
Abstract
Purpose:
We performed a retrospective study to determine the effectiveness and feasibility of articulating linear stapler in laparoscopic total splenectomy (LTS) and laparoscopic partial splenectomy (LPS), focusing on technical laparoscopic skills that could help pediatric surgeons to avoid intra- and postoperative complications.
Methods:
Retrospective cohort study of children younger than 18 years who underwent laparoscopic spleen surgery between January 2008 and March 2020. Age, sex, indication for surgery, operative time (OT), intra- and postoperative complications, and postoperative length of hospital stay (LHS) were analyzed. Data from parenchymal resection and vessels sealing techniques were obtained.
Results:
Thirty patients, 19 LTS and 11 LPS, were included. The mean age of the patients was 10.9 years, and 16 patients were male and 14 were female. For hematologic diseases, LTS was the elective surgery, associated with cholecystectomy in 5 cases. LPS was the common procedure for splenic cysts. The stapler was used in LTS to close the hilum vessels and in LPS for parenchymal resection. No statistically significant differences in OT were observed comparing LTS and LPS. Two conversions occurred in LTS; none in LPS. The mean LHS was 6 days in both groups. No recurrence or major complications appeared in both groups at 1–12 years of follow-up. In particular for LPS, there are no relapse of cyst neither reduction in splenic function.
Conclusions:
This study shows the effectiveness, feasibility, and safety of mechanic stapler in splenic surgery both for hilum vessels sealing and for parenchymal resection. The use of this device can reduce risk of hemorrhagic recurrences or major surgical complications improving the safety of the operation.
Introduction
Splenic pathologies requiring surgical treatment include benign lesions such as cysts, hematologic diseases, vascular anomalies, and post-traumatic lesions. Splenic nonparasitic cysts are rare in pediatric population. They can be mainly congenital or secondary to previous trauma, usually discovered incidentally as abdominal mass or during systematic imaging. 1 In some cases, they can become symptomatic after intracystic bleeding, infection, or rupture, requiring surgery. Hematologic disorders are the most common indications for splenectomy in children: hereditary spherocytosis, idiopathic thrombocytopenic purpura, and sickle cell anemia with sequestration account the majority of cases. 2
Splenic hemangiomas are rare lesions, representing the most common form of benign primary tumor of the spleen. They can be symptomatic but never associated with spontaneously rupture. 3 Post-traumatic lesions can lead to intraparenchymal hematoma or acquired cyst. 4
According to splenic pathology, the goal of surgical management is to avoid complications preserving, when possible, spleen function. Total or partial splenectomy can be safely performed laparoscopically, 5 but to date is still unclear the indication for one or the other. Laparoscopic total splenectomy (LTS) is associated with a small, but potentially life-threatening risk of overwhelming post-splenectomy infection and, therefore, in the pediatric population requires preoperative vaccination against encapsulated bacterial organisms and chronic, daily penicillin prophylaxis. 6 Laparoscopic partial splenectomy (LPS) is a technique in which a portion (20%–50%) of the spleen is preserved during surgery to allow for postoperative retention of splenic immune function.7,8
Despite this, in hematologic diseases, the indication for an LPS is controversial and related to the specific disease. 9 Surgical hot topics are represented by intraoperative bleeding control and strategy of parenchymal resection, which require challenging skills. 10 To prevent complications, we experienced the use of articulating stapler.
We performed a retrospective study to determine the effectiveness and feasibility of mechanical stapler in LTS and LPS. We aim to share our experience compared with those from the literature, focusing on technical laparoscopic skills that could help pediatric surgeons to avoid intra- and postoperative complications.
Materials and Methods
We conducted a retrospective cohort study of children younger than 18 years who underwent laparoscopic spleen surgery (LTS and LPS) between January 2008 and March 2020 in two pediatric surgery referral centers. Patients with benign lesions, hematologic diseases, and vascular anomalies were included.
For hematologic disease, splenectomy was recommended in symptomatic children transfusion dependent, with severe anemia or recurrence of hemolysis, according to local protocol and international guidelines. In all patients, an ultrasound was performed to check the dimension of the spleen and the coexistence of gallstones to guide the decision to make an associated cholecystectomy. The preoperative workup also included computed tomography (CT) or magnetic resonance imaging (MRI) with three-dimensional (3D) imaging reconstruction to evaluate the anatomy of splenic vessels and the position of intraparenchymal lesion (Fig. 1). Age, sex, indication for surgery, operative time (OT), intra- and postoperative complications, and postoperative hospital stay (LHS) were analyzed for all patients from hospital database and de-identified.
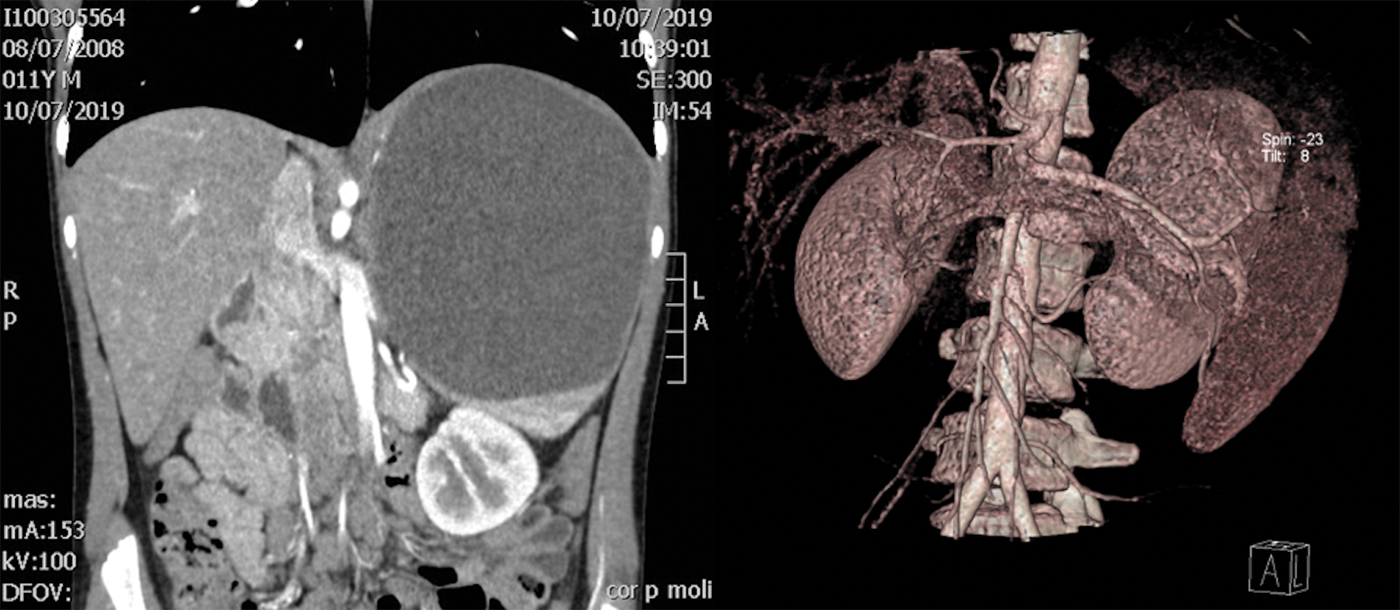
Preoperative MRI scan with 3D imaging reconstruction to evaluate the anatomy of splenic vessels and the position of intraparenchymal lesion. 3D, three-dimensional; MRI, magnetic resonance imaging. Color images are available online.
Patients were grouped according to surgical techniques.
Surgical techniques
Laparoscopic total splenectomy
An anterior approach is performed. The patient is placed in the supine position (reverse Trendelenburg position, right leaning). Surgeon and assistant are between the legs of the patient. The optic trocar (a 12-mm trocar 30°-lens) is inserted in the umbilicus according to the Hasson technique. Pneumoperitoneum is established and maintained at a pressure level of 12 mmHg. Three 5-mm ports are inserted, respectively, in epigastrium (under the xiphoid appendix), left and right hypochondrium. An additional 12-mm port is positioned in left lower quadrant. This port allows to introduce the Endo GIA® parallel to the hilum vessels, improving ergonomics. We practice sealing of short gastric and lower polar vessels with LigaSure®; major vessels of the vascular hilum are sectioned with vascular Endo GIA 6 mm (Fig. 2). Dissection and enbloc release of the spleen with LigaSure is completed. Spleen is placed in an endobag 15 mm of diameter and 40 cm3 volume capacity. After spleen grinding, the endobag is extracted through the umbilicus. A drain is left in place.
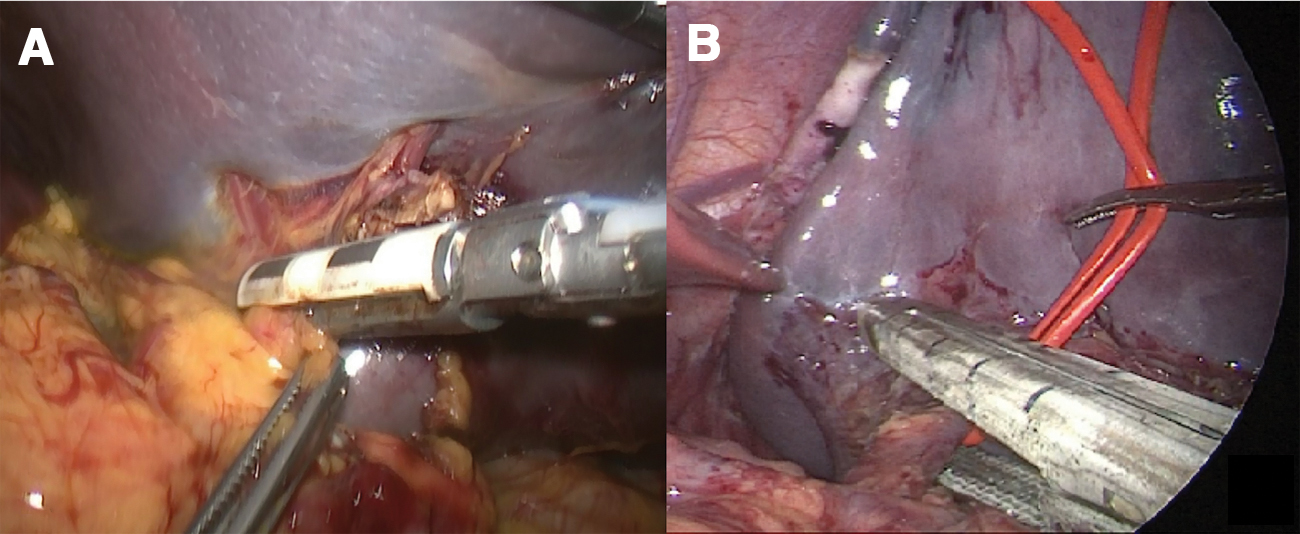
LTS: vessel sealing with LigaSure®
Laparoscopic partial splenectomy
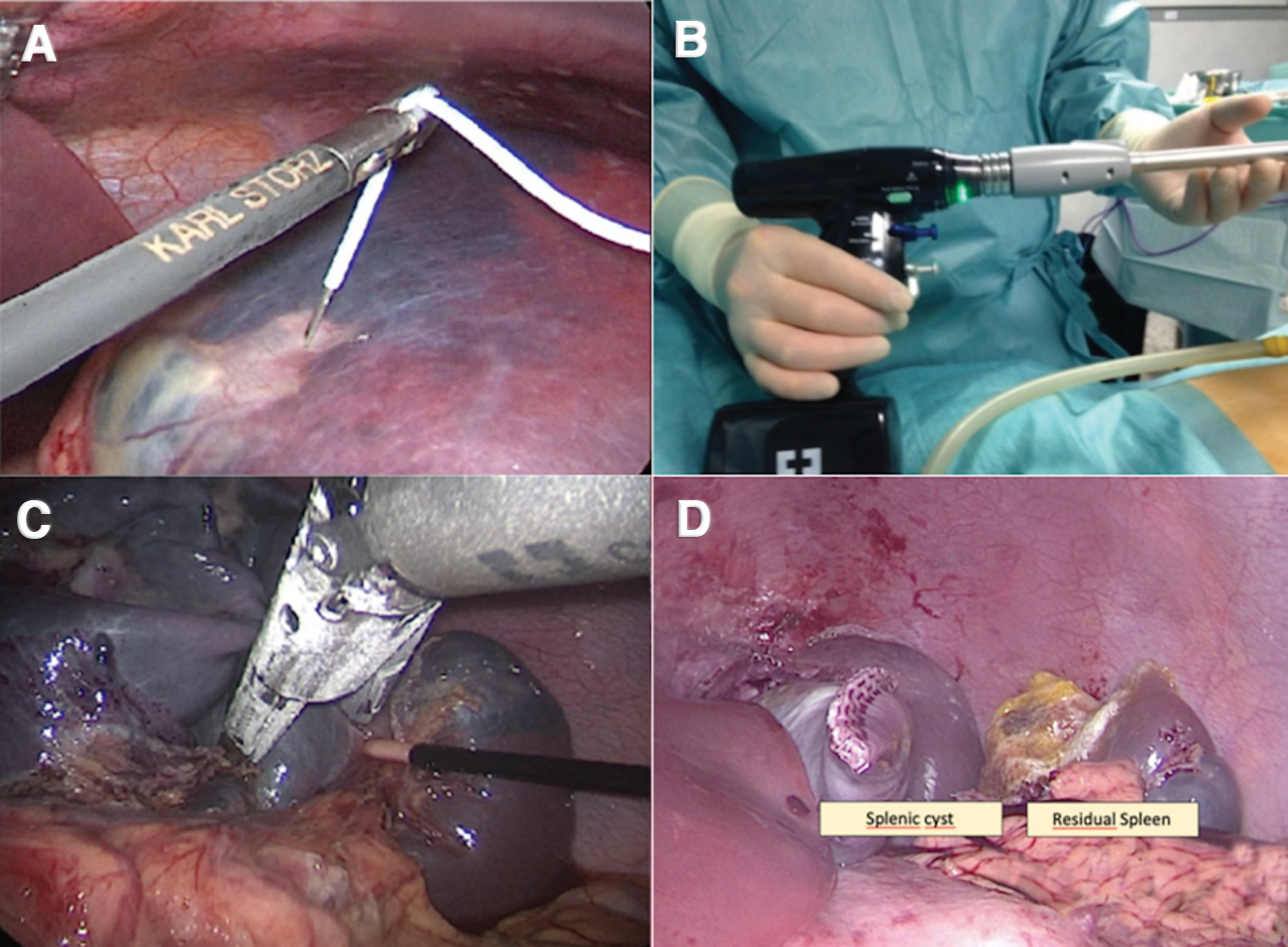
Patient and surgeons are in the same position as LTS. There is no difference for the optic and three 5-mm ports position, but in LPS, we do not use the additional 12-mm port. In this technique, resection involves mainly upper or lower pole. Therefore, the articulating instrument could be better maneuvered from the umbilical port. At this time, a 5-mm optic is placed in one of the two lateral 5-mm ports. If a cyst is present, we proceed to percutaneous punction of the cyst and aspiration of intracystic fluid. This anterior approach provides a clear exposure of splenic vessels and allows their selective division. According to the cyst position in relation to splenic vessels anatomy, we sealed with LigaSure the afferent vessels, preserving the vascularization of the remaining spleen. Resection of the splenic parenchyma is performed with mechanical staplers through the umbilical port, in particular Endo GIA Tri-Staple™ Technology 60 mm Medium/Thick (Fig. 3). Recently, a new advanced surgical stapler, the Signia™ Stapling System (iDrive®), has been used (Fig. 3). This device has sensors that detect the tissue being worked and adjust its speed to produce optimal staple lines. The device is completely powered, including its rotation, articulation, and opening and closing of the jaw. During this maneuver, a 5-mm 30° optic is placed on the right hypochondrium trocar. The extraction of the spleen is performed with an endobag through the umbilicus. A drain is left in place.
To evaluate the use of stapler device for parenchyma resection in partial splenectomy on pediatric patients, we performed an electronic database search on CINAHL, PubMed, and Embase. We included studies with the topics “laparoscopic partial splenectomy” and “children” or “pediatric” in the abstract, and then, we focused on description of vessels sealing and parenchyma resection technique through the article.
We performed statistical analysis with chi-squared test for comparisons of continuous variables between groups. Categorical variables were analyzed by Fisher's exact test.
Results
We included 30 patients who underwent laparoscopic splenectomy, 19 LTS and 11 LPS. The mean age of the patients at surgery was 10.9 years (range: 5–18 years) in both groups, 16 patients were male and 14 were female. Most common diagnosis was hematologic diseases (10 hereditary spherocytosis, 2 beta-thalassemia, 1 autoimmune hemolytic anemia, 1 acute anemia in acute lymphoblastic leukemia, 1 chronic autoimmune thrombocytopenia), followed by splenic cysts (13 cases) and benign tumor (2 splenic angiomas).
For hematologic diseases, LTS was the elective surgery, associated with cholecystectomy in 5 cases due to the presence of gallstones. However, LPS was the common procedure for splenic cysts, except of 2 cases of cyst behind the hilum requiring a total splenectomy due to the position.
The stapler was frequently employed in LTS (8/19 cases) to close the hilum vessels and in LPS for both hilum vessel sealing (2/11 cases) and parenchymal resection (11/11 cases).
The mean OT for LTS was shorter than LTS with associated cholecystectomy (231 minutes versus 298 minutes; P = .01); no statistically significant differences were detected comparing LTS and LPS (231 minutes versus 247 minutes; P = .51).
Two conversions to open surgery occurred in the LTS group: in one child due to thick adhesions that hindered laparoscopic visualization; in the other one due to persistent bleeding during sealing of short gastric vessels. No conversions were observed in LPS, the only intraoperative complication (mild bleeding) was successfully managed with sealing devices.
In 2 cases of LTS, a Pfannenstiel incision was necessary for the extraction of the spleen due to the huge dimension. In all the other cases, the spleen was inserted into an endobag and grinded before extraction through the umbilicus.
In the LTS group, the spleen dimension was 13.32 (±2.59) cm, whereas in the LPS group, it was 14.11 (±3.15) cm (P = .5).
The mean LHS was 6 days in both groups, with no significant difference.
All patients were followed up for 1 year (range 1–12 years). We observed no recurrence or major complications in both groups (Fig. 4). In particular for LPS, there are no relapse of cyst neither reduction in splenic function. Data from our series are summarized in Table 1.
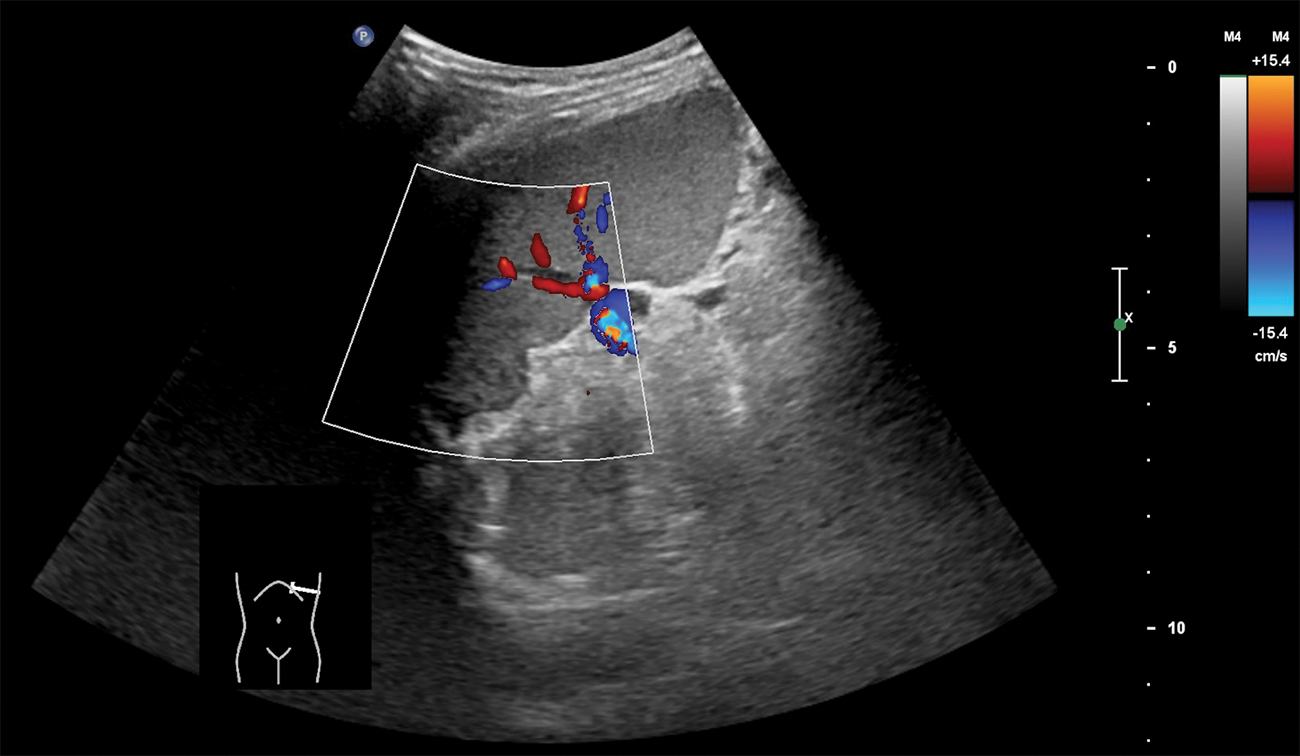
Postoperative imaging at 3 months of follow-up shows splenic remnants appearing as a normal spleen (8.87 cm of longitudinal diameter). Color images are available online.
Demographics and Operative Data
One case required transfusion for postoperative anemia.
LPS, laparoscopic partial splenectomy; LTS, laparoscopic total splenectomy; SD, standard deviation.
After medical database search and article lecture, we found four pediatric studies matching our inclusion criteria, reporting technical specifies about used device for splenic parenchymal resection. The authors describe the use of ultrasonic scalpel in three studies and the employment of both ultrasonic scalpel and stapler in one. We did not find reports about the use of advanced surgical stapler, as in our experience.
We grouped all these studies and our results according to parenchyma resection to evaluate safety of device. Significant difference between groups was found in LHS (P = .02), need for transfusion (P = .01), and complications (P = .05), as shown in Table 2. It was not possible to compare OT due to lack of data.
Comparison Between Sealing Devices
No bleeding complications or recurrence in all groups.
LHS, postoperative length of hospital stay; PE, pleural effusion; SD, standard deviation; SSI, surgical site infections; TE, thromboembolic complications.
Discussion
Laparoscopic splenectomy is a safe and established procedure in children. 11 LTS or LPS, both with associated cholecystectomy, must be scheduled after an appropriate preoperative diagnostic workup. In our experience, performing preoperative CT scan or MRI in all patients allowed us to elaborate 3D vascular imaging reconstruction to better plan the intervention and help the surgeon. Moreover, a detailed study of splenic vascular anatomy can reduce the incidence of totalization during LPS. Weili et al. described in 2013 the importance of preoperatory CT evaluation. A better understanding of the splenic segmental anatomy allows performing LPS with a decreased risk of bleeding and post-splenectomy infections, short hospital stay, and superior cosmetic. 12
Our experience shows no significant difference between LTS and LPS in term of complications and LHS.
In our series, the majority of cases who required LTS were hematologic disorder, most of all hereditary spherocytosis.
Although some authors described a good outcome for LPS in some hematologic diseases and focal splenic tumors, 13 there is a lack of evidence for pediatric population about good outcome at medium–long-term follow-up. That is why in our experience, according to multidisciplinary team with pediatric hematologist, we preferred to perform LTS instead of LPS. In particular, in sickle cell disease, which represents the majority of hematologic disease in our series, LPS is not advised. 14
Limiting evaluation to benign pathology as cysts, we can affirm that LPS is a safe and feasible procedure in experienced hand. This technique allows preserving a sufficient portion of parenchyma avoiding future infective complications. In our experience, this procedure requires the same OT of LTS (that results significatively prolonged in LTS only if associated with cholecystectomy, P = .08), while LHS is similar. Saving splenic parenchyma allows preventing postoperative infections because the immune role of the spleen is conserved, as other authors stated.7,8
Since the goal for the treatment of splenic cysts is to prevent recurrences, cystectomy and unroofing cannot be considered a valid alternative to LPS because they are associated with a high recurrence rate (until 80%),9,15 while partial splenectomy has almost no recurrence. 1 Using appropriate devices, surgeons can safely perform the LPS without risk of bleeding. To transect the splenic parenchyma, several instruments may be used: Ultracision® (ultrasonic scalpel), LigaSure, CUSA®, waterjet, single-stage coagulation, and argon knife.
Reports in pediatric surgery show larger experience in using ultrasonic scalpel and LigaSure. This last device permits to control the vessels (up to 7 mm of diameter), and it is frequently used to resect splenic parenchyma.
The role of staplers in pediatric patients is not clear since we found only one study reporting use of this device in parenchyma resection 1 and another one limited on hilum vessels sealing. 16 In our experience, the stapler demonstrate to be safe to close the hilum vessels both in LTS and in LPS since we had no bleeding complications neither need of transfusion. In all the 11 patients from the LPS group, parenchymal resection was successfully performed with mechanical stapler, with no recurrence observed during the follow-up. According to our results, the use of stapler is safe and allows bleeding control without risk of local infections and permits a perfect reconstruction of the remaining spleen and capsula. Ultracision or LigaSure is effective in parenchyma section but leave a bloody surface that can cause adhesions, secretions, and secondary bleeding. Thanks to a wider opening and a more harmonious closing of the parenchyma, the latest generation staplers (iDrive) limit the splenic tissue lacerations during the resection maneuver. In our series, no patients needed transfusion after LPS for bleeding.
Our mean OT was longer than literature reports: in our series, more than a half of the time is required by grinding and extraction of big spleens through the umbilicus, while in the literature is not specified if the OT include or not this maneuver, or if they use a complementary Pfannenstiel incision. In our experience, an umbilical extraction within endo-catch bag has to be preferred for a better aesthetic result, even prolonging OT, limiting use of complementary Pfannenstiel incision to those cases in whom the extraction maneuver resulted difficult.
In our experience, spleen dimension and age of child do not represent a limitation for a laparoscopic approach. Even with large spleen (over 15 cm), the procedure can be safely performed. Our two conversions were related to adhesions and bleeding control more than splenic dimension. Further studies analyzing the correlation within conversion rate and spleen dimension are needed.
Considering the comparative reports of Table 2, LHS results longer for procedures using staplers rather than ultrasonic scalpel (5.7 days versus 6.6 days; P = .02); the incidence of complications was lower in the stapler group (3.4% versus 13.7%; P = .05), although no relevant bleeding was observed in all articles. There is also a significant reduction in need for transfusion in the stapler group (5.08% versus 21.56%; P = .01). These results focus attention on the great safety of mechanical staplers in performing splenectomy; nevertheless, the relationship between complications and employed devices needs to be further evaluated in larger series focusing on different endpoints.
Limitations of this study are the retrospective cohort analysis and the small sample size. Moreover, our results could be bias by the surgical indication in terms of pathological disease. Since splenic pathology requiring surgery in pediatric age is rare, multicentric cohort studies and prospective Randomized Clinical Trials could better define the safety and effectiveness of stapler compared with other sealing devices in parenchyma resection or vessel sealing.
Conclusions
This study shows the effectiveness and feasibility of mechanic stapler in LTS and LPS for vessel sealing and parenchymal splenic resection, especially for benign lesions as cysts. The use of these devices, combined with Harmonic scalpel or LigaSure, is safe and can reduce risk of hemorrhagic accidents, recurrences of the lesions, or other major complications. In our series, minimally invasive surgery and extraction of the spleen sample through the umbilicus led to an excellent cosmetic result.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.