
Abstract
Background:
Obesity is one of the contributing factors to technical difficulties in minimally invasive colorectal surgery. However, there are no data regarding the outcomes for obese patients undergoing robotic complete mesocolic excision (CME) for colon cancer. In this study, we aimed to investigate whether robotic CME in obese patients can be performed with similar morbidity and pathological results compared with nonobese patients.
Methods:
Patients who underwent robotic CME between 2014 and 2019 were classified into obese and nonobese groups. Obesity was defined as body mass index ≥30 kg/m2. Demographic data, perioperative outcomes and pathological results were compared between the groups.
Results:
There were 42 and 105 patients in the obese and nonobese group, respectively. The groups were comparable regarding preoperative characteristics. There were no significant differences with respect to operative times (244 ± 64 versus 304 ± 75 minutes, P = .29), blood loss (median, 50 versus 80 mL, P = .20), intraoperative complications (0% versus 3.8%, P > .99), and conversions (0% versus 1.9%, P > .99). No differences were detected in length of hospital stay (6 ± 1 versus 6 ± 2 days, P = .73), anastomotic leak (2.4% versus 1.9%, P > .99), septic complications, reoperations (2.4% versus 3.8%), and readmissions (2.4% versus 2.9%) (P > .05). The mean number of harvested lymph nodes (33 ± 11 versus 34 ± 13, P = .79), resection margin status, and mesocolic fascia grading were similar.
Conclusion:
Robotic CME in obese patients can be performed with a similar morbidity and pathological profile compared with nonobese patients. The Clinical Trial Registration number is not applicable for this study.
Introduction
In the past three decades, there have been significant advances in the treatment of colon cancer after the introduction of complete mesocolic excision (CME) and technological improvements in minimally invasive surgery.
In CME surgery, similar to the principles of total mesorectal excision, the entire mesocolon is removed in the embryological planes to create an intact envelope of the mesocolic fascia, and the main artery pedicle is ligated at the root to maximize lymph node harvest. 1 Data indicate that CME is associated with better survival than is conventional colon cancer resection.2,3 From the technical standpoint, CME surgery has gradually evolved from its first description of open approach to laparoscopy, and finally, to robotic approach with acceptable oncologic profile and postoperative outcomes. The technical advantages of robotic systems over laparoscopy have further revolutionized minimally invasive approach in CME surgery. 4
As is widely known, obesity is one of the common contributing factors to technical difficulties in the performance of minimally invasive colorectal cancer surgery.5,6 Accordingly, it may also present challenges in robotic CME procedure. However, no study to date has evaluated the outcomes for obese patients undergoing robotic CME surgery. In this study, we therefore aimed to investigate whether robotic CME in obese patients can be performed with similar morbidity and pathological results compared with nonobese patients.
Materials and Methods
Patients
After obtaining approval from the Institutional Review Board (IRB No. 2019-18/39), we evaluated prospectively collected data of consecutive patients undergoing robotic CME for colon adenocarcinoma between December 2014 and December 2019. Research electronic data capture (REDCap) 7 was used for data collection. Patients with American Society of Anesthesiologists (ASA) score >3, colonic cancer types other than adenocarcinoma, appendiceal or rectosigmoid junction tumors, and synchronous colonic tumors were excluded. Patients were divided into two groups as obese and nonobese. Patients with a body mass index (BMI) ≥30 kg/m2 were accepted as obese according to the recommendation of the World Health Organization. 8 We defined right-sided cancers as those located between the cecum, and mid-transverse colon and left-sided cancers between the distal transverse colon and sigmoid colon. The two groups were compared for the clinical characteristics, pathological findings, and postoperative 30-day outcomes.
Preoperative clinical data collected included patient demographics, ASA status, BMI, tobacco use, comorbidities, previous abdominal surgery, neoadjuvant chemotherapy use, and tumor site. Intraoperative data included surgical procedure classified as right-, left-sided and subtotal colectomy, indocyanin green fluorescent (ICG) imaging to check anastomotic perfusion, site, type and configuration of anastomosis, diverting stoma formation, intraoperative complications, conversions, operative time and blood loss. Postoperative outcome data included time to the first bowel movement and oral diet intake, length of hospital stay and postoperative morbidity within 30 days, including anastomotic leak, surgical site infections (SSIs), sepsis, ileus, bleeding, cardiac and pulmonary complications (atelectasis, pneumonia, pulmonary thromboembolism), readmission, reoperation, and mortality. Complications were classified according to the Clavien–Dindo classification. 9 Focusing on pathological outcomes, data included disease stage, tumor size, specimen length, surrogate oncologic measures, including length of surgical margins to tumor, surgical margin positivity, total number of lymph nodes retrieved, and mesocolic fascia grading.
Operative time was defined as the time from the first skin incision to the end of skin closure. Conversion was defined as the completion of any part of the robotic procedure with a standard laparoscopic or open technique, excluding the delivery of the specimen. Anastomotic leak was defined as clinically apparent leak sign (such as the emission of gas, pus, or feces from the drain) or extravasation of an endoluminally administered water-soluble contrast medium according to the postoperative computed tomography scan.
Preoperative preparation
Bowel preparation protocol included a clear liquid diet and 90 mL Na-phosphate soda and enema the day before surgery. All the patients received venous thrombosis prophylaxis with compressive elastic stockings 12 hours, antibiotic prophylaxis 1 hour before the operation. After induction of general anesthesia, a nasogastric tube and a urinary catheter were placed.
Robotic CME procedure
Operations were performed by three highly experienced robotic colorectal surgeons (T.K., I.H., and B.B.) using the full robotic approach with the da Vinci Xi platform (Intuitive Surgical, Inc., Sunnyvale, CA). The medial-to-lateral dissection and intracorporeal bowel anastomosis techniques were employed, and resections were performed to achieve ∼10-cm proximal and distal tumor-free margins. The technical details of robotic CME procedures for right- and left-sided colonic cancers are described in our previous publications.10,11 Vascular dissection in a right hemicolectomy procedure and the surgical specimen are presented in Figures 1 and 2, respectively.
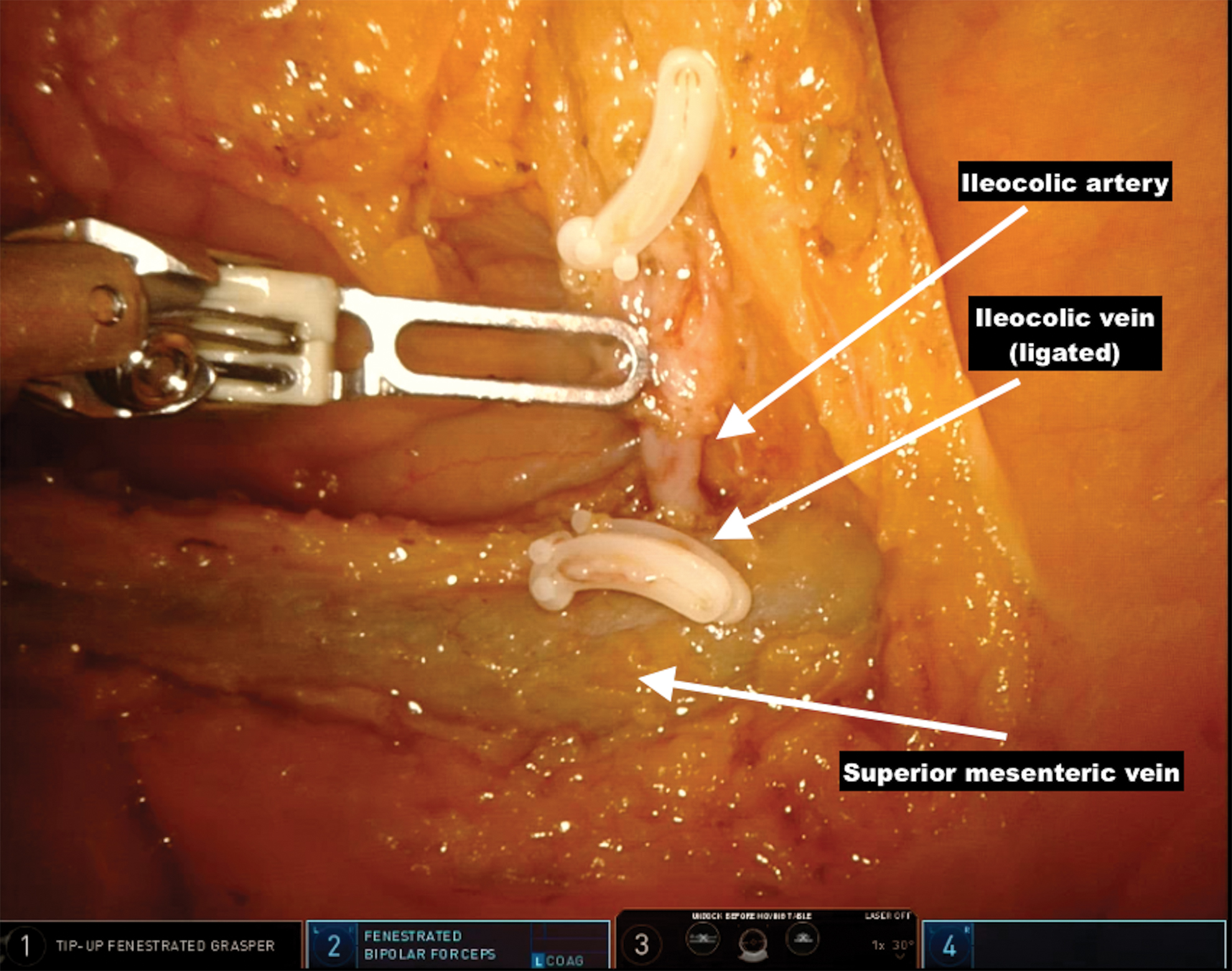
Vascular dissection during robotic right hemicolectomy procedure in an obese patient. Color images are available online.
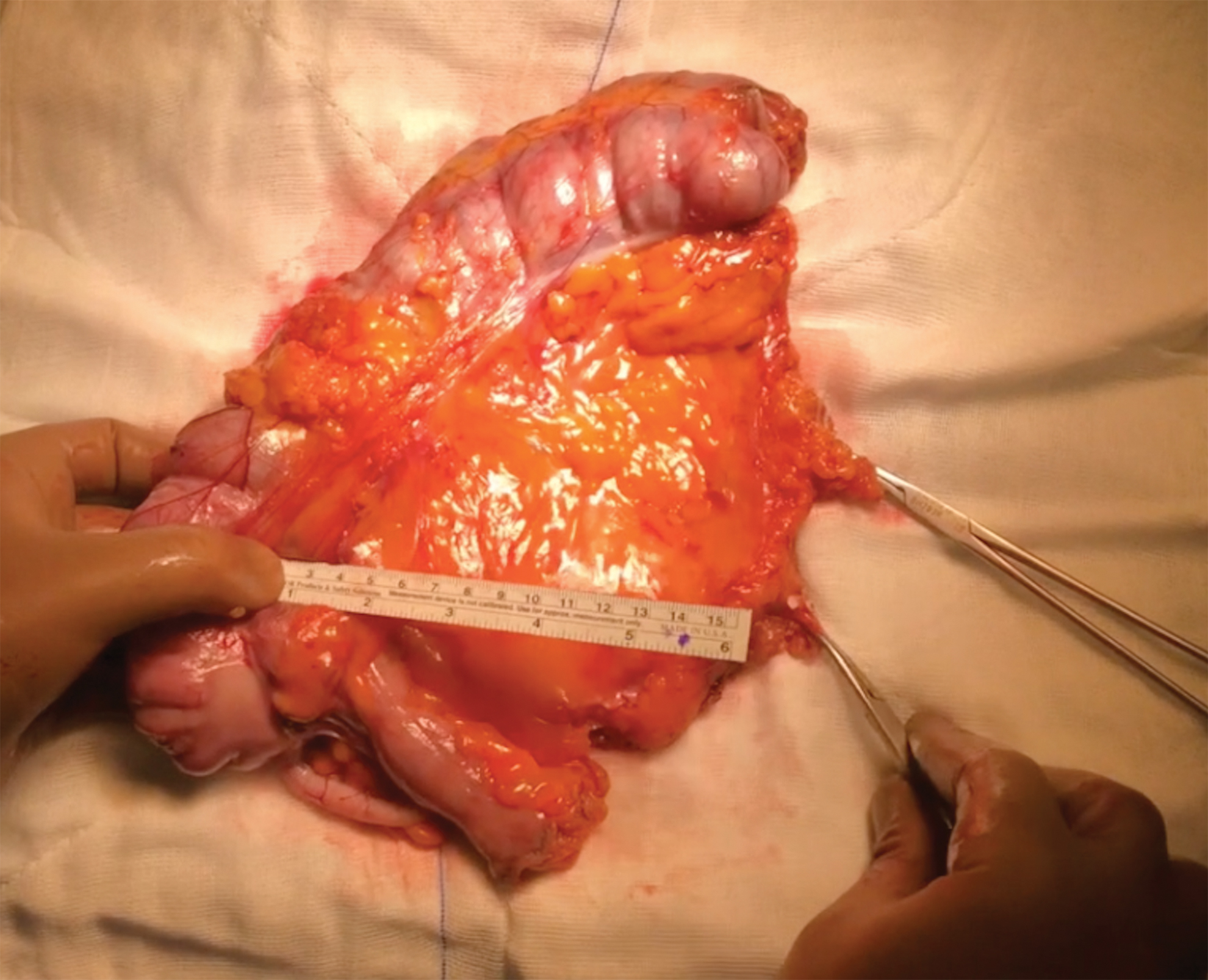
View of robotic right hemicolectomy specimen in an obese patient. The specimen is examined for the quality of mesocolic dissection, distance between the vascular tie and tumor, and distance between the vascular tie and colonic wall. Color images are available online.
Postoperative course
Intravenous narcotics were administered as needed for pain control. Removal of nasogastric tube and start of oral intake were determined on the basis of return of bowel movement. Discharge criteria were sufficient oral intake with documented bowel or stoma function, full ambulation, and adequate pain control with oral analgesics.
Statistical analysis
Statistical analysis was performed using the SPSS 22.0 software package (IBM Corp., Armonk, NY). Categorical variables were analyzed using absolute and relative frequencies. Group comparisons for categorical variables were conducted by the chi-square test with or without Yates' correction or Fisher's exact test. Continuous variables were analyzed using either mean ± standard deviation or median (range) depending on the normality assumption assessed by the Kolmogorov–Smirnov test. The variables that approximated to a normal distribution were compared by Student's t-test, while the ones departed from the normal approximation were compared by the Mann–Whitney U test. A P value <.05 was considered significant.
Results
A total number of 147 patients (males, 61%) met the inclusion criteria. Overall, the mean age of the patients was 63.1 ± 11.7 years, and the mean BMI was 27.4 ± 4.6 kg/m2. Right- and left-sided cancers were identified in 52 and 95 patients, respectively. Of these 147 patients, there were 42 (28.5%) patients in the obese group and 105 patients in the nonobese group.
Preoperative characteristics of the patients are presented in Table 1. There were statistically no significant differences between the groups regarding age (66.4 ± 10.5 versus 63.4 ± 12.3 years), gender (males/females: 59.5%/40.5% versus 61.9%/38.1%), ASA scores, tobacco use, comorbidities, albumin level, previous abdominal surgery (35.7% versus 39%), site of tumor, and neoadjuvant chemotherapy use (P > .05). Sigmoid colon was the most common tumor localization followed by cecum in both groups.
Comparison of Preoperative Patient Characteristics Between the Groups
ASA, American Society of Anesthesiologists; SD, standard deviation.
Regarding the intraoperative outcomes (Table 2), the types of surgical procedures were similar between the groups (right-sided resections, 47.6% versus 27.6%; left-sided resections, 52.3% versus 68.6%; and subtotal colectomies, 0% versus 3.8%, P = .09). No significant differences were detected in the rate of ICG fluorescent imaging, site, type and configuration of bowel anastomosis, and diverting ileostomy creation (4.8% versus 3.9%). Anastomosis was not created in one patient with splenic flexure cancer in the nonobese group due to colonic dilatation. The operative times (244.5 ± 64.9 versus 304.3 ± 75.7 minutes) and operative blood loss (median, 50 versus 80 mL) were similar. Considering intraoperative complications, there were none in the obese group and 4 in the nonobese group (0% versus 3.8%, P > .99). These complications were left renal vein injury in 1 patient, gonadal vein injury in 1, small bowel wall injury in 1, and partial detachment of colorectal anastomosis during removal of a circular staple in 1 patient. All these complications were managed robotically except for the left renal vein injury, which was repaired uneventfully after converting this case to laparotomy. There were no conversions in the obese group and 2 in the nonobese group with no statistical significance (0% versus 1.9%, P > .99): 1 patient with intraoperatively detected liver metastasis required conversion to laparotomy for metastasectomy, and the other was converted due to the aforementioned renal vein injury.
Comparison of Intraoperative Outcomes Between the Groups
Anastomosis was not performed in 1 patient in the nonobese group, thus this patient was excluded from the analyses.
ICG, indocyanin green fluorescent; SD, standard deviation.
The postoperative 30-day outcomes are detailed in Table 3. There were no significant differences with respect to the mean time to the first flatus and bowel movement, oral intake, length of hospital stay (6.1 ± 1.8 versus 6.7 ± 2.9 days), and readmissions (2.4% versus 2.9%). Overall, anastomotic leak occurred in 3 patients (2.4% versus 1.9%, P > .99), and all these cases were managed with diverting stoma creation. Postoperative bleeding occurred in a nonobese patient who had primarily developed an abscess in the lesser omental sac that required a percutaneous drainage. Due to hemodynamic instability in this case, an emergency laparotomy was performed, and the bleeding from the mesocolic site of the abscess cavity was controlled with sutures. Reoperation was performed in 1 patient in the obese group (diverting stoma creation due to anastomotic leak) and 4 patients in the nonobese group (diverting stoma creation due to anastomotic leak in 2 patients, emergency laparotomy for bleeding in 1 patient, and wedge resection and omentoplasty for duodenal leak in 1 patient who had undergone duodenal partial seroza resection for duodenal invasion of tumor during the index CME procedure; P > .99). Regarding other measures, there were no significant differences in SSIs, sepsis, ileus, cardiac, pulmonary, and urinary complications. No mortality occurred in either group. Based on the Clavien–Dindo classification scale, no differences were observed in the distribution of postoperative complications between the two groups (P = .79).
Comparison of Postoperative 30-Day Outcomes Between the Groups
SD, standard deviation; SSI, surgical site infection.
The pathological results revealed that the two groups were comparable in terms of TNM stage and tumor size. Regarding outcome measures, both groups had similar results in terms of mean number of harvested lymph nodes (33.6 ± 11.6 versus 34.6 ± 13.5), distance between tumor and proximal, distal, radial margins and vascular tie. Data on mesocolic fascia grading were available in 67 patients. No differences were detected with respect to the mesocolic fascia grading (Table 4).
Comparison of Histopathological Results Between the Groups
Data were available in 24 (57%) patients in the obese group and 43 (41%) patients in the nonobese group.
SD, standard deviation.
Discussion
In this study, we compared the perioperative short-term outcomes and pathological results of robotic CME for colon cancer in obese versus nonobese patients. The results of this study reveal that robotic CME when performed in obese patients neither increases intraoperative complications, postoperative morbidity nor adversely affects pathological results.
The current evidence suggests that CME is a better strategy to improve specimen quality and eradicate lymphatic metastasis, thus improving survival in patients with colon cancer.1,2,12 This is because CME is a more radical technique than conventional colectomy as it involves a more extensive mesocolic excision and a vascular ligation more distant from the tumor. Inherent to this technique, dissection is performed close to organs and vessels that are not usually fully exposed in conventional colectomy. Although some concerns have been raised about the technical difficulties and potential complications of CME procedure especially in minimally invasive surgery, the safety and feasibility of laparoscopy, and recently, robotic approach for right- and left-sided CME procedures have been demonstrated.10,11,13,14 Furthermore, in two recent studies it is reported that robotic approach allows for the completion of this technically difficult procedure without conversion, 4 and it is associated with a better lymph node yield than laparoscopic or open approaches, concluding that robotic surgery facilitates a better CME. 15 Considering its technical advantages over laparoscopy, we adopted the robotic approach 2014, and since then, have been increasingly employing this approach for CME procedure.
Obesity is known to be a significant risk factor for increased morbidity, including higher conversion rates and blood loss during laparoscopic colorectal surgery.5,6 On the contrary, compared with laparoscopy, robotic approach in obese patients is reported to be associated with fewer conversions and shorter length of stays in a nationwide American College of Surgeons National Surgical Quality Improvement Program study. 6 These results have been supported in a meta-analysis by Wee et al., 16 concluding that robotic surgery provides earlier recovery and reduced readmission rates without compromising other operative outcomes. However, no prior study to date has evaluated the impact of obesity in minimally invasive CME surgery. Problems associated with excessive adipose tissue such as bulky omentum and thickened mesentery decreased working space, suboptimal visualization, and difficulties in gaining access to the splenic and hepatic flexures may add to the technical difficulties of CME.
This is the first study to specifically investigate the impact of obesity on surgical outcomes after robotic CME procedure. Analysis of the obese and nonobese groups revealed similar preoperative clinical characteristics, tumor localizations, disease stages, rate of right- and left-sided resections, and intracorporeal anastomosis creation, suggesting that the two groups were well comparable. The incidence of perioperative complications is a crucial index used to evaluate the safety of a surgical procedure. Considering the intraoperative outcomes, no significant differences were detected between the groups with respect to conversions, complications, operative times, and blood loss. Regarding the postoperative outcomes, robotic CME in obese patients again resulted in similar patient recovery parameters, anastomotic leak, septic complications, other morbidities, length of stay, readmission, and reoperation rates compared with nonobese patients.
So far, there have been three published studies evaluating the impact of obesity in robotic colorectal surgery, and in all these studies, operations were performed for a variety of benign and malignant conditions. In the first study, Keller et al. 17 report similar operative times, intraoperative complications and conversion rates, length of stay, postoperative complication, readmission, and reoperation rates, concluding that robotic approach is a reasonable option to overcome the challenges and improve outcomes for obese patients. In the second study, Lagares-Garcia et al. 18 have shown that BMI has no significant effect on operative outcomes and quality of surrogate oncologic markers but prolongs the procedure during robotic surgery. Finally, similar outcomes have been reported by Harr et al., 19 suggesting that obese patients may see a greater benefit of robotic surgery than nonobese patients. This study provides a unique contribution to the literature that robotic surgery can also be safely performed in obese patients undergoing CME procedure for colon cancer. Of note, although not statistically significant, we notice a trend toward higher rate of conversions (1.9% versus 0%), overall intraoperative complications (3.8% versus 0%), longer operative times (304 versus 244 minutes), and more blood loss (80 versus 50 mL) in the nonobese group. Certainly, these parameters are expected to be inferior in obese patients. We assume that these findings may be due to the smaller sample size of 42 obese as opposed to 105 nonobese patients. Additional studies with larger cohorts would be useful to verify our findings.
From the oncologic standpoint, the key concepts of CME as suggested by Hohenberger et al. 1 were successfully applied to the obese as well as to the nonobese patients. No significant variability in surrogate oncologic markers such as the number of harvested lymph nodes, resection margin status, and mesocolic fascia grading shows that adequate CME resections can also be achieved in obese patients undergoing robotic surgery. This again emphasizes the value of robotic technology in this subset of patients.
All the CME procedures in this study were performed using the latest generation da Vinci Xi robot. Compared with its prior platforms, the Xi system has a range of the latest technologies that enable a wider range of motion and better anatomic access in the abdominal cavity. 11 We recognize that the use of this system helps surgeon to complete this operation successfully even in the presence of anatomical challenges due to obesity.
The results from this study must be interpreted considering the known limitations of its retrospective design although we used a prospectively collected database. In addition, the obese patient cohort is relatively small, thus results that are not significant in this study might show different trends or actually reach significance with more powered data. Operations were carried out by three surgeons with significant experience in robotic colorectal surgery, and this could limit the generalizability of our outcomes. Finally, mesocolic fascia grading is known to be an important factor for the quality of CME surgery and survival. 20 Although the mesocolic fascia grading was similar between the groups, this conclusion should be read with caution since this parameter was available in 46% of the patients in this study.
Conclusion
Our results show that robotic CME in obese patients is safe, and can be performed with similar morbidity and pathological profile compared with nonobese patients. The technical advantages of robotic platforms likely mitigate the surgical challenges associated with obesity. Additional studies would provide further insights on the impact of obesity in robotic CME.
Ethical Approval
This study was approved by the Institutional Ethics Committee.
Footnotes
Authors' Contributions
V.O., Z.A., and B.B. contributed to conception of the work; V.O., Z.A., and I.A.B. performed data analysis; V.O and Z.A wrote the article; I.A.B., E.A., B.B., I.H., and T.K. contributed to revision of the article; B.B., I.H., and T.K. contributed to the operations.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.