
Abstract
Introduction:
The widespread use of robotic surgery has provided surgeons a high-quality and alternative method to perform pyeloplasty. Indeed, robot-assisted technology has made it a lot easier to obtain the advanced technical skills required to perform this procedure. The learning curve (LC) reflects the increase in learning as a function of experience. Robot-assisted laparoscopic pyeloplasty (RALP) represents a well-standardized and reproducible procedure with an LC that allows reliable results to readily be obtained. The aim of our study was to compare the RALP LC of senior versus junior surgeons.
Materials and Methods:
We reviewed all of the RALP procedures performed at three pediatric surgery centers between November 2007 and November 2018. Three senior surgeons and 4 junior surgeons performed the robotic procedures. Neither the senior nor the junior surgeons had previous experience with robotic surgery; they had experience with conventional laparoscopic procedures but not with laparoscopic pyeloplasty. The primary metric that we selected to evaluate competence acquisition was a composite outcome defined by a combination of operative time (OT), complications, and surgical success. The complications were rated according to the Clavien–Dindo classification expressed by a complication factor; surgical success was expressed as a success factor, and we used a cumulative sum (CUSUM) analysis to determine the LC. The CUSUM method, through its multioutcome approach, is a very effective way to evaluate LCs.
Results:
Between November 2007 and November 2018, 3 senior surgeons and 4 junior surgeons performed 88 RALP procedures. The included patients had a median age of 6.1 years (range 7 months–16 years). The median duration of follow-up was 6.4 years (range 14 months–12 years). The median OT was 198.86 minutes (range 106–335 minutes). By CUSUM analysis of the composite outcome, we found that despite the junior surgeons having performed fewer procedures than the senior surgeons, their LCs exhibited an earlier inflection point (Fig. 1) followed by a constant rate of improvement in proficiency, thus indicating a more rapid learning process. The median composite scores for the senior surgeons and the junior surgeons were 299 (range 210–370) and 193 (range 131–255), respectively, after seven procedures.
Conclusion:
Assuming proper exposure to robotics and an adequate case volume, we demonstrated that junior surgeons can readily achieve comparable levels of expertise compared with senior practitioners in the field of pediatric RALP. It can be assumed that the LC in robotic pyeloplasty is not only directly influenced by the individual surgical experience but also by the experience of the surgical team.
Introduction
Dismembered pyeloplasty, first described by Anderson and Hynes in 1949, 1 has long been the gold standard for the treatment for ureteropelvic junction obstruction (UPJO) in children.
With the advent of laparoscopic surgery, minimally invasive treatment options for UPJO have been developed and widely used. Laparoscopic pyeloplasty has been shown to be associated with a shorter hospital stay and a lower rate of complications, but prolonged operative times (OTs), compared with open surgery. 2
Learning laparoscopic pyeloplasty is subject to a steep learning curve (LC), which has limited its uptake in common practice. The introduction of robotic surgery has provided surgeons a high-quality and alternative method to perform pyeloplasty. Indeed, robot-assisted technology has made it a lot easier to obtain the advanced technical skills required to perform this procedure. Robot-assisted laparoscopic pyeloplasty (RALP) is becoming increasingly widespread, presently accounting for more than 80% of all minimally invasive surgery pyeloplasties, and thus potentially becoming the new gold standard for UPJO treatment.3,4
The LC reflects the increase in learning as a function of greater experience. 5 This concept is of great importance in surgery, and there have been an increasing number of studies regarding the LC in robotic surgery. RALP represents a well-standardized and widespread procedure with an LC that allows reliable results to readily be obtained.
The aim of our study was to compare the RALP LC for senior versus junior surgeons. Most of the previous studies regarding the RALP LC used the OT as the sole predictive factor to define proficiency acquirement. 6 We adopted a multidimensional approach that took into account not only the OT but also the complication rate and patient outcome, using a cumulative sum (CUSUM) method.
Materials and Methods
This study was approved by the Institutional Review Board of Limoges Universitary Hospital.
We reviewed all of the RALP procedures performed at three pediatric surgery centers between November 2007 and November 2018. The data were reviewed retrospectively after being collected prospectively. Patients undergoing redo-pyeloplasty were not excluded from the study.
Three senior surgeons and 5 junior surgeons performed the robotic procedures. The data for one of the junior surgeons were excluded from the study because the number of procedures was not enough to define an LC. The surgical robotic teams were the same for both senior and junior surgeons. Both the senior and the junior surgeons did not have previous experience with robotic surgery; they had experience with conventional laparoscopic procedures but not with laparoscopic pyeloplasty. Before starting the robotic procedures, the surgeons and the chief operating nurses underwent a brief robotic surgery training session.
Operative technique
The indications for RALP were symptomatic UPJO, a progressive reduction in renal function with or without urinary tract infections, and an increasing anteroposterior pelvis diameter. All of the patients were preoperatively investigated with renal ultrasonography (US) and a diuretic MAG3 scan.
The surgical procedure was a transperitoneal Anderson–Hynes dismembered pyeloplasty. The patient was placed in lateral decubitus and four or five trocars were placed (Fig. 1). After colon detachment, the ureter was identified and dissected together with the pelvis and the UPJ. The pelvis was divided together with the ureter, which was spatulated by incision of its posterior margin. The pyeloplasty was performed with a running absorbable suture after placement of a Double-J stent.

Patient, robotic console, and patient cart position. The patient is in 60° lateral decubitus and the cart is placed alongside the bed with the robotic arms approaching him from behind; a dual-console is available allowing 2 surgeons to cooperate. In the figure example, the patient is in 60° left lateral decubitus to be operated on the right side.
Parameters of the LC and statistical analysis
The primary metric that we selected to evaluate competence acquirement was a composite outcome defined by a combination of the OT, complications, and surgical success. 7
The OT was defined as the time from the first incision to abdominal closure.
The complications were rated according to the Clavien–Dindo classification, 8 expressed as a complication factor (Fc) graded as follows: no complications = 1; Clavien 1 complications = 1.1; Clavien 2 complications = 1.2; Clavien 3A complications = 1.4; and Clavien 3B complications = 1.6; no Clavien 4/5 complications were recorded.
Surgical success was defined as hydronephrosis disappearance, improvement or stability on US, resolution of the symptoms with no evidence of a further decline in renal function, and no need for further intervention. The success factor (Fs) was graded as 0 for failure and 1 for a successful outcome of the surgery.
We used a CUSUM analysis to determine the LC. This is a statistical method that is very efficient at determining small shifts in the mean of a process.9,10 According to the principles of Montgomery, we defined the CUSUM score of the first case as the difference between the first case outcome and the target outcome for all cases. The CUSUM score for the second case was the summation of the previous cases' CUSUM added to the difference between the second case outcome and the target outcome for all the cases. This operation was applied in all of the cases. The target outcome was set at 200 minutes.11,12
We calculated the composite factor using the following equation:
Thus, the composite factor is 200 when there are no complications and the surgery is successful. When, instead, there are complications, the composite factor increases exponentially, thus giving due weight to the complications and not only to the OT. 7
The Student's t-test was performed for the parametric continuous data (the means and the standard deviations are presented), and the Mann–Whitney test for the nonparametric continuous data (the medians are presented). A P value <.05 was considered significant.
Results
Between November 2007 and November 2018, 92 patients underwent RALP for UPJO. Eight-eight patients, with a mean age of 6.1 years (range 7 months–16 years), were included in our study. The youngest patient in the series was 8 months old and the smallest patient weighed 7.1 kg. The mean OT was 198.86 minutes (range 106–335 minutes), without a significant difference between the senior and the junior surgeons (199.16 versus 198.15; P = .78). The postoperative complications were rated according to the Clavien–Dindo classification and comprised 7 cases that were grade III (5.4%), 3 cases that were grade II (2.3%), and 1 case that was grade I (0.77%). Conversion occurred in 3 cases (2.3%) (Table 1). No patient was lost to follow-up, and the median duration of the follow-up was 6.4 years (range 14 months–12 years).
Patient Characteristics
CUSUM, cumulative sum.
LC analysis
The median number of procedures for the senior surgeons was 20 and for the junior surgeons it was 7.
We calculated the composite factor of each surgeon, and through a COMPOSIT analysis we defined a CUSUM LC for each of them. We then calculated an average composite factor (Fig. 2) and an average CUSUM score (Fig. 3) for the first 15 procedures for the senior surgeons and for the first 7 procedures for the junior surgeons.
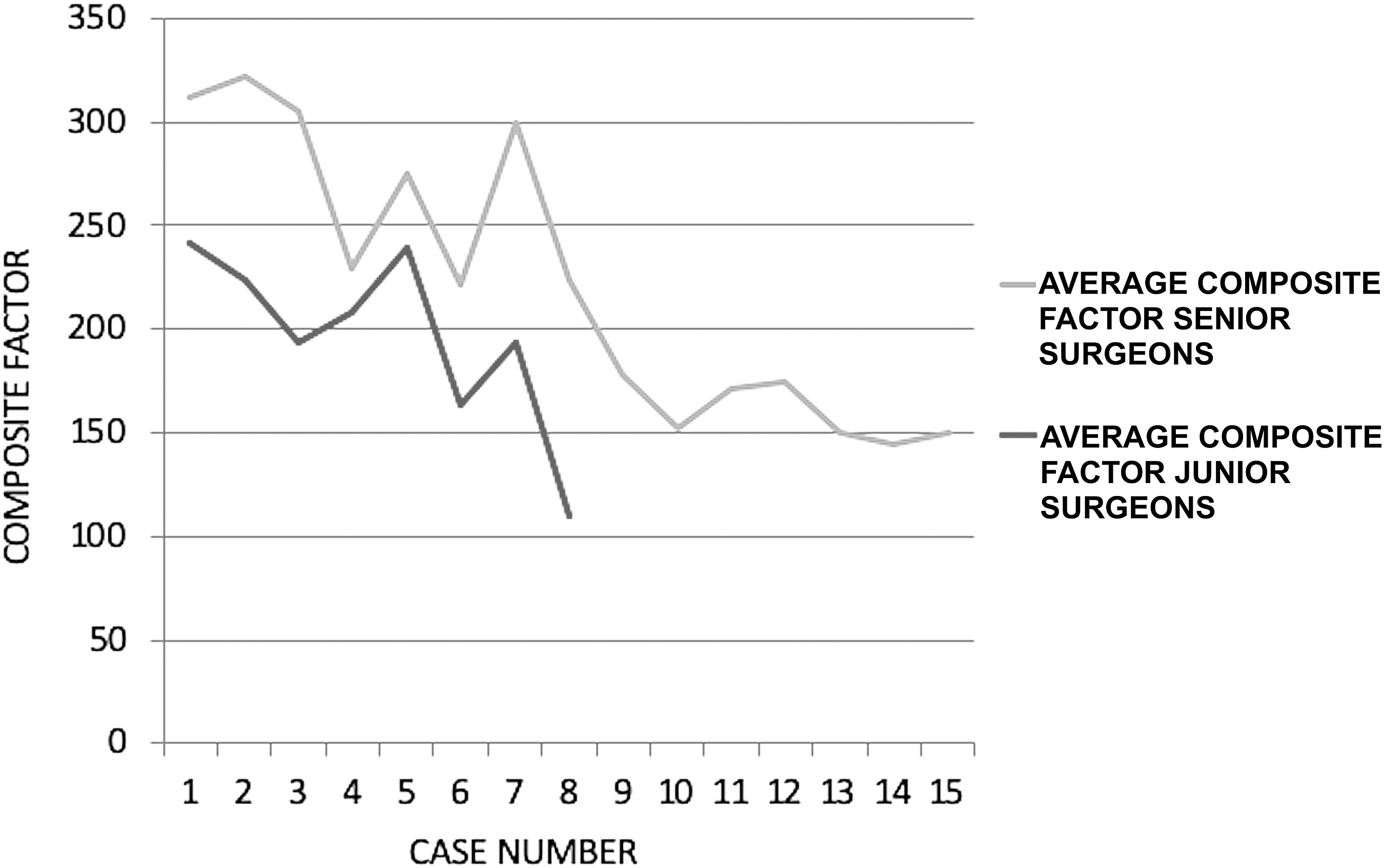
Composite factor. The raw average composite factor plotted versus the case number for the senior and the junior surgeons.
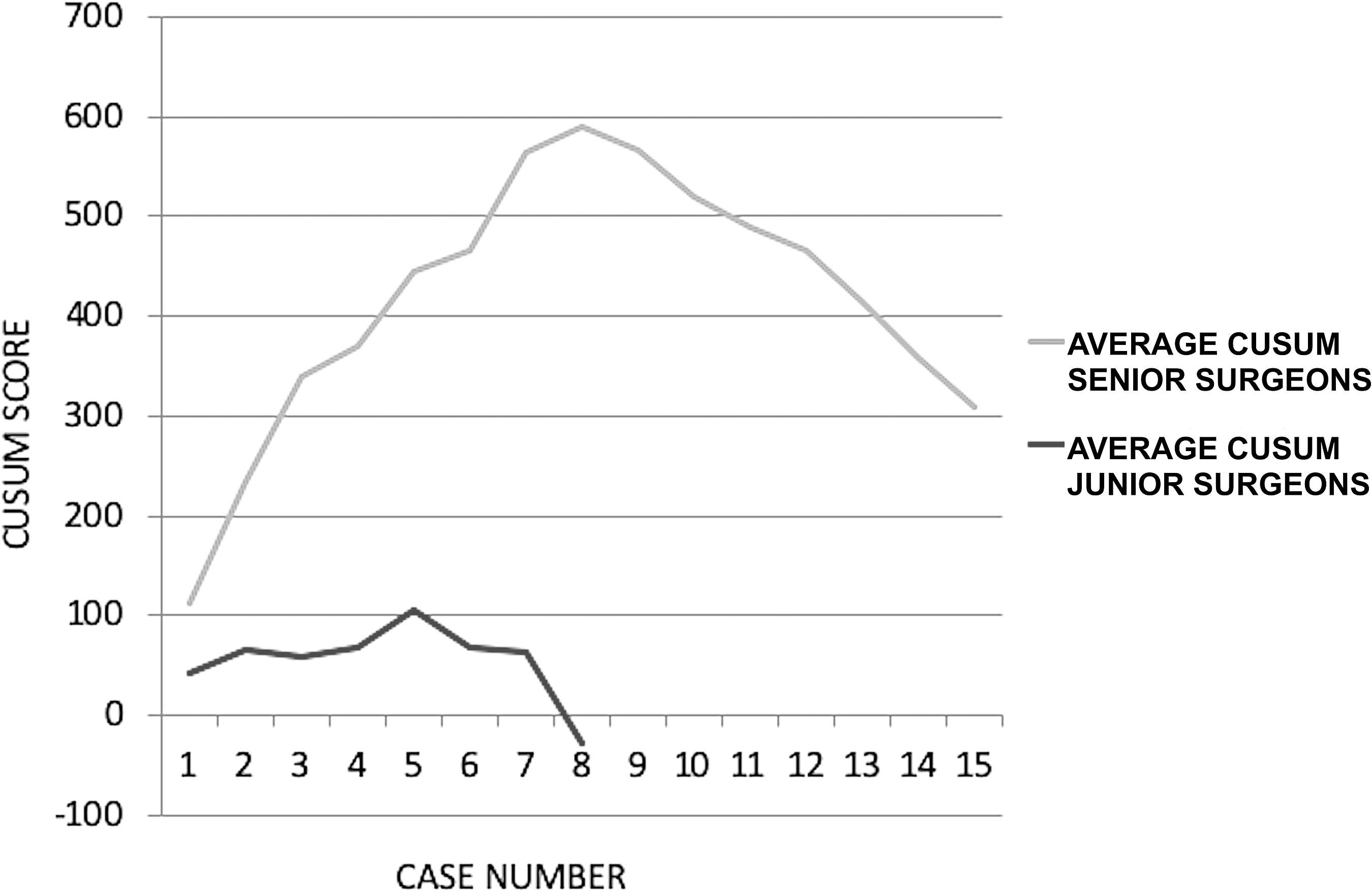
CUSUM. The average CUSUM chart for the composite factor plotted against the case number for the senior and the junior surgeons. CUSUM, cumulative sum.
By comparing the curves, it can be seen that despite the junior surgeons having performed fewer procedures than the senior surgeons, their LCs exhibited an earlier inflection point followed by a constant rate of increase in proficiency, thus reflecting a more rapid learning process.
No overall difference was found for the two groups regarding the mean composite factor: the scores for the senior and the junior surgeons were 220.6 ± 13.2 and 207.4 ± 18.7, respectively (P = .48). The median CUSUM score was significantly higher for the senior surgeons compared with the junior surgeons, at 444.0 versus 63.8, respectively (P < .01).
Discussion
This is the first study to compare senior versus junior surgeons, and a surprisingly better result was found in the latter group. The LC of the junior surgeons was faster compared with the senior surgeons. The difference between the two LCs is particularly apparent in the CUSUM chart.
LCs and UPJ in children
Several studies have been published regarding LCs for pediatric RALP as it is a well-standardized and widespread procedure.6,7,12–20 Most of these studies took into account the OT to define the LC, which is certainly the most important parameter, although surgical success and the complication rate also warrant being taken into account.
The first analysis of the RALP LC in the literature was carried out by Sorensen et al. 13 They compared the LC of RALP and open pyeloplasty. The procedures were performed by 2 pediatric urologists with extensive laparoscopic experience. Their LCs were only defined by the OT, but the authors also emphasized that the majority of the complications occurred with the first 5 cases.
Most of the other articles assessing the LC of RALP in children analyzed cases performed by a single experienced surgeon12,14,15,18,19 or at most by 3 expert surgeons.7,17,20
To the best of our knowledge, the only attempt, before the present study, to analyze the LC for junior surgeons was carried out by Tasian et al. 16 They analyzed the LCs of 4 fellows and compared these with the LC of an attending surgeon. This study suffered from two main limitations: the fellows did not perform the procedures entirely on their own, and the LC was only defined by the OT.
Most publications of RALP mention their complications and other measures of outcomes such as the length of the hospital stay or the need for postoperative analgesia. However, they did not statistically analyze any of these factors to define an objective LC.
Advantages of the CUSUM analysis
The OT, the surgical success, and the complication rate can be accurately expressed as the composite factor (OT x Fc x Fs). These raw data can then be transformed by the CUSUM analysis into trends of data deviation from their group mean. CUSUM analysis appears to allow for a more sensitive analysis of the LC. Indeed, it has a high sensitivity for detecting when outcomes deviate from the defined target. 11 This type of statistical analysis has only been used in a small number of studies addressing learning-phase transition points.7,12
Cundy et al. 12 used the CUSUM method to analyze various parameters of the OT such as the setup time, the docking time, the console time, the operating time, the total operating room time, and the complications. They created CUSUM charts for each of these parameters and they showed that the CUSUM method has ample potential for LC evaluation and definition of various learning-phase transition points.
Kassite et al. 7 made the first attempt to objectively define the LC by CUSUM analysis of a composite factor defined by the OT adjusted for the patient's complexity, the surgical success, and the complication rate. They analyzed the data from 2 experienced surgeons and they found that the LC for RALP can be divided into three different phases: the learning period, or phase 1 (1–12 cases); the consolidation period, or phase 2 (13–22 cases); and the period of increased competence, or phase 3 (23–39 cases).
Robotic surgery pioneers versus the second generation of surgeons
The novelty of our study lies with the comparison of two groups: the pioneers of robotics and the second generation of robotic surgeons. To the best of our knowledge, there are no data in the literature comparing these 2 surgeon populations. From the very beginning, the junior surgeons had a shorter OT and a lower rate of complications; the latter playing a big role in determining the variations of the CUSUM factor. This trend was maintained until an inflection point occurred at approximately the fifth procedure for the junior surgeons and at approximately the eighth procedure for the senior surgeons, followed by a constant rate of increasing proficiency. These results indicate that junior surgeons learn faster than experienced ones, while also exhibiting a lower complication rate. However, this interpretation needs to take into account that as assistants to the senior surgeons, the junior surgeons may have derived significant benefit from this previous operating room experience. In fact, junior surgeons started operating on their own only after senior surgeons and they previously integrated the team through the dual-console.
Before independently performing surgical procedures, junior surgeons have the opportunity to repeatedly assist experienced surgeons, after which they receive training and then perform the procedure while being supervised. This allows them to gain experience and hence learn faster than the senior surgeons who did not have this opportunity for learning. 21 The advent of a dual-console da Vinci SI Surgical System provides a great method to reduce the time involved in the learning process. This device provides trainees with more exposure and experience in robotic surgery by allowing them to cooperate with experienced surgeons while under their direct supervision. 22
Laparoscopy is nowadays commonplace in nearly all hospitals in the world so that new generations of junior surgeons are being inducted into this minimally invasive environment. In addition to laparoscopy, they are exposed to robotic surgery at an early stage in their medical training.
Junior surgeons no doubt benefit from the experience of the whole team, as a result of which they rapidly achieve levels of expertise comparable with senior surgeons. Our study has a number of limitations. In addition to the limited number of included cases, there was also a difference in the number of cases performed by the junior versus the senior surgeons. This means that only the first phase of the two LCs can be compared. Future studies should hence include a larger number of cases to compare all of the phases of these LCs to obtain more reliable and comprehensive results.
Conclusion
Assuming proper exposure to robotics and adequate case volumes, we demonstrated that junior surgeons can rapidly achieve levels of expertise comparable with those of senior practitioners in the field of pediatric RALP. It can be assumed that the LC in robotic pyeloplasty is not only directly influenced by individual surgical experience but also by the experience of the whole surgical team. Moreover, the CUSUM method represented an excellent way to approach the LC as objectively as possible by combining different parameters. As our unexpected result that “junior surgeons learned faster than seniors” only applies to the first phase of the LC, further studies should evaluate the entire LC with the aim of substantiating our results.
Comparison of the data for the senior and the junior surgeons was regarding patient numbers, OT, complications rated according to the Clavien–Dindo classification, 8 the CUSUM, and the composite factor after seven procedures.
The patient is in 60° lateral decubitus and the cart is placed alongside the bed with the robotic arms approaching him from behind; a dual-console is available allowing 2 surgeons to cooperate. In the figure example, the patient is in 60° left lateral decubitus to be operated on the right side.
Footnotes
Acknowledgment
The authors thank R. Peymirat for his technical assistance with image editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.