
Abstract
Background:
We previously reported a 2% Clavien IIIb urologic-induced complication rate associated with blind (no guidewire, no fluoroscopy) prophylactic ureteral localization stent (PULSe) placement. As part of a quality improvement initiative, mandatory guidewire placement before PULSe was performed and urologic-induced Clavien IIIb or greater complication rates were evaluated. A systematic review was performed to elicit the overall urologic-induced complication rate in the literature.
Materials and Methods:
A retrospective review of all patients who underwent guidewire-assisted PULSe placement before colorectal surgery was performed. The contemporary cohort was compared with those in the prior cohort using age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, preoperative creatinine, postoperative creatinine, pre-/postoperative creatinine difference, and Clavien IIIb urologic-induced complication rates. A review of literature from 1982 to 2019 was performed using 14 unique search terms. Of 38 studies reviewed, 18 met predetermined inclusion criteria.
Results:
One hundred thirty-two patients underwent bilateral PULSe placement with mandatory guidewire utilization. Mean age and BMI were 55.78 (18–89) and 27.02, respectively, with zero Clavien IIIb complications, compared with a rate of 2% (P < .001) in our prior study. Our contemporary cohort yielded a more favorable postoperative creatinine (P < .022) and pre-/postoperative creatinine difference (P < .003). A review of literature identified a mean Clavien IIIb complication rate of 0.38%.
Conclusions:
Mandatory guidewire utilization before PULSe placement reduced the Clavien IIIb complication rate to zero, compared with a rate of 2% from our prior cohort. Guidewire utilization can decrease Clavien IIIb urologic-induced complication rates. A review of the literature shows a lack of uniformity concerning the technique of PULSe placement.
Introduction
Iatrogenic ureteral injury (IUI) can occur during abdominopelvic operations, with gynecologic and colorectal surgery (CRS) being the number one and two most common culprits, respectively. 1 In particular, reported rates of occurrence are between 0.24% and 7.6% during CRS.2–4 Unfortunately, trends show the rate of IUI increasing over time,5–7 with the majority being associated with bulky tumors, history of radiation or pelvic surgery, obesity, fistulas, or inflammatory processes such as diverticulitis and Crohn's disease.8–10 Utilization of prophylactic ureteral localization stent (PULSe) is theorized to aid in intraoperative ureteral localization and discovery of IUI.2,11–14
PULSe placement is not a benign procedure. We previously reported the incidence of urologic-induced Clavien grade IIIb or greater complications secondary to PULSe placement at 2%. 14 Complications may include transient, gross hematuria,14–16 postoperative urinary tract infection (UTI),10,11,13,14 hydronephrosis,11,14 and reflex anuria.14,17 More recently, a retrospective study demonstrated a nearly threefold increase in acute kidney injury incidence among CRS patients after PULSe placement. 1
Conclusions from our previous investigation raised the possibility of mandatory guidewire usage before PULSe placement, to limit these urologic-induced complications. 14 As a quality improvement initiative, we sought to compare rates of urologic-induced complications in patients with and without mandatory guidewire use before PULSe placement. We believe a further investigation into PULSe utilization and complication rates, with comparison to mean Clavien IIIb complication rates found in the literature is vital; therefore, a systematic review of the literature was conducted.
Materials and Methods
This protocol for this study was evaluated by the IRB of Wake Forest University School of Medicine and determined to be exempt. A retrospective review of all patients who had undergone PULSe placement at the time of CRS, between July 2015 and June 2016, was performed. A SensorTM PTFE-Nitinol Guidewire with Hydrophilic tip (Boston Scientific, Marlborough, MA) was required during the sterile placement of bilateral 5 French × 70-cm TigerTail (Bard Medical Division, Covington, GA) PULSe devices before CRS cases. This cohort was then compared with the prior cohort 14 from July 2013 to June 2014 by the following variables: age, American Society of Anesthesiologists (ASA) score, body mass index (BMI), Clavien III urologic-induced complication rate, general complication rate, pre- and postoperative serum creatinine, change in pre- and postoperative serum creatinine, fluoroscopy and guidewire utilization rates. The procedure codes and associated diagnoses for CRS cases among the two different years were reviewed and found to be similar.
The Dindo et al. 18 classification system was used for complication grading. Complication rates in patients receiving PULSe placement utilizing a guidewire before CRS were compared with patients in our prior cohort 14 that received PULSe placement without the use of a guidewire. More than 90% of cases were performed in a minimally invasive manner; indications for surgery were similar between the cohorts.
Evidence acquisition
Search criteria and article selection
A review of literature for articles published between 1985 and 2019 was conducted using the following terms: “prophylactic ureteral stent,” “localization stent,” “ureteral localization stent,” “prophylactic ureteral stent/localization stent/colorectal surgery,” “prophylactic ureteral stent/localization stent/colectomy,” “prophylactic ureteral stent/localization stent/general surgery,” “intraoperative ureteral injury/ureteral stent,” “intraoperative ureteral injury/ureteral stent/colorectal surgery,” “intraoperative ureteral injury/ureteral stent/colectomy,” “intraoperative ureteral injury/ureteral stent/general surgery,” “intraoperative ureteral injury,” utilizing PubMed, Embase, Scopus, and Web of Science databases. 19 The patient-intervention-comparison-outcome (PICO) criteria 20 was utilized in constructing our study structure.
A sum of 1946 records was reviewed. After screening for “Human-study,” “English language,” “full-text articles,” 994 results remained. Nine hundred ninety-four abstracts were reviewed. After applying predetermined inclusion/exclusion criteria and removing duplicates, 18 journal articles were included in our review. Our inclusion criteria were as follows: original journal article, PULSe placement performed before CRS, and articles targeting human subjects. Our exclusion criteria were as follows: systematic reviews or literature reviews, any publication that was not considered to be an “original journal article,” PULSe placement before gynecologic surgery, PULSe placement not performed before CRS procedures, articles written in languages other than English, and animal studies. Sources from systematic reviews were scoured and utilized in our analysis as indicated (Fig. 1).
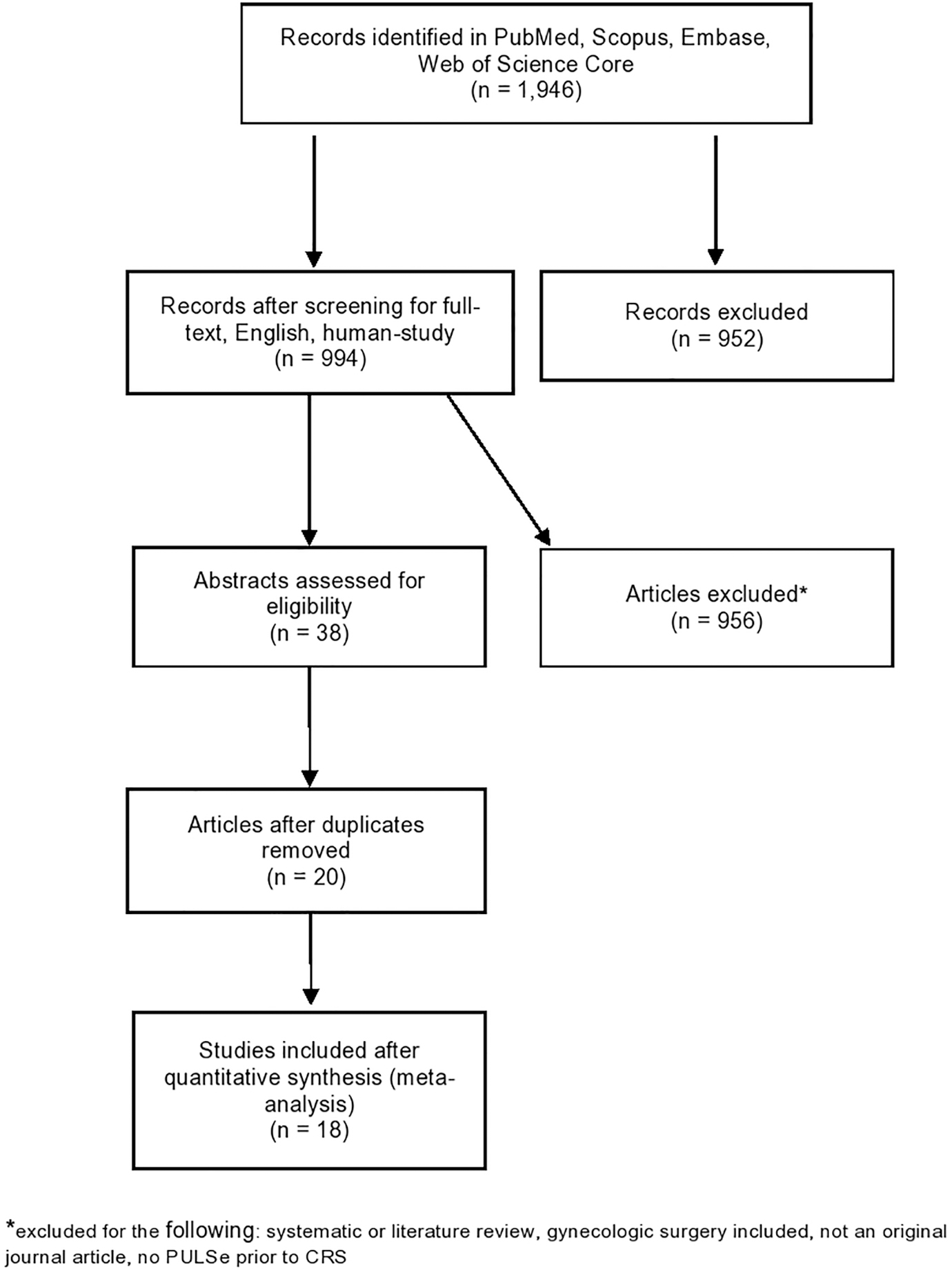
PRISMA flow diagram. 19
Results
One hundred thirty-two patients underwent bilateral PULSe placement with mandatory guidewire use. The mean age and BMI of the contemporary cohort were 55.78 (18–89) and 27.02, respectively. We report no Clavien grade IIIb or greater complications in the contemporary cohort, compared with a rate of 2% (P < .001) as reported in the last study. The contemporary cohort yielded a more favorable postoperative creatinine (P < .022) and pre-/postprocedural creatinine difference (P < .003). 14 A comparison of the contemporary versus the prior series can be seen in Table 1.
Data Comparison Between Prior and Contemporary Cohorts
n = number of ureters.
Statistically significant.
BMI, body mass index.
A review of literature and urologic-induced complication profile can be seen in Table 2. Of the 18 articles evaluated in the review of literature, a total of 3880 PULSe placements were performed. In addition, between the aforementioned studies, none utilized a guidewire during initial PULSe placement, 1/18 studies (5.55%) utilized fluoroscopy, and 7/18 (38.9%) reported postoperative complications after PULSe placement (Fig. 2). The overall rate of Clavien IIIb or greater urologic-induced complication rate in the literature is 0.38%.

Articles reporting fluoroscopy versus guidewire utilization.
Comparison of Our Contemporary Series with Literature Averages of Clavien IIIb Complications
Per renal moiety.
Some patients only received unilateral stenting.
CRS, colorectal surgery; NR, not reported; PULSe, prophylactic ureteral localization stent.
Discussion
IUI is associated with an array of complications, including acute renal failure, UTIs, and sepsis, resulting in prolonged hospitalization with associated increased costs from subsequent treatments.12,14 Although they are associated with a plethora of complications, these are uncommon, occurring at rates between 0.2% and 7.6%4,22 of all CRS. The majority of IUIs (>65%) are diagnosed postoperatively through retrograde urography or by CT scan with IV urography, 23 although evidence suggests that when diagnosed postoperatively, IUI are associated with more complicated repairs and require more procedures to correct the injury when compared with those detected intraoperatively. 24 Despite this, IUI is unequivocally associated with higher morbidity even when detected intraoperatively; therefore, safer techniques to reduce IUI incidence during CRS, especially laparoscopic procedures, are a logical next step.
PULSe devices have been widely recognized as critical in localization of the ureters as well as early recognition and possible prevention of IUI,2,8–10,13 although there may be economic and logistical concerns regarding their use, including added time, cost, and resources. The reported cost of PULSe utilization shows some variability in the literature. In 2017, usage of lighted ureteral stents in 465 laparoscopic CRS cases, reported no IUI, although at an added cost of $167.01 per stent. 13 Placement of unilateral ureteral catheters costs an average of ∼$398.50 (€360) per insertion. 11 Other studies have estimated the added cost associated with PULSe device placement to be much higher, between $1500.0012,15 and almost $3500.0025 after the operating room time, urologist fees, and actual stent costs were included. Authors who advocate for broad utilization of PULSe argue that the increased costs of ureteral stent placement before surgery would ultimately be less than those incurred from an IUI with delayed diagnosis. IUI requires additional procedures to repair the defect, adds additional days to the patient's hospitalization (thereby increasing the time to return-to-function), and requires additional medical care for the associated complications. Further research should be completed to determine the cost-effectiveness of standardized guidewire use in PULSe placement versus additional length of stay and hospital costs due to IUI in the absence of guidewire use.
Those who may oppose the use of PULSe argue that complications, both during stent placement and after surgery, outweigh their benefit. Hematuria is a frequently observed complication, noted in 98.4% of cases, often resolving in 3 days and typically requiring no intervention. 15 Other PULSe-associated complications include perforation, anuria, and oliguria.2,8,9,14–16 It is important to keep in mind that even routine ureteral stent placement has reported complications of stent migration, stent encrustation, and impaired renal function at rates of 6.1%, 14.5%, and 5.4%, respectively. 26 There is no reported difference in rates of septic complications between groups that had received ureteral stenting before CRS versus those who received no stent. 2 Furthermore, multivariate analysis was performed to determine complications after PULSe placement, revealing no association between PULSe placement and postoperative UTI (P < .17). 2
Guidewire use, at a minimum, is effective at reducing PULSe complications. Previously, a retrospective study from July 2013 to June 2014 was performed, reviewing patients who underwent PULSe placement before CRS procedures. A Clavien class IIIb complication rate of 2% (4/188 patients) 14 was reported. Conclusions from this study beckoned for additional measures to minimize PULSe placement-induced complications while simultaneously demonstrating PULSe benefit. After this study, an institutional policy was made for the obligatory utilization of guidewire before PULSe placement. One hundred thirty-two patients underwent bilateral PULSe placement with mandatory use of a guidewire and no Clavien IIIb or greater complications were encountered. Eighteen articles were examined for guidewire utilization in the setting of initial PULSe placement for rates of Clavien IIIb or greater complications. The overall rate of Clavien IIIb or greater complications in patients not receiving a guidewire before initial PULSe placement was 0.38%. When contrasted with the mean rate of Clavien IIIb or greater complications reported in the contemporary series, guidewire use neutralizes the risk of urologic-induced injury. 14 Furthermore, we demonstrated that postoperative creatinine and pre-/postprocedural creatinine differences also favored the contemporary cohort against the prior cohort 14 (P < .022 and P < .003, respectively).
Other methods have been evaluated for their potential to prevent IUI. indocyanine green (ICG) has been studied extensively as a noninvasive modality to identify the ureter intraoperatively. 27 Utilizing ICG comes with three significant drawbacks; first, ICG must be infused either through the placement of a percutaneous nephrostomy tube or by retrograde infusion through a catheter, as IV infusion will result in nonselective fluorescence of nonureteral tissues. 28 Second, continuous infusion of ICG is necessary for adequate fluorescence of the ureter throughout the CRS case, resulting in increased resource utilization and cost. Finally, by utilizing ICG as opposed to PULSe, the surgeon loses the availability of a preinjury bridge of a potential ureteral defect. The use of lighted stents also shows promise,13,25 with one study claiming ureteral identification in 83% of laparoscopic colectomy cases. 25 Unfortunately, these studies are limited by factors such as added cost 13 and thermal injury. 25
Some limitations of our study should be noted. Our evaluation focused on complications in the setting of CRS, thus these results may not be reflected in the setting of gynecologic surgery. Although the institution data arise from a single center, indication for PULSe placement was not uniform among the two cohorts. Bilateral stent placement was the preferred method by the colorectal surgeon on record and, hence, unilateral placement was not routinely performed. To our knowledge, this is the first study to display the result of guidewire use before PULSe placement in complex CRS cases. In addition, although we recognize that there can be many variables that influence the rates of Clavien IIIb complications such as underlying cancer diagnosis (primary colorectal cancer versus gynecologic cancer versus postchemotherapy/radiation recurrence), intraoperative ureterolysis, duration stents were left in postoperatively, and patient gender, we were unable to control for these factors. In addition, due to the nature of the literature review, we were not able to maintain uniformity between articles, including the operating surgeon and center at which the procedure was performed. Ideally, follow-up for this study would entail a randomized control trial to assess urologic-induced ureteral complication incidence in guidewire versus no guidewire use in PULSe placement, allowing for better control of patient-specific and operative variables; however, its use is primarily at the discretion of the colorectal surgeon thereby limiting the potential for this opportunity.
Conclusion
PULSe utilization has been shown to decrease rates of intraoperative ureteral injury but is associated with an increase in direct costs and complications itself. Clavien IIIb or greater complication rates associated with guidewire-assisted PULSe placement are below the literature reported an average of 0.38%. Benefits to guidewire use for PULSe placement were also observed in postoperative and pre-/postprocedural creatinine difference.
Footnotes
Authors' Contributions
R.R.A.W., G.T., C.E., and G.S. performed data collection or management, data analysis, and article writing/editing; R.A.P. was in charge of protocol/project development, data analysis, and article writing/editing.
Disclosure Statement
No competing financial interests exist.
Funding Statement
No funding was received for this article.