
Abstract
Background:
Laparoscopic orchiopexy (LO) has become a standard procedure for the treatment of nonpalpable undescended testes (UDT). LO for palpable UDT is still controversial. The aim of this study is to explore the method and effect of LO procedure for palpable UDT in children suffering from cryptorchidism.
Methods:
A retrospective study was performed for LO and traditional inguinal incision orchiopexy (TIO) for palpable UDT. A total of 291 children were enrolled, and they were aged 9–96 months with either left- or right-side palpable inguinal canalicular testes. Patients with testes that were nonpalpable, ectopic, and retractable were excluded. One hundred seventy patients received LO and 121 patients received TIO. Patient age, operative time, and clinical outcomes were reviewed. Independent t-test and Fisher's exact test were performed by SPSS 25.0 software.
Results:
The mean operative time (30.77 ± 6.02 minutes versus 44.76 ± 6.70 minutes) and postoperative normal activity time (1.25 ± 0.43 days versus 2.48 ± 0.68 days) of LO were significantly shorter than those of TIO group (P < .05). Forty-seven of 49 cases (95.9%) aged <1 year successfully achieved LO.
Conclusion:
LO is an appropriate choice for palpable UDT, especially in younger children aged <2 years. The success rate of LO decreased with age.
Background
Cryptorchidism or undescended testes (UDT) are a common genital malformation in boys. In similar studies performed in different countries, the prevalence of cryptorchidism has varied from 2% to 8%. 1 The incidence of UDT of birth to premature and/or birth weight (<2500 g) infants varies from 1.1% to 45.3% and bilateral presentation was 50%–75%. 2 Nearly 80% of UDT are palpable. 3 Traditional inguinal incision orchiopexy (TIO) is recommended after 6 months of age. 4 Laparoscopic orchiopexy (LO) is a standard procedure for the treatment of nonpalpable UDT. 5 However, LO for palpable UDT is still controversial. The procedure is not recommended by any organization yet. Although many literatures have reported that the LO for palpable UDT is a great and safe option for patients with palpable UDT, regardless of the age and others.6,7 This study has compared LO with TIO in children with palpable UDT with our experience of the recent 5 years.
Materials and Methods
This study was approved by the Ethics Committee of The First People's Hospital of Lianyungang. From August 2014 to August 2019, a retrospective study of LO and TIO was conducted. A total of 291 children with either left- or right-side palpable inguinal canalicular testes were included (Table 1). Patients with testes that were nonpalpable, ectopic, and retractable were excluded. LO was performed on 170 patients aged 9–48 months (mean 16.62 ± 8.43 months), with 74 on the left side and 96 on the right. One hundred twenty-one patients aged 9–96 months (mean 18.37 ± 15.35 months) received TIO, with 50 on the left side and 71 on the right. All patients had unilateral palpable UDT and the testicles cannot be drawn into the scrotum in the physical examination. Patient age, operative time, the proportion of closure of internal inguinal ring (IIR), and clinical outcomes were reviewed. Follow-up visits were performed to assess the postoperative testes.
Patient General Data
Value indicates P value < .05 which was considered statistically significant.
Chi-square test was performed for the different side of the two groups.
Independent samples t-test was performed between the age of the two groups. LO, laparoscopic orchiopexy; TIO, traditional inguinal incision orchiopexy.
The patients were treated under general anesthesia, and then a supine position was taken. Tilt the operating table to 15°–20° with the head low and feet high. A 5-mm umbilical incision was made along the superior border of umbilicus. First, a 5-mm trocar was inserted into the umbilical incision. Carbon dioxide pneumoperitoneum was established routinely with pressures between 8 and 10 mmHg. The lens (30°) was placed into the abdominal cavities to explore the IIR. If the IIR was closed, transfer to the inguinal incisions. If the IIR was open, the other two 5-mm trocars were placed at the subcostal midclavicular line. Alternately using two graspers to pull the testes from the inguinal canal into the abdominal cavity. If the testicle can be pulled into the abdominal cavity, laparoscopic dissection and orchiopexy were performed. The gubernaculums testis (GT) was cut off in the abdominal cavity, then peritoneum around the IIR was cut off completely, the vessels and deferent duct were dissected for adequate testicular mobilization, and the testicle was retracted to the scrotum for orchiopexy using a clamp guided by a suction tube. The suction tube was inserted from the ipsilateral trocar, and then taken out from the scrotum incision through the inguinal canular. A clamp was inserted into the suction tube (Fig. 1), and then the suction tube was retracted. The clamp can be pushed into the abdominal cavity smoothly. After bringing the testis into the scrotum, 2–3 sutures were used to fix the testis inside the scrotum. If the testicle cannot be pulled into the abdominal cavity, it can be transferred to the inguinal incisions.
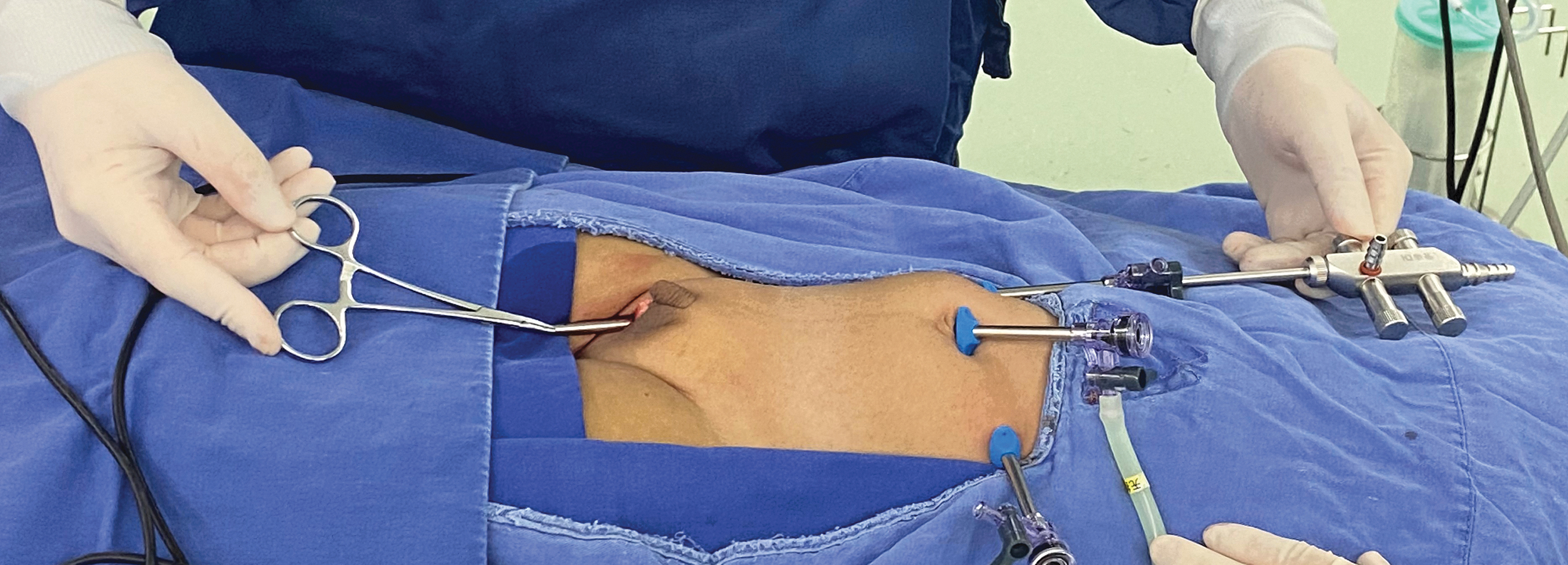
The testicle was retracted to the scrotum for orchiopexy by a clamp inserted from the scrotum guided by a suction tube.
In TIO group, the GT was cut off through an inguinal incision. Standard inguinal orchiopexy was performed. The operations of both groups were done by some surgeons in the same period.
The comparison of continuous data was conducted with independent t-test and categorical variables were compared with the use of chi-square test. All statistical analyses were performed by SPSS 25.0 software. Normality of data was checked before the t-test (if normal distribution was not obeyed, U-test was used). Chi-square test was performed (if n < 5 for cell(s), Fisher's exact test was performed).
Results
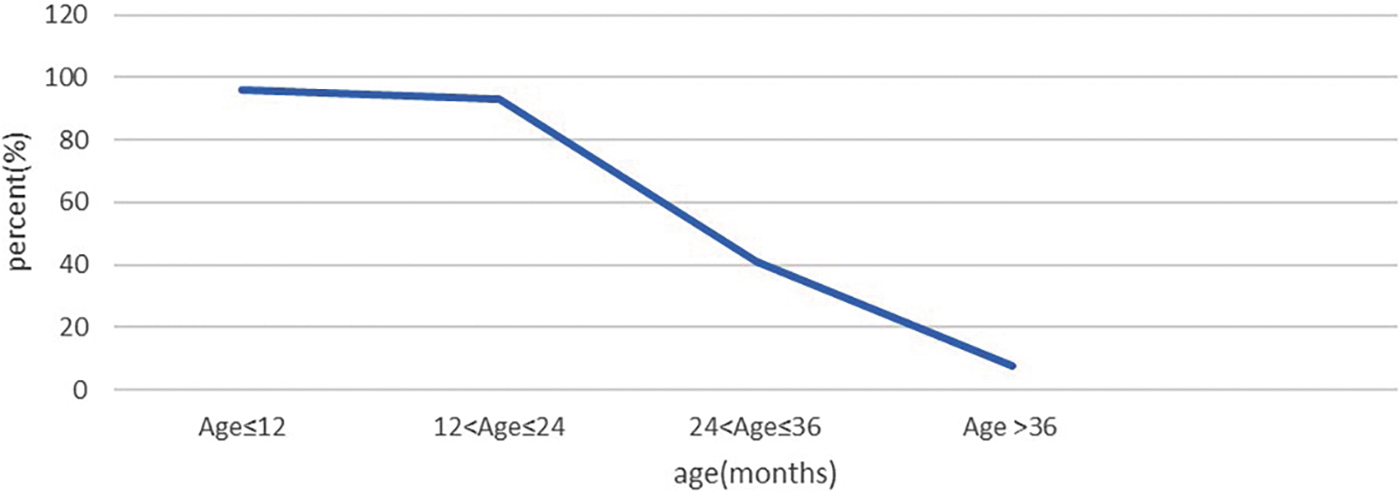
Among 170 patients who underwent laparoscopic exploration, 137 patients (80.5%) achieved LO without transfer to the inguinal incisions. Among them, 49 cases were aged <1 year, 48 cases (98.0%) had open IIR, and 47 cases (95.9%) successfully achieved LO, which took an average time of 30.77 ± 6.02 minutes. Among the 86 patients aged 1–2 years, 83 cases (96.5%) IIR were open, and 80 cases (93.0%) were successfully achieved LO. Among the 22 patients aged 2–3 years, 13 cases (59.1%) had open IIR, and 9 cases (40.9%) successfully achieved LO. Among 13 patients >3 years old, 3 patients (23.1%) had open IIR and only 1 patient (7.7%) successfully achieved LO. In all cases, the testicles were placed at the middle or bottom of the scrotum. Thirty-three cases were transferred to inguinal incisions since the IIR was closed. Ten cases were transferred to the inguinal incision because the testicle cannot be pulled into the abdominal cavity although the IIR was open (Figs. 2 and 3)

Proportion of open patent ring with age changing of LO groups. LO, laparoscopic orchiopexy.
The successful ratio of the testicle can be pulled into the abdominal cavity with age changing of LO groups. LO, laparoscopic orchiopexy.
The transferred 43 cases were still calculated in LO groups. The mean operative time of lower age groups (<1 year old, 30.50 ± 5.88 minutes versus 39.86 ± 6.11 minutes; 1–2 years old, 34.43 ± 6.65 versus 40.23 ± 8.74), and postoperative normal activity time (<1 year old, 1.20 ± 0.40 days versus 2.12 ± 0.48 days; 1–2 years old, 1.58 ± 0.50 days versus 2.02 ± 0.43 days) of LO were significantly shorter than those of TIO group (P < .05). The operative time of LO was significantly longer than that of TIO group in elder groups (age >3 years). There were no statistically significant differences in postoperative normal activity time between LO and TIO in elder groups (age >3 years) (Figs. 4 and 5). The follow-up was not different in two groups (Table 2).
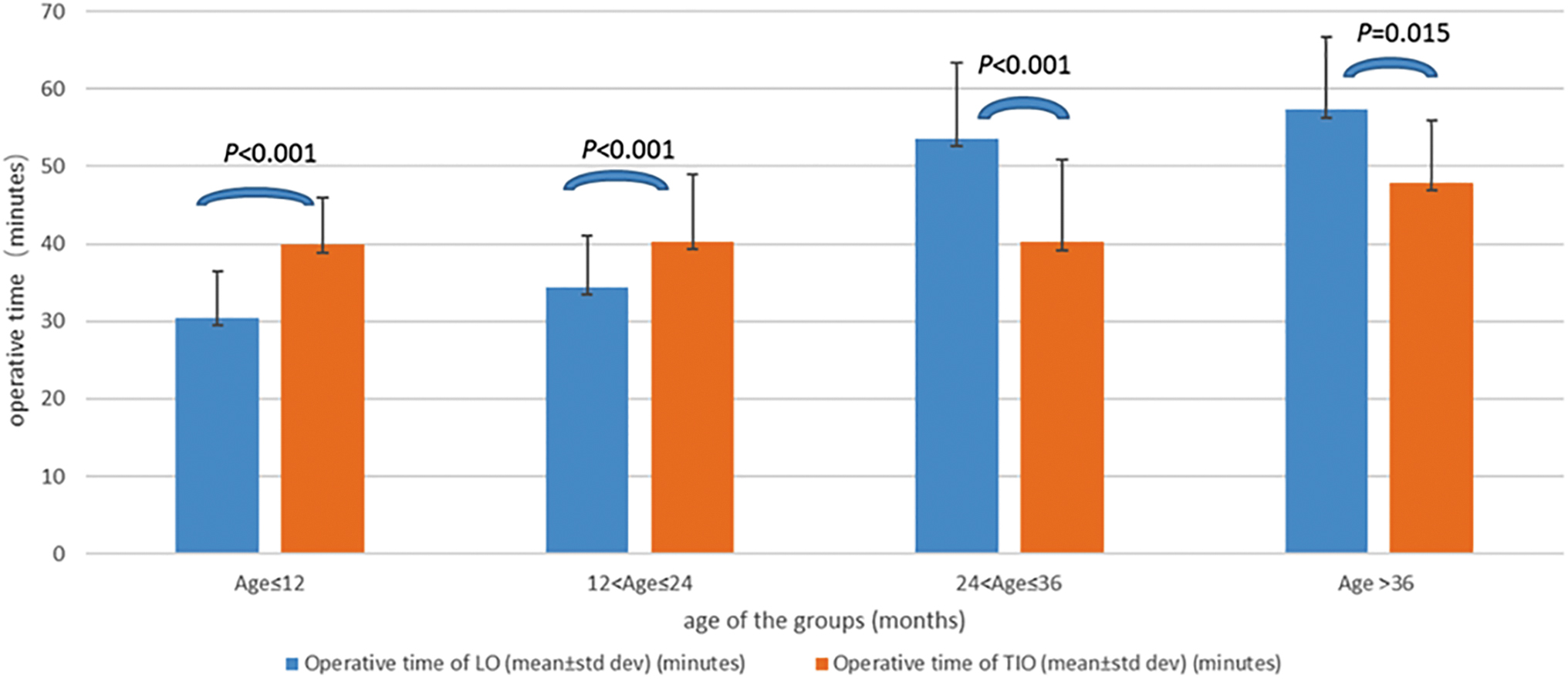
Comparison of operative time between LO and TIO. LO, laparoscopic orchiopexy; TIO, traditional inguinal incision orchiopexy.
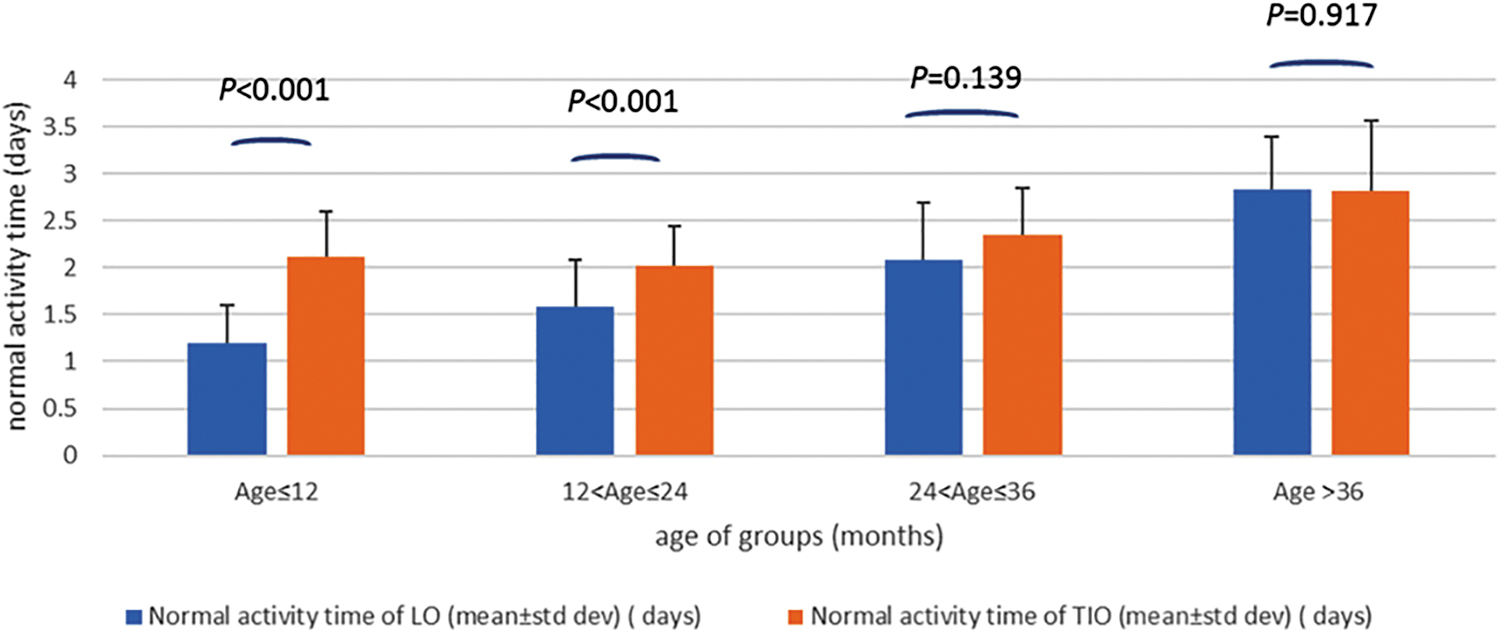
Comparison of postoperative normal activity time between LO and TIO. LO, laparoscopic orchiopexy; TIO, traditional inguinal incision orchiopexy.
Comparison of Postoperative Outcomes Between Laparoscopic Orchiopexy and Traditional Inguinal Incision Orchiopexy
Value indicates P value <.05, which was considered statistically significant.
Independent samples t-test (two-tailed) was performed (normality of data was checked before t-test [if not normal distribution, U-test was used]).
Chi-square test was performed (with cell[s] with n < 5 Fisher's exact test was performed).
LO, laparoscopic orchiopexy; SD, standard deviation; TIO, traditional inguinal incision orchiopexy.
Discussion
In recent years, LO has been mostly applied to the treatment of nonpalpable UDT and peeping testicles. The results show that laparoscopic surgery was more efficient and more sufficient in the aspect of testicular dissection than traditional surgery. To date, laparoscopic surgery had become a gold standard for nonpalpable UDT.3,8 However, the application of LO for palpable UDT was still controversial.
In 1995, Docimo et al. 9 first reported LO treatment of the palpable UDT and then Riquelme et al. summarized that LO is a safe procedure for patients with palpable UDT, and no more complications were found. Of the 192 patients, only one case was converted to TIO.7,10 However, recommendation for palpable UDT undergoing surgery is still disputable and the prescrotal techniques were based on the surgeon's preference and experience. 11
Bianchi first described the scrotal approach for management of cryptorchidism in 1989. 12 Evidence shows that the scrotal approach has success rates ranged from 88% to 100% for palpable UDT. 13 However, the general view is that more proximal testes tend to have a poorer outcome of operation due to inadequate exposure. 14
As far as we knew about the etiology of cryptorchidism, testicular descent from the abdominal cavity to scrotum occurs between 25 and 35 weeks of gestation. 15 Testicular descent into scrotum relies on a ligament called GT. Many uncertain reasons prevent the descent and remain the testicle in the abdomen or groin in cryptorchidism. 16 Meanwhile, the GT remained as ligament that leads the testicular could not extend into scrotum.
Surgery of orchiopexy need to cut off the dysplastic GT as the main procedure to make adequate mobilization of testicles. In LO for palpable UDT surgery, if the testicles can be pulled back into the abdominal cavity, the laparoscopic way is more conveniently to cut off the dysplastic GT compared with the traditional way. The subsequent mobilization of testicles would be sufficient and efficient. So, whether the testicles can be pulled back into the abdominal cavity is a key procedure.
According to relevant literature reports, the incidence of cryptorchidism associated with an inguinal hernia was 56%. 17 More than 92% of patients with unilateral palpable UDT had an ipsilateral open IIR at a median age of 14.9 months. 18 Our study found that 98.0% of children were aged <1 year, and had open IIR. 97.9% of the testicles could be pulled into the abdominal cavity easily to accomplish the LO procedure. From this study, we found that open IIR does not necessarily mean hernia. The open IIR generally exists in cryptorchidism. The proportion of open IIR decreased gradually with age. From 2008, guidelines recommended that surgery should be performed before the child's first birthday to minimize the risk of impaired fertility. 19 In this recommended age, almost all IIR is open, which is an advantageous term for laparoscopy.
Our study shows that palpable UDT associated with an ipsilateral open IIR confirmed during the laparoscopy was >90% (91.7) even within 2 years of age. It seemed that LO is not suitable for the majority of the elder children, especially those >2 years old. If closed IIR was available, it would be very hard to achieve LO surgery, since testicles might not be pulled back into the abdominal cavity in those patients. We tried to reopen the closed IIR, and then it was found that it was still hard to pull back the testicles and increased the risk of damage to vas deferens and spermatic vessels. So, we take a relatively conservative technique routine, we transferred to inguinal incisions when the IIR were closed. Forty-three out of 170 cases converted to open inguinal approach. Combined with an inguinal incision maybe necessary when LO procedure was hard to continue for these elder children; further study is needed for the challenge of inadequate length of spermatic cord of these elder children.
The peritoneal defect is closed after the testicle has been mobilized during LO. When no ligature or suture was contemplated, the operative time decreased significantly. Rafiei et al. 20 carried out a randomized controlled trial to evaluate the no ligation method for children. He concluded that herniotomy without sac ligation in children saved many times and also prevented many other possible complications such as nerve damage, spermatic cord injury. Riquelme's literature shows that there was no need for closure of the IIR during LO. 21 In their study of the staged treatment of LO, they found the peritoneum of the unsutured IIR in the first stage of the operation was completely closed during the second stage of the operation. Khairi et al. 22 carried out a prospective study to compare the difference between the IIR conventional suture group and IIR without closure group during LO. It was concluded that closure of the peritoneum over the IIR can be omitted in LO, saving operative time and effort, without risk of recurrent inguinal hernia.23,24
The main controversy of LO still focuses on abdominal interference and anesthesia with tracheal intubation, which may cause more risks to patients. No additional complications of LO were observed in our study. Further studies are needed in the future. Accompanied by the advance of technique, incisions of laparoscopic surgery are becoming smaller and smaller, which contributes to more cosmetic effects. In addition, LO imitates the natural descent procedure of testes more similarly.
Conclusions
LO is an appropriate choice for palpable UDT, especially in younger children aged <2 years. The success rate of LO decreased with age.
Footnotes
Acknowledgments
The authors gratefully acknowledge the trust and support given by staff of our pediatric surgery.
Ethics Approval and Consent to Participate
The research has been performed in accordance with the declaration of Helsinki. Our study was approved by the Ethics Committee of The First People's Hospital of Lianyungang (JSYY-20131228001).
Availability of Data and Materials
The data sets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Authors' Contributions
S.D.G. and H.L. design the study; S.D.G. and Y.-X.W. collected the data; S.D.G. wrote the article; Y.-X.W. and H.L. revised the article; all the authors read and approved the final article.
Disclaimer
The author confirms that the study described has not been published before, it is not under consideration for publication elsewhere,its publication has been approved by all coauthors, if any, and its publication has been approved (tacitly or explicitly) by the responsible authorities at the institution where the study is carried out. The author agrees to publish in the journal indicated hereunder and also in English by BMC Surgery Journal.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.