
Abstract
Aim/Background:
Assessment of current role and future trends of Single-Incision-Pediatric-Endoscopic-Surgery (SIPES) in pediatric surgery among International Pediatric Endosurgery Group (IPEG) members two decades after introduction.
Materials and Methods:
An online survey was conducted between December 2019 and April 2020 on behalf of the IPEG Research Committee. All IPEG members were contacted by e-mail and asked to complete an anonymous questionnaire that included 39 items on SIPES.
Results:
One hundred eighty-four practicing pediatric surgeons completed the questionnaire from a pool of 890 IPEG members. The majority (76%) of respondents performed SIPES for more than 6 years with the following caseload per month: 1 case (31%), 2–5 cases (30%), 6–10 cases (24%), and >10 cases (17%). The four most commonly performed procedures were appendectomy (95%), Meckel diverticulectomy (55%), treatment of ovarian pathologies (43%), and U-stitch gastrostomy (40%). Complex reconstructive SIPES procedures were performed rarely. Most surgeons (95%) stated that better cosmesis is the predominant advantage of SIPES procedures. The majority of respondents (70%) felt that there is no convincing scientific evidence that SIPES offers benefits to multi-port minimally invasive procedures.
Conclusion:
Twenty years after introduction of SIPES, this technique has found its place in pediatric endoscopic surgery. Eighty percent of participating IPEG members of this survey apply SIPES for cases of lower complexity, such as appendectomy mainly for cosmetic reasons. The fact that 70% of respondents state that the scientific evidence for the benefits of SIPES is not convincing suggests that further studies and discussion on this technique are needed.
Introduction
Since the introduction of pediatric Single-Incision-Pediatric-Endoscopic-Surgery (SIPES) for appendectomy in 1993 by Begin, 1 several techniques and indications including simple ablative procedures as well as complex reconstructive surgery have been described.2–6 SIPES was primarily invented to improve the cosmetic appearance by hiding the scar in the navel. After initial enthusiasm, it is unclear whether SIPES has entered routine clinical pediatric surgical practice worldwide. To analyze the current role and possible future trends of SIPES, we aimed at investigating the perspectives and experiences of the members of the International Pediatric Endosurgery Group (IPEG) on this topic.
Materials and Methods
The survey was conducted between December 2019 and April 2020 on behalf of the IPEG Research Committee by using an online provider for Web-based surveys (SurveyMonkey™). All IPEG members (n = 890) were contacted by e-mail and invited to complete an anonymous questionnaire that included personal background and 39 items on SIPES. Since the data were completely anonymized, IRB approval was not required for this study. The invitation was sent out by e-mail with an embedded link to connect to the survey. Trainees and fellows were included in the study. The first section of the survey assessed demographic information and professional background, including type of institution and SIPES caseload. The second part assessed practice patterns, indications, benefits and drawbacks, and equipment used in SIPES. Since a completion of all 39 items was not mandatory (e.g., if a question did not apply to the respondents practice), certain questions could be skipped by the respondents. Therefore, percentages were calculated based on the total number of respondents who answered the question. Answers were anonymously collected, converted into a database with Microsoft (Redmond, WA) Office Excel™ (version 2010), and analyzed by using descriptive statistics.
Results
General information
The online questionnaire was completed by 184 practicing pediatric surgeons from a pool of 890 IPEG members (recall 21%; mean age 48.4 ± 10.0 years). Surgeons from 40 countries on five continents participated in the study: U.S./Canada 47%, South America 18%, Europe 18%, Middle East 5%, Asia 3%, Russia 2%, Africa 1%, and Australia 1%. All respondents were pediatric surgeons. The primary practice setting was a university hospital (71%). Other types of practice settings were community hospital (15%), urban private pediatric hospital (8%), multispecialty group private practice (5%), or “other” hospital (1%).
The majority (76%) of respondents performed SIPES for more than 6 years with the following caseload per month: 1 case (31%), 2–5 cases (30%), 6–10 cases (24%), and >10 cases (17%). In contrast, 38 surgeons (21%) had never performed SIPES, mainly due to disbelief in any advantage (72%). Other reasons for this included inadequate resources (11%) and lack of proficiency (8%).
Procedures
The most commonly performed procedures were appendectomy (95%), Meckel diverticulectomy (55%), treatment of ovarian pathologies (43%), U-stitch gastrostomy (40%), cholecystectomy (36%), inguinal hernia repair (32%), and splenectomy (28%) (Fig .1). Complex reconstructive SIPES procedures were performed rarely: total abdominal colectomy +/− proctectomy with ileal pouch-anal anastomosis (21%), endorectal pull-through (8%), fundoplication (8%), choledochal cyst resection (4%), and pyeloplasty (2%). Nineteen percent of the respondents performed tumor resections as SIPES. The most common kinds of pathology were tumors of the ovary (97%), adrenal gland (31%), liver (10%), and kidney (7%).
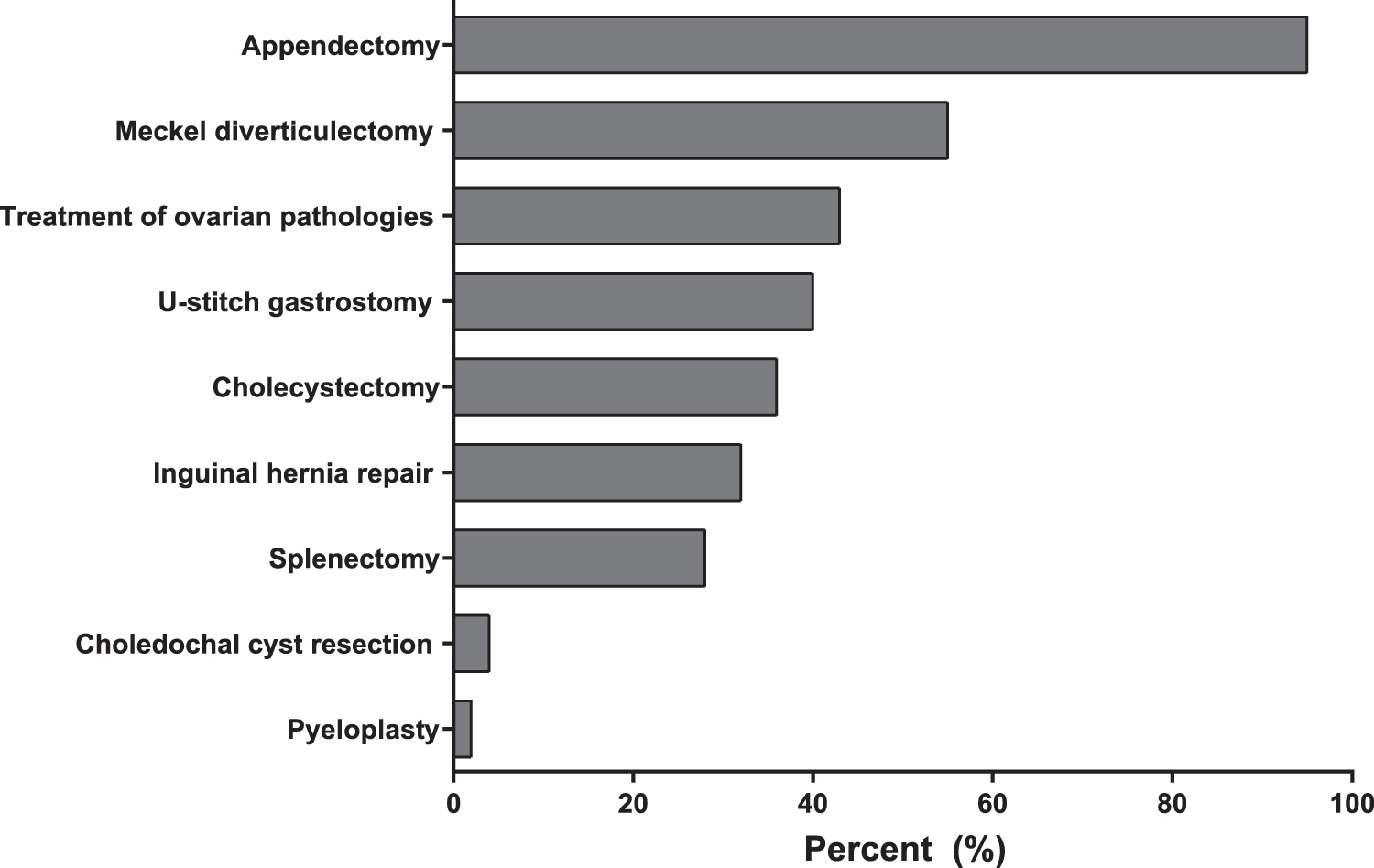
SIPES procedures performed by IPEG members. The most cases are ablative procedures. Complex reconstructive SIPES procedures were performed rarely.
Instruments and ports
Most surgeons operate with regular laparoscopic equipment (75%). Special instruments for SIPES included instrument channel operating laparoscopes (18%), bended instruments (14%), long bariatric laparoscopes (12%), single-use percutaneous needle graspers (12%), single-use articulating instruments (7%), articulating cameras (5%), and magnetic retractors (2%). Commercially available SIPES ports were used by 51%; alternative devices such as home-made ports (e.g., “glove-port”) were also frequently applied (24%). Twenty-five percent of the respondents did not state their preference regarding ports.
Conversion
Conversion from SIPES to conventional minimally invasive surgery (MIS) had been performed at least once by 87% of surgeons. Twenty-six percent of the respondents placed additional instruments via trocars, 11% via stab incisions without using a trocar, and 63% used both of these options. The causes for conversion to conventional MIS included difficulty of the procedure (83%), bad exposure (75%), bleeding (26%), adhesions (25%), and intestinal injury (6%). The causes for conversion to open surgery (at least once in 22% of respondents) were difficulty of the procedure (72%), bad exposure (47%), bleeding (34%), and adhesions (34%).
Benefits, drawbacks
Most surgeons (95%) stated that better cosmesis is the main advantage of SIPES procedures (Fig. 2). Other indicated benefits included less tissue trauma (43%), less pain (34%), shorter operating time (29%), decreased costs compared with conventional MIS (40%), and shorter length of stay (16%). On the downside, close instrument proximity (“clashing of instruments”) was perceived as the biggest problem of SIPES by 79% of the respondents. Other stated drawbacks were higher difficulty of SIPES procedures (76%), lack of triangulation (72%), longer operating time (50%), the demanding learning curve (34%), less involvement of surgical trainees (29%), more pain (20%), higher incisional hernia rate than conventional MIS (16%), increased costs (13%), and more wound infections compared with conventional MIS (11%) (Fig. 2). The answers regarding “operating time” and “postoperative pain” were conflicting, whereas 34% stated less pain and 20% more pain and 29% of the surgeons reported a shorter operating time and 50% a longer operating time.

Presumed benefits and drawbacks of SIPES.
Contraindications
The participants considered several clinical or radiological findings as contraindications for SIPES. These included an appendiceal mass on imaging (44%), perforated appendicitis (34%), a retrocecal appendix on imaging (27%), choledocholithiasis (35%), acute/gangrenous cholecystitis (29%), signs of intestinal obstruction (38%), previous abdominal surgery/adhesions (25%), obesity (37%), and coagulopathy (30%) (Fig. 3).
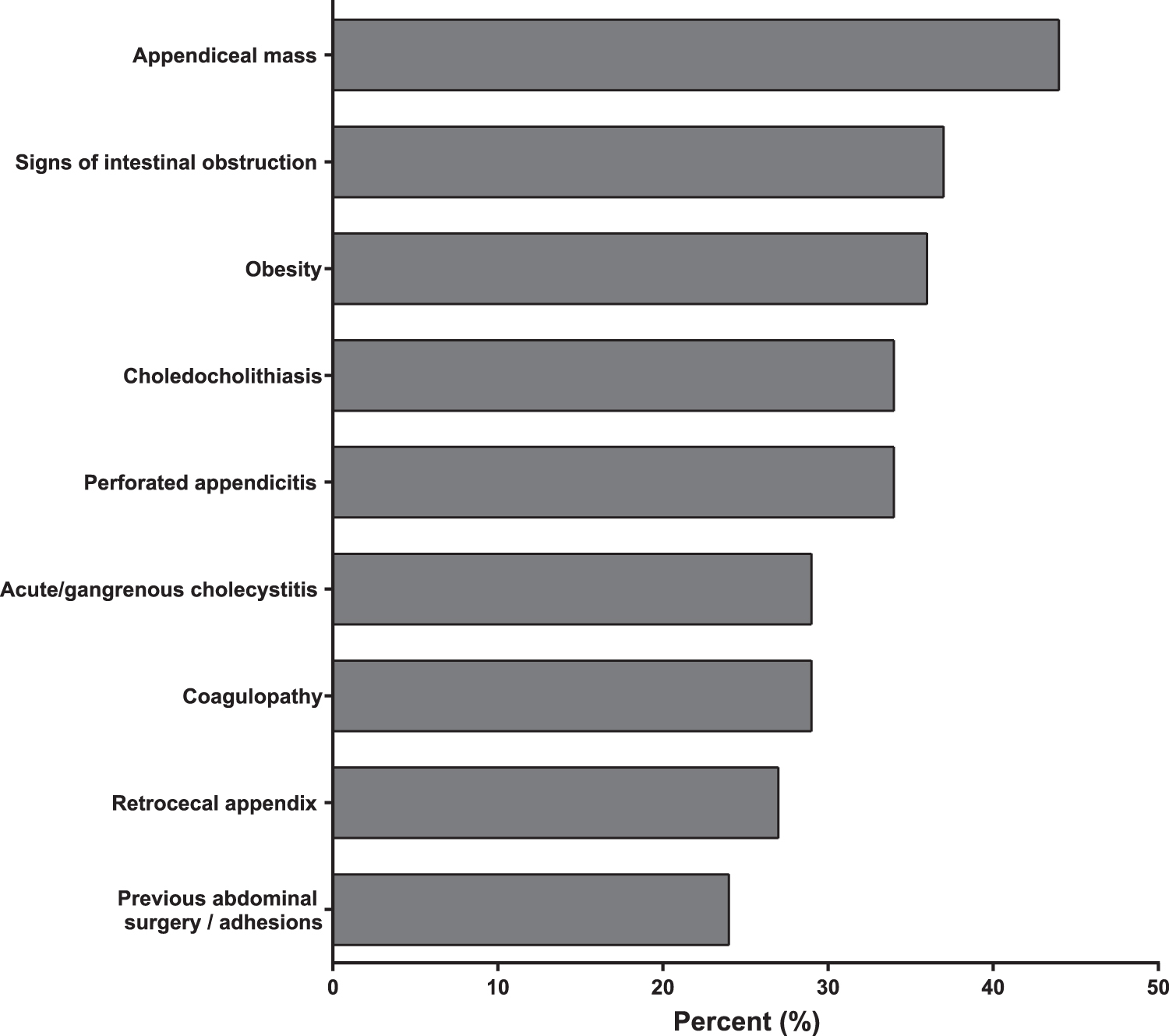
Considered contraindications for SIPES.
Decline and increase in the use of SIPES
A decline in the use of SIPES during the past 5 years was stated by 25% of the respondents. Thirty-nine percent reported that the frequency of SIPES stayed the same, whereas an increase over the past 5 years was recognized by 36%.
Abandoning SIPES
One-third (36%) reported to have abandoned SIPES over time because of SIPES being a more difficult procedure (76%) with lack of triangulation (66%). Other reported causes to stop using SIPES were longer operating time (66%), close instrument proximity (“clashing of instruments”) (59%), technical difficulties (50%), increased pain (27%), more complications (18%), and increased costs (16%) (Fig. 4).
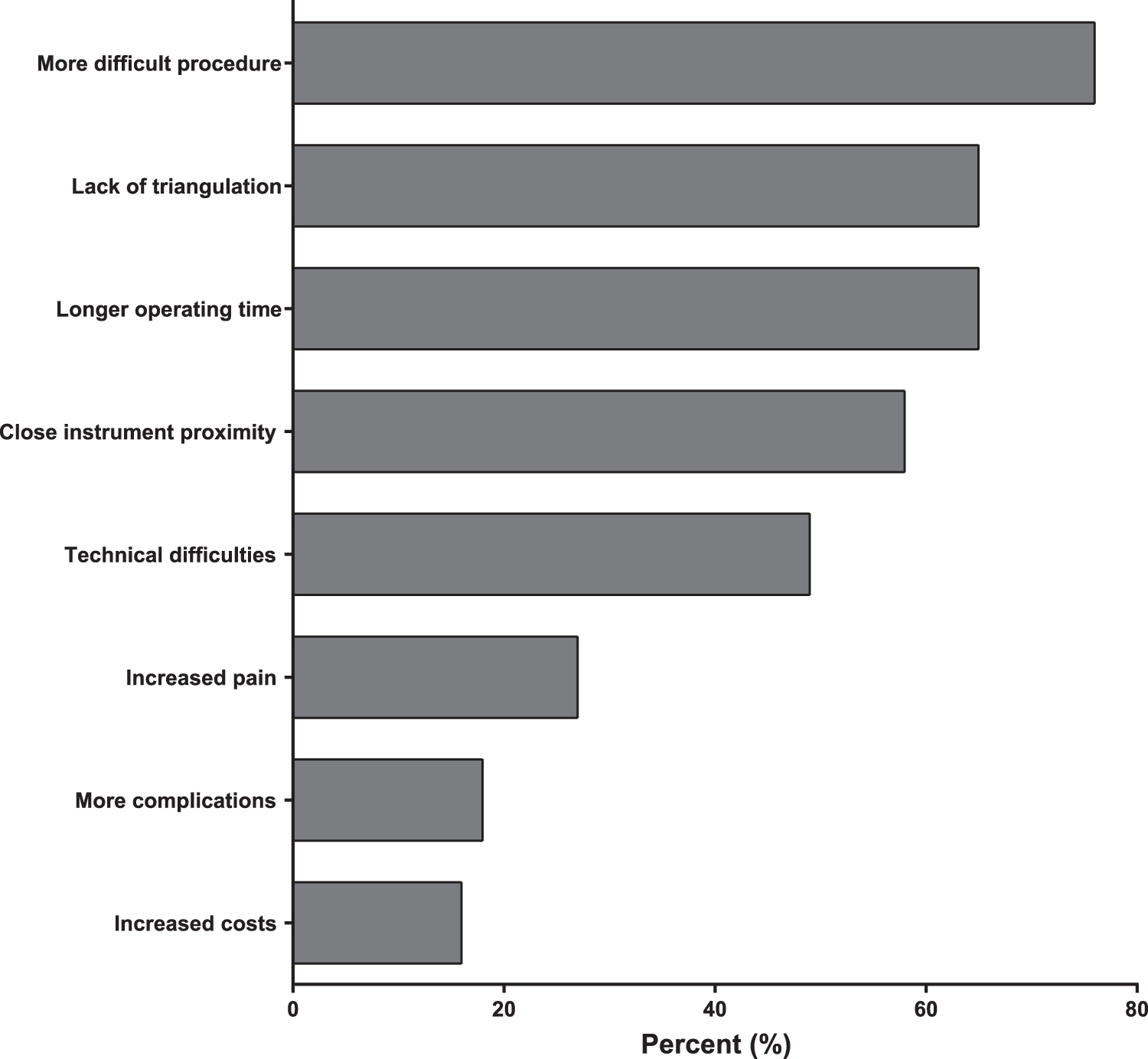
Reasons for abandoning SIPES. One-third (36%) stopped doing SIPES over time.
Robotic SILS/SIPES
Six surgeons (3%) had experience with robotic SIPES in children. Every one of these used the “da Vinci Single-Port (SP) platform” (Intuitive Surgical, Inc., Sunnyvale CA). Two of them stopped doing “conventional” SIPES.
Discussion
SIPES is mainly used for ablative procedures and non-complex surgery
Generally, SIPES was used for a great variety of less complex procedures. The four most commonly performed cases included ablative procedures and non-complex surgery such as appendectomy, Meckel diverticulectomy, treatment of ovarian pathology, and U-stitch gastrostomy.
Appendectomy was the most common performed procedure, which corresponds to a survey performed by Rich et al. in 20145 and a large patient series by authors of this survey. 3
In the survey by Rich et al. from 2014, 60% of the respondents performed SIPES cholecystectomy as the second most common SIPES procedure. 5
Although it has been shown that single-incision cholecystectomy is a safe and feasible alternative for cholecystectomy in children,7,8 our survey showed that only one-third of the surgeons were doing SIPES cholecystectomy, indicating a significant decline of this technique. One explanation for this finding might be that SIPES cholecystectomy is more difficult and demanding than multiport cholecystectomy.
Only very few surgeons used SIPES for complex reconstructive procedures such as fundoplication, choledochal cyst resection, and pyeloplasty. Compared with the results of Rich et al., there have been no trends to a higher rate of complex reconstructive SIPES procedures over the past 6 years. 5 Therefore, the role of this technique may be mainly simple ablative procedures and non-complex surgery.
Lack of triangulation (“Clashing of instruments”) remains the biggest technical problem
Different instruments for SIPES have been described; however, most surgeons (75%) operated with conventional straight instruments, which do not create additional costs.7,9–11 “Clashing of instruments” was perceived as the biggest problem of SIPES by 79% of the respondents. At the same time, only 12% of the surgeons used techniques that can limit this, such as long bariatric scopes. Therefore, it is possible that in some cases SIPES is expected to be cumbersome because certain equipment that may facilitate SIPES have not been translated into surgical practice in general.2,3,12
At least one out of 4 surgeons uses alternatives to commercially available SIPES ports (home-made ports)
In most institutions, commercially available SIPES ports were used (51%). Alternative techniques such as home-made ports (e.g., “glove-port”) were also frequently applied (24%). The “glove-port” can be used as a cost-effective method with improved ergonomics to circumvent the limitations of the conventional SIPES ports.9,13,14 Unfortunately, 25% of the respondents did not state their preference regarding ports. Therefore, we only can speculate that the surgeons might use either of these techniques or some different method.
Every second IPEG member feels that operating times are longer compared with multiport MIS
Fifty percent of the respondents stated that the operating time of SIPES was longer compared with multiport laparoscopy. It has been demonstrated that the operating times of common SIPES procedures are favorably comparable with those of multiport MIS. 7
Two prospective randomized trials comparing SIPES appendectomy and SIPES cholecystectomy with multiport (3-port and 4-port) laparoscopic approaches reported an increase in the mean operating times of 5 and 12 minutes, respectively.15,16 However, the clinical relevance of these differences in mean operating times is debatable.
Conversion to multiport MIS is not infrequent
Since SIPES is a demanding minimally invasive technique, 22% of respondents reported that they had converted at least once from SIPES to open surgery. Studies have shown that SIPES and multiport laparoscopy have similar complication and conversion rates to open surgery.7,17 However, it needs to be emphasized that SIPES is not a “one-way-street” and placement of additional trocars is always possible and SIPES should not be performed in a dogmatic way.
Postoperative pain: Results of scientific studies do not match the experience of IPEG members
Twenty percent of the surgeons felt that SIPES causes more pain compared with multiport laparoscopy (less pain: 34%). However, several studies, including a randomized controlled trial, showed that postoperative pain is similar to multiport operations.15,18 This prospective randomized trial by St Peter et al. noticed that more total doses of analgesia were given to single-site patients during the hospital stay, but not during convalescence. The authors concluded that there might be more discomfort in the early postoperative period with single-site approaches due to the larger fascial and skin incision, but the mean difference was only a single dose of analgesia, and this did not prolong hospitalization or translate into delayed convalescence. 15
The vast majority of IPEG members (70%) considers the scientific evidence for the benefits of SIPES not convincing
Different studies have shown at least non-inferior results of SIPES compared with conventional laparoscopic surgery. A meta-analysis of 12 studies, including four randomized controlled trials comparing SIPES appendectomy with conventional laparoscopic appendectomy, revealed a significantly shorter length of stay after the SIPES approach. 19 In addition, two prospective randomized trials have shown a superior cosmetic result of SIPES at follow-up.20,21 However, 70% stated that the scientific evidence for the benefits of SIPES is not convincing. This suggests that there is either an unawareness of or disbelief in these studies and that further research and discussion on this controversy is needed.
SIPES has found its place in pediatric endoscopic surgery
Twenty-five percent of the pediatric surgeons indicated a decline of performing SIPES in their institution during the past 5 years. However, most of the respondents reported that their frequency of using SIPES stayed at least the same (39%) or even increased (36%). This is in contrast to a recent survey among the society of endourological surgeons describing a steady decline in the number of single-incision procedures. 22 Even in the “peak year” (2009), the majority of surgeons only performed five or fewer single-incision procedures per year. 22 This low number of cases might be one factor leading to a decline of single-incision surgery, since surgeons may not perform enough cases to overcome the learning curve. In contrast, in this study 75% of the surgeons reported a steady state or even an increase of SIPES over the past 5 years. This indicates that SIPES has found its place in pediatric endoscopic surgery.
Limitations
Despite offering a general picture of the current practice of SIPES among IPEG members, we are aware of several limitations of our study. Only a minority of IPEG members responded (recall: 21%); however, this corresponds to recall rates of similar surveys on operative techniques.5,23 Moreover, the fact that the respondents were members of a society obligated to promote pediatric MIS may have influenced the results. Finally, we can only assume that the participants provided honest answers.
Conclusion
Twenty years after the introduction of SIPES, this technique has found its place in pediatric endoscopic surgery. Eighty percent of participating IPEG members of this survey apply this technique for cases of lower complexity such as appendectomy. Since the rate of complex reconstructive SIPES procedures is still extremely low, the role of this technique may be mainly simple ablative procedures and non-complex surgery. The main benefit is better cosmesis. One-third of surgeons were reported to have abandoned SIPES over time for the lack of triangulation, making SIPES a more difficult procedure, especially for advanced cases. The fact that 70% of respondents state that the scientific evidence for the benefits of SIPES is not convincing suggests that further studies and discussions on this technique are needed.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.