
Abstract
Background:
Posterolateral thoracotomy provides limited access to the thoracic apex that can result in poor visualization of subclavian vessels, their branches, and the brachial plexus. A thoracoscopic approach may overcome these limitations.
Purpose:
We report a thoracoscopic approach and associated technical challenges in resecting apical thoracic neuroblastoma encasing the subclavian artery.
Methods:
A single-institution retrospective chart review was performed (2018–2020) for patients undergoing thoracoscopic resection of apical neuroblastoma encasing the subclavian artery. Patient demographics, imaging, and hospital course were reviewed. Operative video recordings were assessed for exposure quality, technical challenges, and percentage of tumor resection. Patients were placed laterally, with three 5-mm ports triangulated to the apex. Dissection started at the tumor edge and followed along the vessel and branches.
Results:
Four patients (median age 2.7 years) underwent thoracoscopic apical neuroblastoma resection. Median length of stay was 2.5 days. One low-risk patient underwent resection for tumor growth during observation. One intermediate and 2 high-risk patients received neoadjuvant chemotherapy. Two patients continued having persistent vascular encasement, whereas in 1 patient the mass decreased in size and only abutted the subclavian and vertebral arteries. In 1 patient, tumor involved the brachial plexus, which was freed and preserved thoracoscopically. All cases had substantial tumor-feeding vessels branching from the subclavian artery. There was one conversion to open thoracotomy due to dense tumor adherence to the subclavian artery and vein. More than 95% resection was achieved in all cases. All patients had baseline Horner syndrome. No complications were reported.
Conclusion:
The thoracoscopic approach for resecting apical neuroblastoma provides optimal exposure and safe access in selected patients.
Introduction
Neuroblastoma is the most common extracranial pediatric solid tumor, and ∼25% of neuroblastomas are thoracic. Thoracotomy during childhood is associated with a high risk of scoliosis and chest wall deformities.1–3 Thoracoscopic resection of neuroblastoma is associated with a shorter length of stay and decreased blood loss, without a significant difference in complications or oncologic outcome; however, patients need to be carefully selected.3–16 Thoracoscopic resection of neuroblastoma without image-defined risk factors (IDRFs) has been demonstrated to be safe.3–16 However, the effect of IDRFs on the feasibility of thoracoscopic resection of apical neuroblastoma has not been studied.3,5 Posterior mediastinal and paravertebral exposure can be provided with standard posterolateral thoracotomy; however, this approach provides suboptimal access to the subclavian vessels and brachial plexus. The aim of this study was to examine the utility of the thoracoscopic approach for apical neuroblastoma encasing the subclavian vessels.
Methods
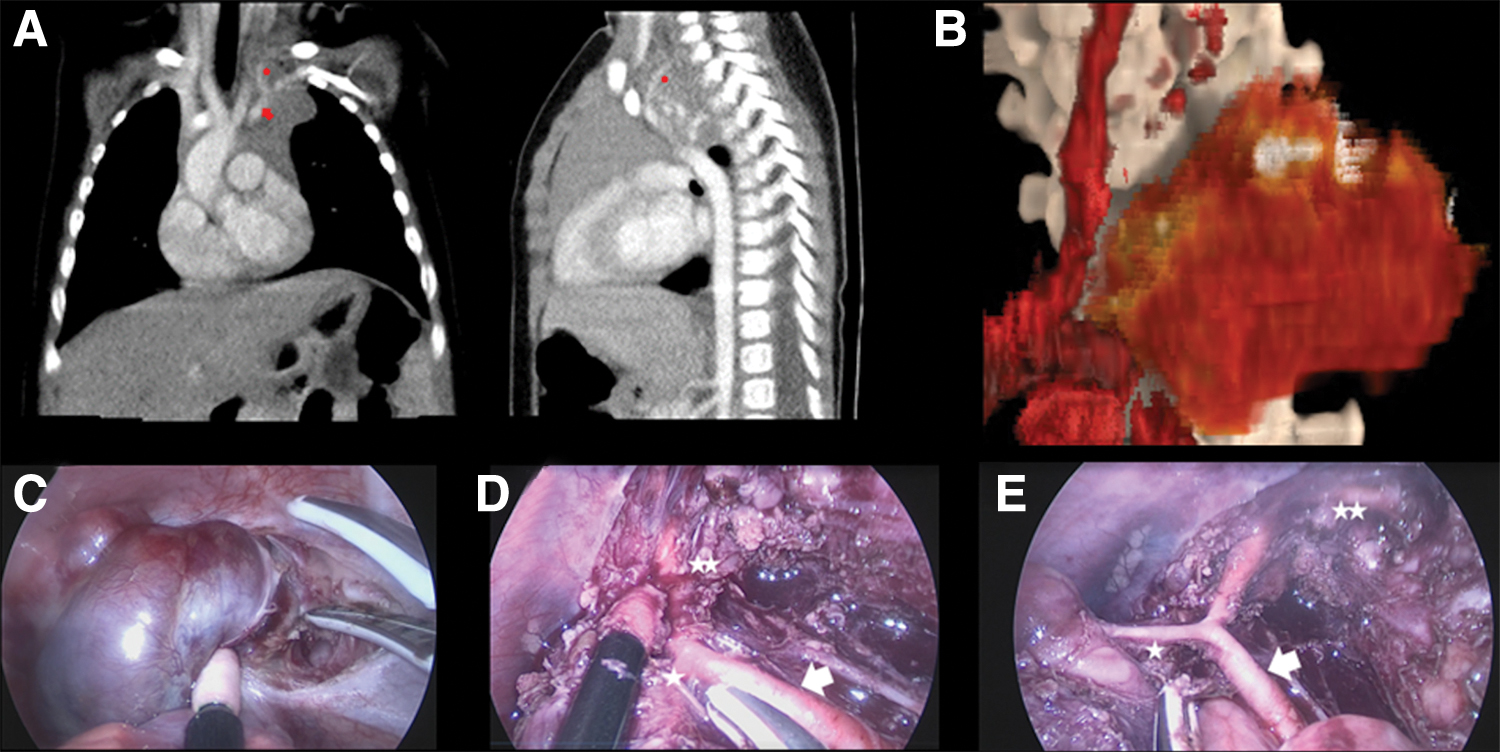
The local institutional review board approved this study and informed consent was waived. A single-institution retrospective chart review was performed from 2018 to 2020 for patients undergoing thoracoscopic resection of apical neuroblastoma encasing the subclavian artery. Patient demographics, imaging, and hospital course were reviewed. Patients were evaluated with dual-phase contrast computed tomography scan and magnetic resonance imaging to enhance the visualization of IDRF and degree of vessel encasement (Fig. 1A, B). Operative notes and video recordings were assessed for quality of exposure, technical challenges, and percentage of resection. The contralateral bronchus was intubated to establish single lung ventilation, and patients were placed in a lateral position with three 5-mm ports triangulated to the apex.
Patient 2, images and resection:
The pleura over the lateral corner of the tumor was incised with an energy device to expose the distal subclavian artery anterior wall and to establish a dissection plane for the remainder of the procedure (Fig. 1C). When the distal subclavian artery could be visualized, blunt dissection was performed using the LigaSure™ device (Maryland Jaw Thoracic Sealer/Divider with Nano-coating; Medtronic, Minneapolis, MN) on top and parallel to the anterior wall of the artery from distal to proximal. This technique allows for deliberate exposure of the subclavian artery and branches. The first branch to be encountered was usually an inferiorly located tumoral branch, and as dissection proceeds proximally, the origin of the vertebral artery can be seen superiorly (Fig. 1D, E). Once the subclavian artery and the proximal part of the vertebral artery are displayed, the tumor branch anatomy can be verified and controlled with a clip. The tumor can then be freed using an endoscopic Kittner or Ligasure, and all tumors were removed from the chest by using an endoscopic retrieval bag. No vascular injury or significant bleeding occurred; a clear operative field was maintained throughout dissection. When the brachial plexus was involved, a neurosurgeon participated in the operation to ensure accurate identification of anatomy. Critical steps of subclavian vessel dissection and resection of apical neuroblastoma are shown in the Supplementary Video S1.
Results
Four patients (3 boys and 1 girl) underwent thoracoscopic resection of apical neuroblastoma with IDRFs (Table 1). Median age of patients at the time of resection was 2.7 years (range: 6 months to 4 years). Median length of stay was 2.5 days. Median tumor volume was 36.5 mL (range: 12–115 mL). Median operative time was 225 minutes (range: 130–235 minutes) and median blood loss was 35 mL (range: 15–50 mL). One low-risk patient (patient 2) underwent resection due to 70% tumor growth during observation (Fig. 1). The other 3 patients received neoadjuvant chemotherapy (2 intermediate risk and 1 high risk). Three patients continued to have persistent vascular encasement, whereas in 1 patient (patient 4), the mass decreased in size and only abutted the subclavian and vertebral arteries. In 1 patient (patient 3), the tumor also involved the brachial plexus that was freed and preserved thoracoscopically (Fig. 2). A substantial tumor-feeding vessel branching from the subclavian artery was seen in all cases. The 1st patient in the series with intermediate risk (patient 1), who received neoadjuvant chemotherapy, required conversion to open thoracotomy due to dense tumor adherence to the subclavian artery and vein. Subclavian vein encasement was not seen in any of the 4 patients. More than 95% gross total resection was achieved in all cases. All 4 patients had preoperative Horner's syndrome that persisted postoperatively. No complications occurred.
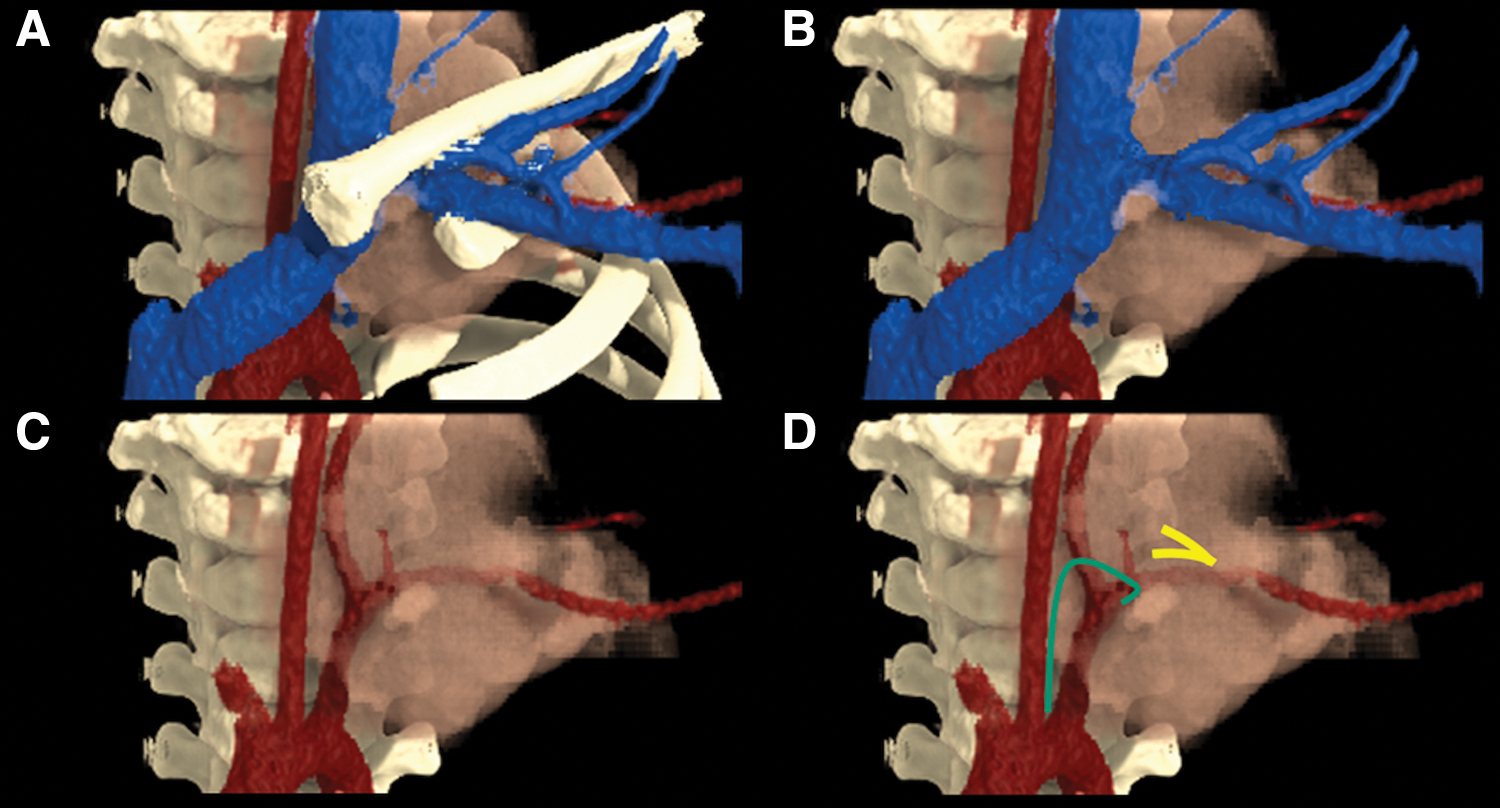
Patient 4, 3D image reconstruction showing apical neuroblastoma encasing the subclavian and vertebral arteries.
Characteristics of 4 Patients (3 Boys and 1 Girl) Undergoing Thoracoscopic Resection of Apical Neuroblastoma with Image-Defined Risk Factors
IDRFs, image-defined risk factors; NA, not available.
Discussion
This study shows that moderately sized apical neuroblastomas encasing the subclavian artery can be safely approached and resected thoracoscopically. The technique described herein allows safe and confident dissection of the subclavian artery, with identification of critical branches including the vertebral artery and tumor-supplying branch vessels that must be identified when conducting this operation. This approach can be safely attempted in patients who have received neoadjuvant chemotherapy; however, dense adhesions to the subclavian vessels or brachial plexus may prompt conversion to an open procedure in some cases. Although subclavian artery encasement represents an IDRF, our study shows that this does not preclude the use of a safe thoracoscopic approach. However, larger tumors with subclavian artery encasement or bulky cervicothoracic tumors are still best approached using the open surgical technique. 17 The primary limitation of posterolateral thoracotomy is suboptimal exposure of the thoracic inlet. This exposure can be slightly improved by transection of the costosternal junctions of the ribs above to maximize rib retraction. Optimal exposure of the subclavian vessels can be achieved by median sternotomy with supraclavicular extension 18 ; however, this “trap door” incision is associated with high morbidity. 19
Some specific anatomic considerations can help improve the success of this approach. First, the thoracoscopic technique allows safe dissection of the subclavian artery by maintaining dissection on top of its anterior wall in a parallel direction from distal to proximal. If this cannot be safely achieved during the operation, then conversion to an open procedure is recommended. Second, the critical relationship of the proximal subclavian artery and the major lymphatic channels should be considered to avoid inadvertent ductal injury and chylothorax. The thoracic duct descends anterior to the first part of the left subclavian artery before draining into the junction of the left internal jugular and subclavian veins (Fig. 2D). The left subclavian trunk courses superior to the subclavian artery, and the left bronchomediastinal trunk ascends posterior to the artery. Both trunks may either join the thoracic duct or drain separately into the venous system. A higher incidence of postoperative chylothorax was observed in patients with IDRF. 5
Three patients in this study received neoadjuvant chemotherapy before thoracoscopic resection was attempted. The decision to administer neoadjuvant chemotherapy is dictated by the tumor risk-stratification status, which incorporates a multitude of elements including patient age, tumor biology, and International Neuroblastoma Risk Group (INRG) stage. 20 Patients with high-risk or intermediate-risk disease usually receive neoadjuvant chemotherapy before surgical resection. Neoadjuvant chemotherapy can successfully resolve subclavian vascular encasement in up to 66% of patients, but should not be administered solely for this anatomic consideration. 21 Chemotherapy-induced changes may make the tumor more adherent to the vessel wall. No controlled studies have examined the relationship between tumor size and feasibility of thoracoscopic resection; however, tumor size has ranged from 3 to 5 cm in most studies using the thoracoscopic approach.1–16 The feasibility of a minimally invasive approach is influenced by working space, and, therefore, the ratio of tumor-to-hemithorax size may be most relevant when planning surgery.13,14
Because the microscopic tumor resection margin does not influence the prognosis for neuroblastoma, resection of tumors with IDRF can be facilitated by bisecting or dividing the tumor. In some circumstances, gross disease can be left behind without significant oncologic consequences to prevent vascular or nerve injury. The lower trunk of the brachial plexus is near the distal thoracic course of the subclavian artery (Fig. 2D), and care should be taken when the tumor extends to this region. In our study, for the patient who had brachial plexus involvement, we elected to leave ∼5% of the overall tumor volume in this area to minimize the chance of neurologic injury.
Although thoracoscopic resection offers satisfactory exposure with minimal incisions and low morbidity, patients <18 months old with moderately sized apical neuroblastomas could also be potentially managed by observation alone. This is an area of active investigation and could become standard practice in the future. Previous studies reported a high rate of spontaneous regression in infants with neuroblastoma and confirmed the safety of a nonoperative approach in this group.22–26 In the current Children's Oncology Group Trial ANBL1232: (“Utilizing response- and biology-based risk factors to guide therapy in patients with non-high-risk neuroblastoma”), eligibility criteria have been extended to include observation arms for infants <18 months old with IDRF and favorable histology and genomics. In this trial, infants <12 months of age at diagnosis and with tumors <5 cm were enrolled on a study arm and received observation alone for up to 96 weeks without tumor biopsy. Surgical resection was reserved only for patients who demonstrated disease progression during observation. Also, in ANBL1232, patients <18 months of age at diagnosis who have INRG stage L2 tumors (localized tumors with IDRF) undergo tumor biopsy. If the tumor demonstrates favorable biology and no unfavorable genomic features (segmental chromosomal copy number aberrations), patients may be followed by observation alone.
For resection of apical neuroblastoma, the thoracoscopic approach provides optimal exposure and safe access and should be performed by surgeons with both advanced minimally invasive skills and experience with neuroblastoma surgery.
Conclusion
The thoracoscopic approach for apical neuroblastoma provides optimal exposure and safe access for resection in selected patients with IDRF. The importance of understanding neuroblastoma biology and principles of resection, together with familiarity with endoscopic tumor anatomy, cannot be overemphasized. Thoracoscopic dissection of vessels encased with neuroblastic tumors requires specific competencies such as maintaining a bloodless field, readiness to appropriately change the approach to prevent injury, and the ability to rapidly correct injuries that may occasionally occur during thoracoscopic dissection.
Footnotes
Authors' Contributions
All authors took part in writing the article, reviewing it, and revising its intellectual and technical content. All authors assume responsibility and accountability for the results.
Acknowledgment
The authors thank Vani Shanker for editing the article.
Disclosure Statement
All authors declare no conflict of interest.
Funding Information
No funding was received. There has been no financial support for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.