple surgical specialties. In the bariatric surgery field, it has been associated with favorable outcomes, as compared with conventional management.1,2 Implementation of ERAS protocols focus on decreasing surgical stress and achieving an early return to normal homeostasis for the patient.3,4 Interventions of ERAS protocols occur in the preoperative, intraoperative, and postoperative period. Preoperative phase is focused on patient education on the surgery and recovery, prehabilitation, and avoidance of excessive fasting before surgery. Intraoperatively, the focus shifts to opioid-sparing analgesia, short-acting anesthetic agents, multimodal nausea and vomiting prophylaxis, and goal-directed fluid therapy. Postoperative management is directed toward early oral intake, aggressive mobilization, and continued focus on non-opioid multimodal analgesia to minimize nausea and vomiting, and it promotes early return of bowel function.5,6
ERAS protocols in different surgical specialties have resulted in patients reaching recovery milestones faster with subsequent earlier hospital discharge. Decreased length of stay (LOS) has been described in several studies, without an increase in overall adverse events or readmissions.6–11 Further, these protocols have shown a positive economic impact, decreasing overall cost of care.12–14 Recent studies demonstrated the feasibility of ERAS implementation in bariatric and metabolic surgery.15–21 However, ERAS protocols in bariatric surgery are still in an early stage when compared with their use in specialties such as colorectal surgery. Currently, there are multiple recommendations, and different centers have implemented ERAS with their own variations. We designed this study to share our experience of implementing ERAS in bariatric surgery, as more data are needed to develop a standard protocol.
Accordingly, the aim of our study was to assess the association between ERAS protocol implementation and postoperative outcomes for bariatric surgery patients at our institution. We evaluated the compliance to the ERAS protocol, possible effects on LOS, control of postoperative pain and nausea, and 90-day postoperative outcomes (i.e., readmissions, reoperations, emergency department [ED] visits, dehydration rate, mortality, leaks, bleeding).
Materials and Methods
We performed a retrospective review of patients who underwent primary elective sleeve gastrectomy (SG) or Roux-en-Y gastric bypass (RYGB) from October 1, 2016 to October 31, 2018. Before surgery, every patient signed an informed consent form approved by our institutional review board. Before implementing the ERAS protocol, surgeons have performed more than 1500 bariatric cases, overcoming the learning curve.
Approval was obtained from the Institutional Review Board.
Surgical technique
Four surgeons were represented in this cohort. Both laparoscopic SG and RYGB technique were performed in the same fashion by the surgeons. For the performance of the SG, a 36 French bougie with blunt tip was introduced through the mouth to tailor the sleeve. After verification of the bougie along the lesser curvature of the stomach and toward the pylorus, the stomach was transected beginning 5 cm proximally to the pylorus, using an EndoWrist® linear stapler. In the laparoscopic RYGB, the alimentary limb measures 150 cm and the biliopancreatic 60 cm. A mechanical side-to-side jejunojejunostomy was performed, and enterotomy was closed in one plane by running and absorbable sutures. Gastrostomy was performed with an ultrasonic scalpel at the distal end of the gastric pouch just under the staple line. Enterotomy was performed with an ultrasonic scalpel on the antimesenteric border of the alimentary limb 4–5 cm away from the stapled end. A side-to-side gastrojejunostomy was created with two layers of running suture by using absorbable material. If needed, concomitant procedures such as hiatal hernia repair were performed during both SG and RYGB. Laparoscopic robotic-assisted RYGB was carried out only by 2 of the surgeons, performing a similar technique as the laparoscopic approach. The SG is only performed by the laparoscopic approach at our institution.
Study design and data collection
The first study period, from October 1, 2016 to September 30, 2017, included patients who followed a conventional management pathway (non-ERAS group). The second study period included patients from October 1, 2017 to October 31, 2018, after the ERAS protocol was implemented (ERAS group). Patients with a previous history of bariatric surgery were excluded. In the non-ERAS group, patient management was not standardized, and it varied according to the surgeon preference.
During the second study period, compliance to ERAS elements was prospectively collected and monitored with checklists: enhanced preoperative education, preoperative holding medications (aprepitant 40 mg) and carbohydrate loading the night before surgery and 2 hours before surgery, avoidance of nasogastric tube, urinary catheter removal, mobility on POD 0 and subsequent hospital days, intravenous fluids discontinued and diet advancement per protocol, and lastly, adherence to scheduled acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) postoperatively. Total compliance meant that all ERAS components were followed. These data were then retrospectively reviewed.
Data collected included demographic information (i.e., sex, age, body mass index [BMI], obesity-related comorbidities, and American Society of Anesthesiologists classification), surgical type and approach, duration of operation, and conversion to an open procedure. Outcome variables included LOS and 90-day postoperative outcomes, such as visits to the ED, dehydration requiring intravenous fluids, readmissions, reoperations, mortality, morbidity classified as Clavien-Dindo Classification III or higher, 22 and postoperative surgical complications, such as anastomotic or staple line leak, and bleeding. Postoperative pain and nausea were measured in two ways: (1) based on therapies received, and (2) based on pain scores (11-point analog pain score scale) and number of postoperative nausea and vomiting (PONV) episodes recorded daily.
Enhanced recovery after bariatric surgery protocol
After reviewing the available literature on the different elements of ERAS, a protocol was developed by our institution (Fig. 1). Patients met with the service clinic nurse, who reviewed the elements of the protocol and what was expected of the patient. An information sheet describing the purpose of the ERAS protocol along with steps for the patient to follow before and after surgery was provided. At this time, patients received an incentive spirometer to begin practicing deep breathing, a pedometer to keep track of steps taken daily, and a carbohydrate-rich clear solution, if not diabetic, to consume as part of the preoperative carbohydrate loading (the night before surgery and 2 hours before surgery). Patients were advised that ingesting clear fluids was allowed up to 2 hours before presenting to surgery (3 hours if diabetic).
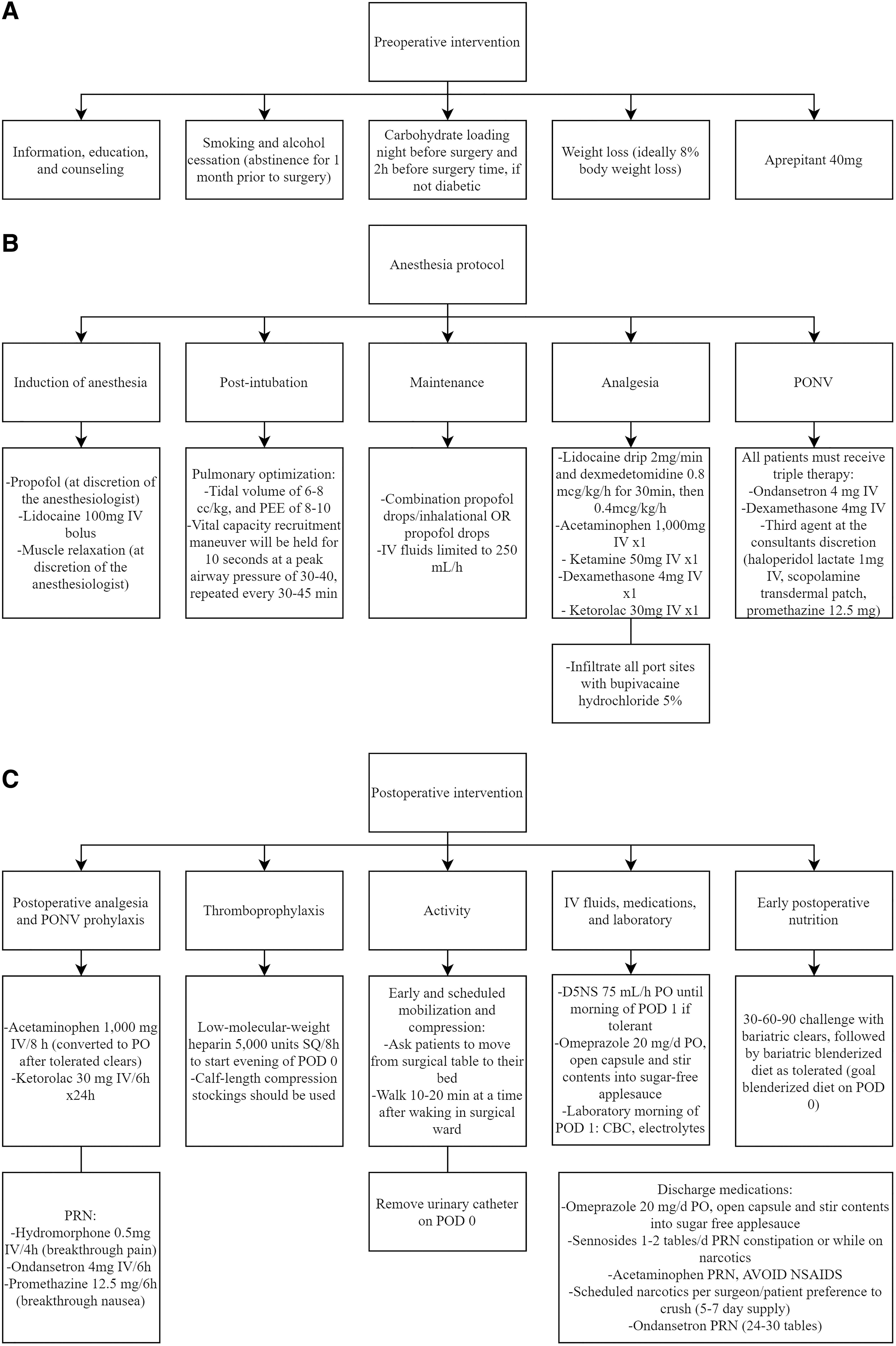
Components of ERAS protocol.
Eligible patients were identified and placed on a standardized protocol as developed by the anesthesia and surgical services. Laparoscopic approach was employed in every SG case, and the robotic-assisted approach was also used for RYGB. See Figure 1 for the components of the intraoperative protocol. Tubes and drains were avoided whenever possible.
Postoperatively, patients recovered in the Postanesthesia Care Unit (PACU) and were transferred to the general surgical ward when PACU discharge criteria were met. Regardless of surgery type, patients were expected to be out of bed within 2 hours of arriving to the ward. A 30-60-90 minutes challenge with bariatric clears was then started. This consisted of sipping liquids every 30 minutes, with a gradual increase of their volume to ∼1500 mL/day. Only neutral liquids were permitted (without sugar, carbohydrates, and caffeine), followed by a bariatric blenderized diet as tolerated, with the goal of a blenderized diet on POD 0. Postoperative medications included a multimodal approach with standing acetaminophen and ketorolac, and as needed ondansetron and promethazine for PONV. Opioids in the form of intravenous hydromorphone would only be given for severe breakthrough pain with a pain score of 7 or higher. Routine upper gastrointestinal contrast studies were not performed unless required. Objective discharge criteria were achieved on POD 1 if the patient was able to maintain oral intake without nausea, ambulate with minimal assistance, and manage pain with oral analgesia.
Postdischarge pain and nausea regimen, including scheduled non-opioid pain medication (i.e., acetaminophen), along with oxycodone and ondansetron as needed for breakthrough pain and nausea, respectively, was continued for 7 days. The patient was provided a postoperative appointment and the clinic's telephone number with coverage 24 hours a day.
Statistical analysis
Nonparametric statistical analysis was performed. Continuous variables were evaluated by using t-test, reported as mean (standard deviation, SD) and median (range), and categorical variables were evaluated by using Fisher exact test and χ 2 test, reported as frequency and percentage. All statistical tests were two-sided, with α level set at 0.05 for statistical significance. SPSS software, version 25.0, Statistical Package for Social Sciences (IBM Corp.) was used for data analysis. Our study followed the reporting guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology.
Results
During the study period, 366 patients underwent primary bariatric procedures (193 non-ERAS versus 173 ERAS). Baseline characteristics were compared between the two groups (Table 1). Age, sex, BMI, American Society of Anesthesiologists classification, and surgical procedure (SG or RYGB) were similar in both groups. In the non-ERAS group, 99 (51.3%) patients underwent RYGB, with the laparoscopic approach in 48 patients (48.5%) and the robotic-assisted approach in 51 (51.5%) patients. In the ERAS group, 82 (47.7%) patients underwent RYGB, with the laparoscopic approach in 4 patients (4.9%) and the robotic-assisted approach in 78 patients (95.1%). Conversion to open procedure was not required in any group.
Baseline Characteristics of Patients With and Without Enhanced Recovery After Surgery Protocol
“—” Not applicable.
There were 0 patients with ASA grade higher than 4.
ASA, American Society of Anesthesiologists; BMI, Body Mass Index; ERAS, enhanced recovery after surgery; GERD, gastroesophageal reflux disease; OSA, obstructive sleep apnea; RYGB, Roux-en-Y gastric bypass; SD, standard deviation; SG, sleeve gastrectomy; T2DM, type 2 diabetes mellitus.
Mean (SD) surgery duration for RYGB was significantly lower during the ERAS study period when compared with non-ERAS (143.9 [38.4] minutes versus 160.1 [42.5] minutes, P = .01). However, there was no significant difference when comparing operative time for SG. The number of patients undergoing associated procedures was similar in both periods. In the ERAS group, 40 (23.1%) patients underwent associated procedures (28 hiatal hernia repair, 9 lysis of adhesions, 5 ventral hernia repair, 2 cholecystectomy, and 1 wedge gastrectomy), and in the non-ERAS group, 47 (24.3%) patients underwent associated procedures (42 hiatal hernia repair, 5 lysis of adhesions, 3 wedge gastrectomy, and 1 cholecystectomy). Some patients underwent more than 1 associated procedure.
Ninety-day outcomes are summarized in Table 2. During the study period, ERAS protocol implementation was not associated with a significant lower median LOS (2 [1–5] days versus 1 [1–8] days, P = .28). The percentage of patients discharged at postoperative day 1 rose from 49.2% to 57.8% (P = .10). Also, the number of visits to ED, and the need for intravenous fluids for dehydration significantly decreased.
Ninety-Day Perioperative Outcomes Comparison Between Groups
“—” Not applicable.
Adverse events classified as Clavien-Dindo Grade III or higher.
Cholecystectomy 2 months after laparoscopic SG.
Staple line leak 15 days after laparoscopic SG.
ED, emergency department; ERAS, enhanced recovery after surgery; LOS, length of stay; POD, postoperative day.
Postoperative use of opioid medications was significantly lower in the ERAS group than in the non-ERAS group when comparing morphine milligram equivalents both intraoperatively (10.0 [0–45.0] versus 25.0 [0–56.0], P < .01) and perioperatively (14.0 [0–99.5] versus 21.0 [0–186.7], P < .01). From the overall postoperative pain medications, the percentage of opioids (i.e., hydromorphone, morphine, oxycodone) in the ERAS group decreased compared with the non-ERAS group (51.0% versus 69.7%), with an increase of the use of acetaminophen and NSAIDs (ketorolac) (28.6% versus 19.0% and 20.4% versus 11.3%, respectively).
Overall, PONV medications were also lower in the ERAS group than in the non-ERAS group. Ondansetron and promethazine administration decreased in the ERAS group compared with the non-ERAS group (73.9% versus 78.5% and 14.1% versus 16.7%, respectively), with an increase of the use of scopolamine patches (12.0% versus 4.7%).
Postoperative average pain score was lower in the ERAS group than in the non-ERAS group up to POD 2; however, differences were not significant. Episodes of PONV in every POD were significantly lower in the ERAS group compared with the non-ERAS group (Table 3).
Postoperative Nausea and Vomiting and Pain Scores and Medication Usage Comparison Between Groups
ERAS, enhanced recovery after surgery; POD, postoperative day; PONV, postoperative nausea and vomit; SD, standard deviation.
Overall compliance was found to be substandard (<80%), with 72.3% met (Table 4). Areas of improvement were noted to be lack of mobilization on POD 0, onset of diet on POD 0, and adherence to scheduled postoperative medications.
Compliance to Enhanced Recovery After Surgery Elements (n = 173)
ERAS, enhanced recovery after surgery; POD, postoperative day.
Discussion
This study demonstrates that implementation of an ERAS protocol for bariatric surgery, a streamlined perioperative process consistent with the most current evidence, correlated with an improvement in outcomes. According to our study, ERAS implementation for bariatric surgery was associated with decreased PONV, postoperative use of opioids, and postoperative dehydration, without increased LOS, 90-day readmission, or rates of adverse effects.
Based on chart reviews, pain, PONV, and dehydration are the primary reasons for patients remaining in hospital after surgery or being readmitted after discharge.23–25 Implementation of the ERAS protocol in our study was associated with better pain control, and decreased use of perioperative opioids. The significant decrease in opioid usage found in our study (25 versus 10 morphine equivalents intraoperatively, and 21 versus 14 morphine equivalents perioperatively) represents an important goal in ERAS protocol in bariatric surgery, as this patient population is at higher risk for addiction. 26
In addition, implementation was significantly associated with less PONV and decreased use of antiemetic therapy (P < .01). Multimodal opioid sparing analgesia may reduce the risk of adverse events related to opioids, such as PONV. Better pain control and less PONV may improve oral intake, leading to less episodes of dehydration and, consequently, less need for intravenous fluids for dehydration.
Our findings are consistent with a study by King et al., 5 analyzing 1081 patients undergoing bariatric surgery. Implementation of ERAS did not correlate with a higher percentage of patients discharged on POD 1, but it was associated with significant reductions in perioperative opioid use, PONV, and early ED visits. 5 However, as can be observed in our study, pain scores were slightly better on POD2 for non-ERAS patients, although there were no significant differences (P = .57). This was probably because mostly all ERAS patients were discharged on POD1. LOS was extended in those few patients who still referred higher pain scores, and hospital discharge was delayed until complications were discarded and pain was controlled with scheduled analgesia.
The LOS is a common measure of efficacy of ERAS protocols. Previous meta-analysis studies evaluated the efficacy and safety effects after applying ERAS protocols to bariatric surgery, reporting that LOS decreased by 1.5 days.1,20 A matched-cohort study of bariatric and metabolic patients undergoing conventional pathways versus ERAS yielded a decrease in LOS of 1.79 days with the ERAS, with lower recovery costs and shorter operative time. 27 However, no significant differences were achieved in terms of surgical outcomes. Our study did not find a significant association between ERAS pathway implementation and LOS, but a decreasing trend was noted. It is important to notice that the median LOS was of 2 days before introduction of ERAS at our institution, which possibly contributed toward reducing the difference between our groups. A recent systematic review of randomized controlled trials regarding ERAS in bariatric surgery found a reduction in LOS of only 0.5 day. 28
In terms of postoperative morbidity, a systematic review and meta-analysis described no or low influence on morbidity. 17 In accordance with these results, Lam et al. 29 supported a shorter LOS in patients undergoing SG, without increasing 30-day perioperative morbidity (3.6%, P = .4) or readmission rates (1.2%, P = .8). Our findings are congruent with the previous reported studies, showing a decreasing trend regarding readmissions and postoperative adverse events.
Another outcome that we analyzed was compliance with ERAS elements, of which our data demonstrated <80% compliance with all elements. There is significant research looking at ERAS compliance outcomes. Veziant et al. 30 performed a multicenter prospective study that followed outcomes after ERAS implementation in colorectal surgery, bariatric surgery, and orthopedic surgery specialties. Adequate compliance to the ERAS protocol was associated with better outcomes. Specifically, if compliance occurred in more than 15 elements of the protocol, a significant reduction in LOS was noted for both bariatric surgery and colorectal surgery. 30 Pecorelli et al. 31 also demonstrated improved outcomes with increased compliance to ERAS elements. When looking at our data, a question does arise as to whether higher compliance may have resulted in improved outcomes.
The literature regarding ERAS in colorectal surgery consistently demonstrated improved patient outcomes, and our experience with implementation of such pathways in bariatric surgery appears to suggest that in a larger cohort series, these findings could also be significant. Barriers to implementation included availability of certain resources and achieving adequate compliance. Further, additional nurse, resident, and covering physician education is needed regarding the protocol and its adherence. Surgeons and anesthesiologists must work together and develop an intraoperative protocol that both specialties agree on to deliver standardized, enhanced intraoperative care.
Limitations of our study include its retrospective design, relatively small sample size, shift from laparoscopic to robotic approach during the second period, and lack of patient randomization. There is also a time bias, as the study period was only 2 years long, and a small study population measured (N = 366). Further, the sequential design of the study did not allow us to perform the comparison during the same time period; thus, it may have potentially affected the outcomes, as patient care staffing and postoperative floor assignments varied, and surgical expertise increased.
The significant increase in the number of robotic surgeries performed in our institution during the ERAS period is a potential cofounder of our results. Considering this, we performed a subgroup analysis according to the surgical approach during the ERAS period (Table 5). There was no significant difference in LOS or 90-day outcomes when comparing the laparoscopic or robotic approach.
Ninety-Day Perioperative Outcomes in the Enhanced Recovery After Surgery Period According to Surgical Approach
“—” Not applicable.
Adverse events classified as Clavien-Dindo Grade III or higher.
ED, emergency department; ERAS, enhanced recovery after surgery; LOS, length of stay; POD, postoperative day.
Further education and including the nursing staff in proposed ERAS meetings would be beneficial for the nurse to feel comfortable while approaching the provider in an effort to keep the patient on the pathway. In addition, improving the documentation of many of the routine care items will aid in further compliance outcome measures. Further validation with cohorts that are large enough to obtain statistical significance is needed. In addition, our study was conducted at a single institution, and so, may not be a representative sample.
Conclusion
Our study suggests that ERAS is associated with less PONV episodes, postoperative use of nausea therapy and pain medication, including opioids, and postoperative dehydration, with no additional adverse effects or readmissions compared with conventional pathways.
Future research with larger cohort series should study the link between improved ERAS compliance by staff and patients, in addition to continued evaluation of outcomes.
Ethical Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.