
Abstract
Background:
Incisional hernias are a common complication of abdominal surgery (10%–35%) and are notorious for recurrence. Laparoscopic incisional hernia repair (LIHR) was first performed in 1991 and is reported to have lower recurrence rates. Few studies to date have assessed quality of life (QoL) resulting from a repair. The purpose of this observational study was to present a 12-year experience performing LIHR, with a focus on the impact on QoL.
Methods:
All adult patients undergoing elective LIHR performed by a single surgeon, whether primary or recurrent, were included in the study. The data collection was performed prospectively between 2007 and 2019 to include demographic details, intraoperative findings and postoperative short- and longterm outcomes. We used the Carolinas Comfort Scale (CCS) to assess QoL following surgery.
Results:
Ninety-seven patients were included in the study. Patients had a median age of 57 years, body mass index of 32 kg/m2, 35% were male and 88% were American Society of Anesthesiologists (ASA) class I or II. The duration of surgery was 90 minutes*. Nineteen percent of patients had complications during or after surgery; 1 (1%) had recurrence. length of stay in hospital was 1* (0–12) days and long-term follow-up period was 42* (2–140) months after surgery. Time of return to daily activities was 14* (1–365) days. Eighty-six percent of patients rated their experience undergoing LIHR as “Excellent” or “Good”. Regarding QoL after surgery, scores on the CCS indicated that 82% of patients had minimal or no discomfort following surgery, and only 1% had significant discomfort. *Presented as median.
Conclusions:
The technique for LIHR displayed in this study is safe and effective. There was an acceptable rate of complications, with a low recurrence rate. Patients were highly satisfied and had a good QoL after the procedure. Research Registry ID Number: researchregistry6056.
Introduction
Incisional hernias are a common complication of abdominal surgery, with an incidence of 10%–35%.1–3 Historically, incisional hernias have been notorious for recurrence following repair, particularly with open nonmesh repairs.4,5
Le Blanc and Booth reported the first experience with laparoscopic incisional hernia repair (LIHR) in 1993, developed primarily with the aim of reducing the rate of recurrences. 6 Two systematic reviews and meta-analyses so far have pooled the results of studies comparing open to LIHR.7,8 Despite considerable heterogeneity and need for further studies, they conclude that the laparoscopic approach offers lower rates of recurrence, shorter length of stay (LOS) in hospital, and lower rates of wound-related complications.
There is considerable variability in several aspects of LIHR, which may impact on the outcomes of the procedure. These include the numerous variations in the technique used by different surgeons, the large diversity of biomaterials available even within institutions, and the variety of fixation materials from which to choose. 9 It is generally accepted that application of a standardized technique for any surgical procedure offers a greater chance of positive outcomes.
Furthermore, few studies to date have addressed the impact of LIHR on quality of life (QoL), which overall is the primary objective of any surgical procedure. This is one of the main focuses of this study, applying the Carolinas Comfort Scale (CCS), which is a well-validated assessment tool of QoL in patients undergoing a hernia repair. 10
The primary aim of this study was to assess the impact of LIHR on patient satisfaction and the impact on QoL. Secondary aims included describing the standardized technique used throughout a 12-year experience of a single surgeon at a large district general hospital, the intraoperative details and other postoperative surgical outcomes such as LOS in hospital, complications, and functional recovery, including return to work and normal daily activities.
Methods
Patient selection
Adult patients who underwent a primary or repeated elective LIHR between 2007 and 2019 were included in this study. Hence, any patient undergoing repairs of primary ventral hernias, open repairs, emergency procedures and hernia repairs performed as a part of any other procedure were excluded.
The surgical technique
As standardized technique is followed for all patients. Following anesthetic induction, the patient is kept in the supine position and antisepsis and aseptic draping are completed, as well as the administration of prophylactic antibiotics. The position of the laparoscopic camera varies according to the hernia site. The port position is also chosen based on appropriate triangulation, depending on the location of the hernia. The majority of the hernias belong to the midline. Hence, the procedure is described based on this.
The surgeon starts the procedure standing on the left of the patient and creating a pneumoperitoneum with a Veress needle and insufflating to 12 mmHg. A 10 mm optical trocar is introduced in the left upper quadrant, followed by the instrument ports. Three ports are sufficient for hernia defects with a transverse diameter equal to or less than 8 cm. For hernias greater than 8 cm, two further ports (10 and 5 mm) are required for safer, more controlled handling of the hernia and of the mesh.
Most patients require adhesiolysis. Sharp dissection is preferred, but in some cases where dense adhesions involving bowel are encountered, a laparoscopic bipolar energy device is used. a The falciform ligament requires dissection for upper abdominal hernias. A peritoneal flap is routinely mobilized for lower abdominal hernias to access the preperitoneal space and expose the symphysis pubis for mesh fixation, as well as to allow free bladder expansion after the hernia repair.
The hernial contents are reduced and bowel inspected for any iatrogenic injury (Fig. 1). At this point, the intra-abdominal pressure is reduced to 10 mmHg for internal measurements of the hernial defect. The edges of the defect are project to the skin using 18-gaugle needles and an outline of the defect drawn on the skin. The required area of mesh is also drawn on the abdominal wall, extending 5 cm beyond the hernia defect in its whole circumference.

The hernial contents are freed from the hernial sac and reduced. Color images are available online.
At each of the four poles (cephalic, caudal, left, and right) of the defect outline, different shapes (triangle, circle, cross, and square) are drawn (Fig. 2). These are then also drawn on the composite mesh b c with the same orientation, the mesh is sized adequately and 2-0 polypropylene sutures are placed at each of the poles d (Fig. 3).

Dimensions of the hernial defect projected onto the abdominal wall as well as an outline of the mesh area required and shapes drawn to denote the orientation of the mesh. Color images are available online.
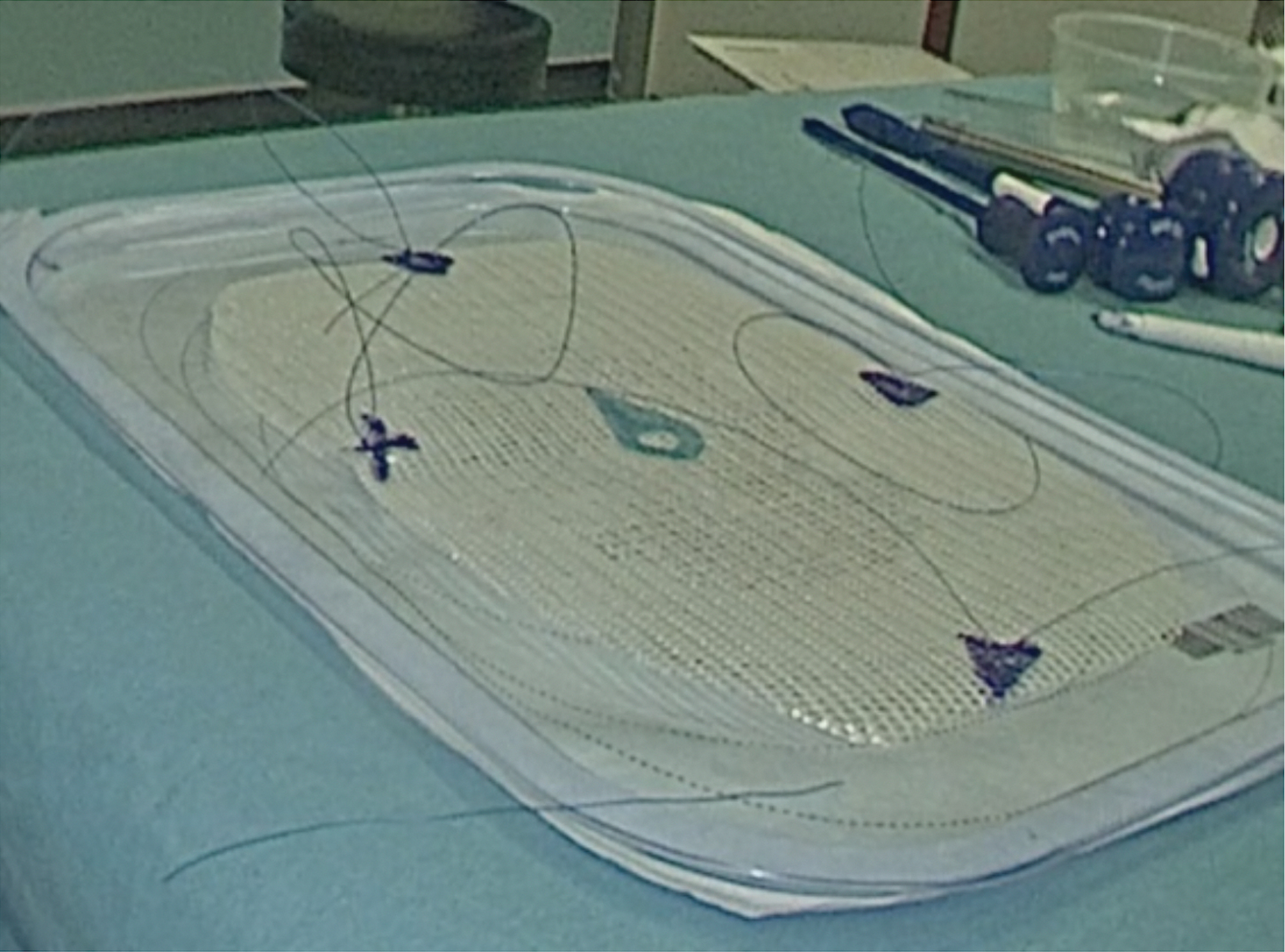
The same shapes as those on the skin are reproduced on the composite mesh to ensure its correct orientation. The mesh is sized adequately and 2-0 polypropylene sutures are passed through each of the drawn shapes. Color images are available online.
The intraperitoneal pressure is reduced to 6–8 mmHg. The edges of the hernial defect are approximated using trans-fascial 1 Nylon extracorporeal sutures e , which are introduced through stab incisions using an endoscopic suturing device. f These are passed 1 cm from the hernial defect edge and at 2–2.5 cm intervals (Fig. 4). This does not apply to hernia repairs related to Pfannenstiel incisions, where the defect closure is not feasible.
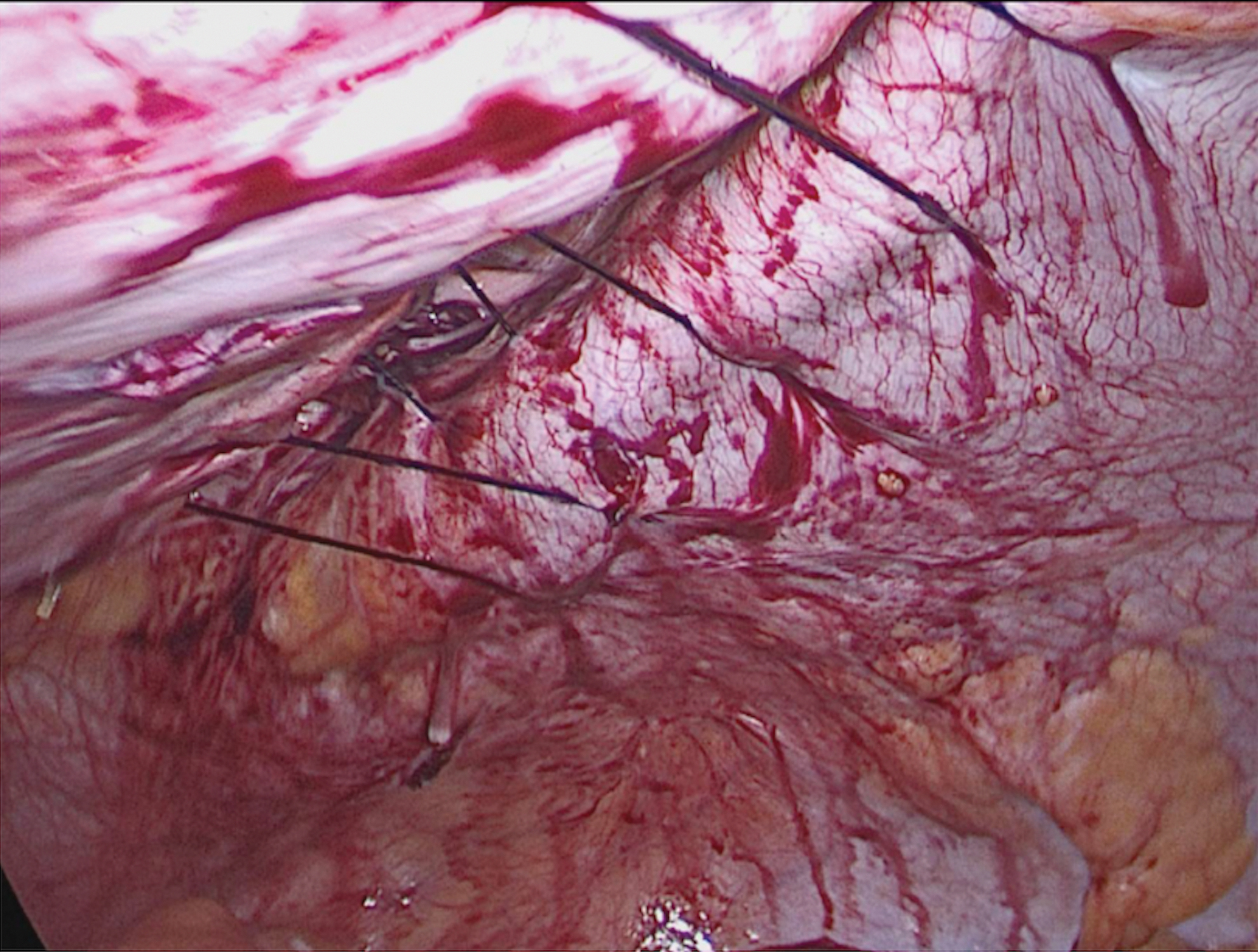
The hernial defect is closed using transfascial 1 Nylon extracorporeal sutures passed 1 cm from the defect edge and at 2 cm intervals. Color images are available online.
The abdominal pressure is then restored to 10–12 mmHg and the mesh is rolled up and introduced into the abdomen through a 10 mm instrument port. The drawings on the mesh are matched with those on the skin for correct orientation. The 2-0 polypropylene sutures on the mesh are transfascially fixed to the abdominal wall with the use of the endoscopic suturing device. Further mesh fixation is performed by applying titanium tacks g at 1 to 1.5 cm intervals applying the “Double Crown” technique (Fig. 5). For lower abdominal, this includes fixation of the mesh to the pubic symphysis, and the free peritoneal flap that had been created is fixed back to the abdominal wall, therefore overlapping part of the mesh.
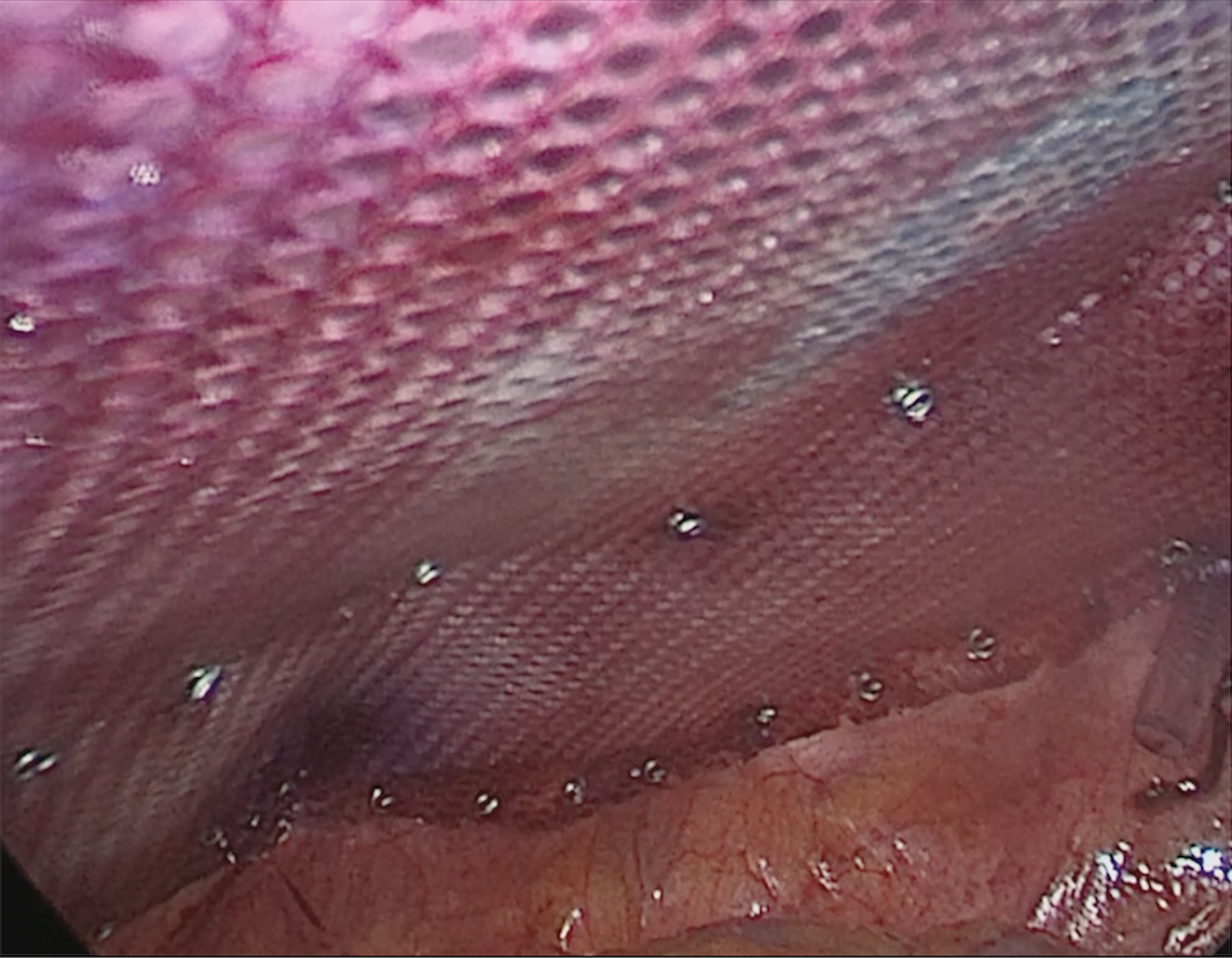
After the 2-0 polypropylene sutures on the mesh are transfascially fixed to the abdominal, fixation is completed with titanium tacks at 1 to 1.5 cm intervals applying the “Double Crown” technique. Color images are available online.
Standard postoperative care included low-molecular-weight heparin injections for thromboprophylaxis and analgesia starting with patient-controlled analgesia administered via an infusion pump, which is then downgraded gradually until oral analgesia is tolerated. Similarly, patients are started on clear fluids and gradually progressed to a normal diet. Patients are discharged once mobilizing freely, tolerating diet, and pain is adequately controlled.
Patients are routinely reviewed in clinic 8 weeks after the operation. Further outpatient reviews are arranged as needed, and follow-up telephone calls are conducted yearly.
Data collection
The dataset was collected prospectively between 2007 and 2019. Patient details recorded preoperatively included age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status class, hernia site, and whether the patient presented with a primary or recurrent incisional hernia.
Intraoperatively, data were collected on the number of defects found in the abdominal wall, the total defect size, the size of the mesh used, intraoperative complications, duration of the operation, and the successfulness of performing the procedure laparoscopically.
In the postoperative phase, the compliance of patients with a follow-up appointment at 8 weeks from time of surgery, as well as early complications, was recorded. Similarly, the total duration of follow-up was documented. During this time, data were collected on recurrence, return to normal activities (normal day-to-day, driving, work), overall patient satisfaction, and for the parameters required to complete the CCS.
Data presentation and analysis
Quantitative data are presented in tables and graphs along with medians or means, depending on whether normally distributed or not, as determined by the Shapiro–Wilk test. Percentages and ranges were also presented where appropriate. No comparative analysis was undertaken, given the observational nature of the study. Microsoft® Excel was used for statistical calculations and creation of graphs where needed. This manuscript was prepared following the Strengthening the Reporting of Cohort Studies in Surgery (STROCCS) guideline. 11
Ethics
This study was registered with the East Kent Hospitals University NHS Foundation Trust Research & Innovation Department, for which the registration number is 2020/GAP/22, and added to Research Registry ID Number: researchregistry6056.
Consent was obtained from all patients, at time of consultation before surgery, for their data to be stored for future research purposes. Patients' personal data were kept confidential on a password-protected file, which was stored on a nonnetwork share drive belonging to the Trust's network, which in turn has its own protection measures.
Results
Preoperative patient factors and clinical presentation of incisional hernias
Ninety-seven patients underwent a LIHR between 2007 and 2019 at this large District General Hospital in South East England. Most patients were female and obese (BMI >30) and the median age was 57 years. Similarly, most patients were ASA Grade of I (38%) or II (50%) (Table 1).
Patient Factors
Presented as median.
ASA, American Society of Anesthesiologists.
Nineteen (20%) patients had incisional hernias that were recurrent. Thirty (31%) belonged to lower midline incisions (including pfannenstiel incisions), 20 (21%) to paraumbilical incisions, 18 (19%) to full midline incisions, 14 (14%) to upper midline incisions, and 10 (10%) belong to right lower quadrant incisions (Fig. 6). Right paramedian and right upper quadrant were the least common locations for incisional with an incidence of 3 (3%) and 2 (2%), respectively.

Location of incisional hernias encountered. Color images are available online.
Operative findings and procedure
The median duration of surgery was 90 minutes (range 40–240) (Table 2). Ninety-six percent of incisional hernias were successfully repaired laparoscopically. The maximum craniocaudal and transverse defect was 20 and 12 cm, respectively. This does not include 3 patients with incisional hernias related to gynecological procedures through Pfannenstiel incisions who had defects measuring 13, 16, and 20 cm transversely. This is important given the difference in the technique applied to repair these hernias, as described above.
Operative Findings
Presented as median.
LIHR, laparoscopic incisional hernia repair.
Postoperative recovery and follow-up
The median LOS in hospital following LIHR was 1 day, ranging from 0 to 12 days (Table 3). One patient had the operation as a Day Surgery case. The longest stay was 12 days, in a patient who developed a small bowel obstruction postoperatively.
Follow-up and Return to Normal Activities
Eighteen (19%) of the 97 patients included in the analysis had a complication from the surgery (Fig. 7).

Complications following LIHR. LIHR, laparoscopic incisional hernia repair. Color images are available online.
Intraoperative complications included 2 (2%) iatrogenic bowel injuries. One was repaired primarily and one required bowel resection with a primary anastomosis. There was 1 (1%) patient who aspirated during surgery, leading to a collapsed lung and required admission to the Intensive Therapy Unit (ITU) for their immediate postoperative care.
Postoperatively and at 8-week follow-up, 9 (9%) patients had a seroma, 2 (2%) of which required radiological drainage. Three (4%) had a hematoma with 1 (1%) requiring a laparoscopic washout. One (1%) patient developed a small bowel obstruction, on a background of Crohn's disease with multiple prior open hernia repairs. He required a laparotomy, during which the mesh was removed. He was discharged from hospital 12 days after the initial operation.
The median follow-up period for patients was 42 months, ranging from 2 to 140 months. The time to return to normal activities had a median of 14 days (Table 3).
Twenty-four (25%) patients were not contactable or expressly declined to their data being used. Four patients died during follow-up of causes unrelated to the surgery. These patients were therefore excluded for the analysis related to the QoL and patient satisfaction.
Eighty-six percent of patients rated their experience undergoing LIHR as “Excellent” or “Good,” 8% as “Fair,” and 6% as “Poor” or “Very Poor” Table 4. Six (8%) patients were troubled by pain after surgery. Two (5%) reattended the hospital with severe acute pain but recovered subsequently, while 4 (6%) developed chronic pain.
Patient Satisfaction Feedback
Mean scores for sensation of mesh, pain, and movement limitation for each of the routine activities or movements included in the CCS are presented in Figure 8.
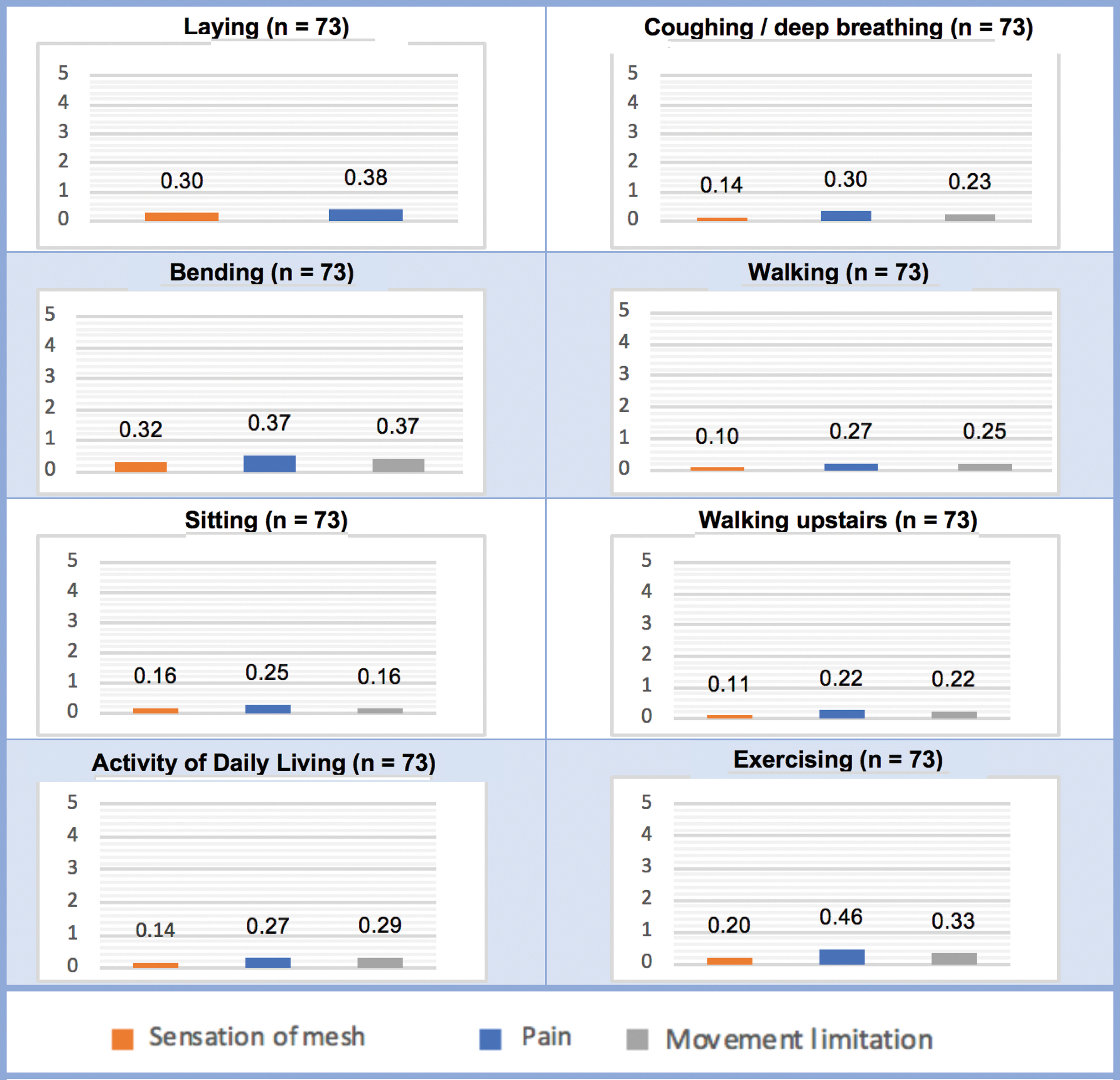
Carolinas Comfort Scale scores. Color images are available online.
All mean scores were <1, indicating no or minimal discomfort, as a result of the LIHR, during day-to-day activities or movements. This was consistent with the fact that 60 (82%) had a total CCS score between 0 and 10. Twelve (16%) patients had a total CCS scores between 11 and 60, indicating moderate discomfort and 1 (1%) patient had a total CCS score higher than 90, indicating debilitating discomfort (Fig. 9).
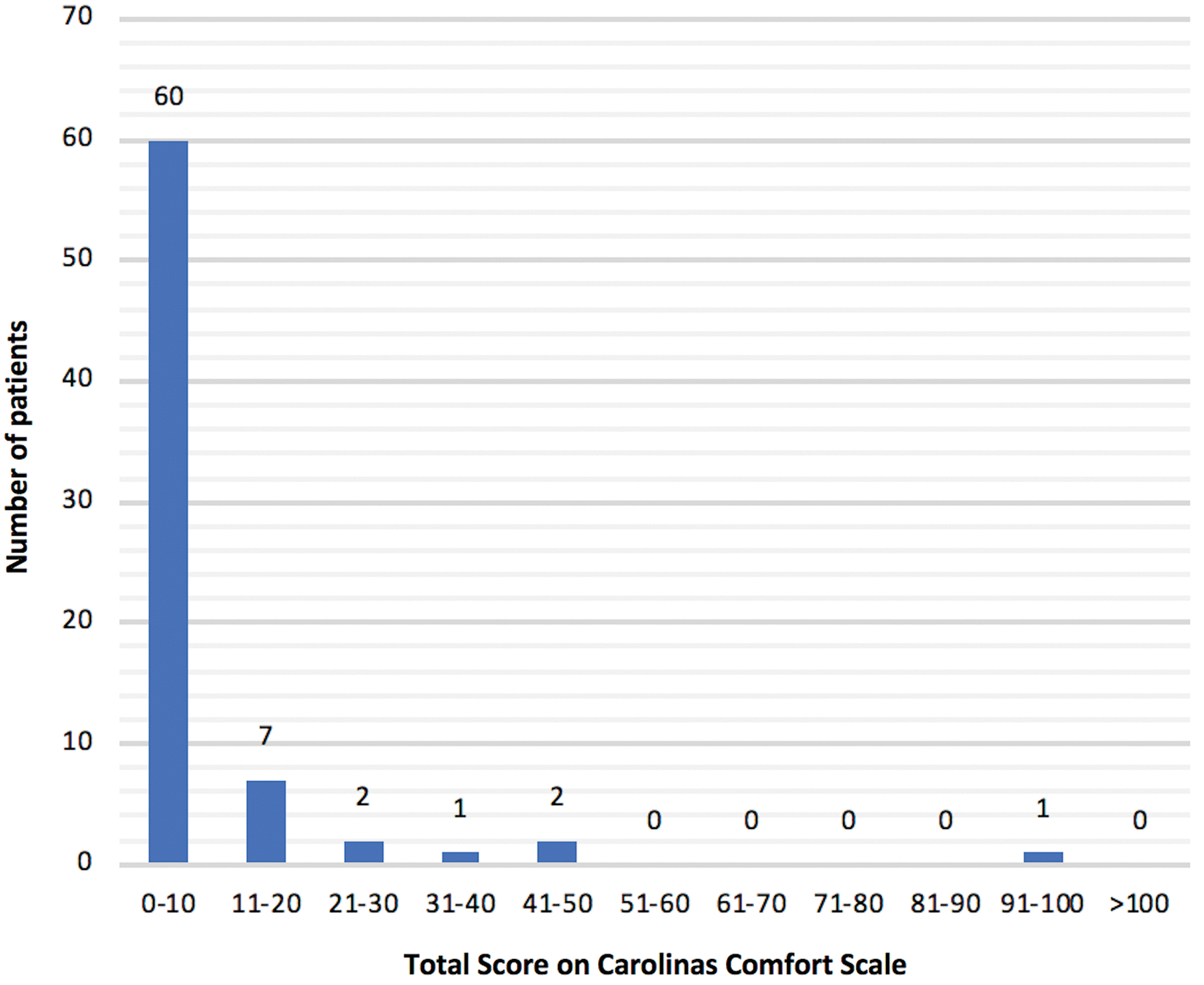
Total scores on the Carolinas Comfort Scale. Color images are available online.
There was moderate correlation between feedback for patient satisfaction and the total CCS score for each patient, with a correlation coefficient of 0.47.
Discussion
This was a retrospective review of a prospectively recorded data set, which provides an in-depth analysis of a 12-year experience performing laparoscopic repair of incisional hernias.
Preoperative patient demographics and characteristics
The demographics of patients in this study were similar to those in other series with a median age of 57 versus 46–64, a gender distribution where 35% were male versus 36.8–51.1, and a median BMI of 32 versus 29–32.12–15 Patients' preoperative ASA grades were also similar.16–19
Twenty percent of patients had recurrent incisional hernias, which again was consistent with prior studies, where the proportion of patients presenting with a recurrent incisional hernia ranged between 1% and 24%12,15,17,20
Intraoperative findings
The area of hernial defect found during surgery was significantly larger in this study (56 versus 26.2–33.1 cm2).15,21,22 Despite this, the median duration of surgery of LIHR in this study was 90 minutes and, therefore, similar to operative time previously reported (81–157.9 minutes).12,15,17,20,22
In this study, conversion rate to open surgery was 4% (4 patients). In 2 patients, this was because of dense adhesions; one in the context of Crohn's disease, and one following multiple previous hernia repairs. In other 2 patients, conversion to open procedure followed iatrogenic bowel injury. In previous studies, rate of conversion ranged from 0% to 13.7%.12,13,15–17,23
Complications
Overall, complications occurred in 19% of patients, which would seem high. However, in a meta-analysis by Awaiz et al. the pooled overall rate of complications was 38.9%. 8 Also, in the largest observational study to date on LIHR by Sharma et al., which included 1242 patients, an overall complication rate of 66% was reported. 15 No doubt there is a degree of heterogeneity between studies, particularly in terms of what was being considered as a complication of the surgery. The rate of complications leading to an intervention (6% versus 1.6%–8.3%) was consistent with prior experiences.12,16,21
Rates of wound hematoma or seroma (12% versus 15.3%) and bowel injury (2% versus 5.9%) were lower in this study compared to the pooled results presented by Awaiz et al. The rate of wound infections (1% versus 5.9%) was also lower in this study. Other than strict adherence to principals of surgical asepsis, no specific factors seem to account for this.
Six percent of patients complained of chronic pain in this study with a median postoperative follow-up of 42 months. Few other studies reported on chronic pain, all of which were observational. In these, the rate of chronic pain following LIHR ranged between 5.9% and 10%.13,15,21
It is important to note that 25% of the patients in this study were lost to follow-up, expressly declined being included, or died in the months following surgery. It is difficult to predict whether this may have had an impact on patient satisfaction and the CCS; those lost to follow-up may have been content and hence opted not to attend their appointments, while those who went back on their consent may have been less satisfied with the outcome of surgery.
Postoperative recovery and follow-up
In the meta-analysis by Awaiz et al., the mean LOS in hospital ranged between 2 and 5.7 days following LIHR. In observational studies, mean LOS similarly ranged between 1.9 and 6 days.12,15,21 In this study, the median LOS was 1 day. Of the 97 patients in this study, 73 received follow-up for a median period of 42 months. Of the 24 patients (25%) who were excluded from the data collection in the postoperative period for patient satisfaction and CCS, 18 were lost to follow-up, 2 declined the use of their data during follow-up, and 4 died in the months following surgery from causes unrelated to the operation. In other studies, the average follow-up period ranged between 34.2 and 90.2 months.12,13,15,17
Recurrence of incisional hernia occurred in 1 (1%) patient in this study. The pooled results reported by Awaiz et al. show a recurrence rate of 8.7% in a total population of 366 patients. This lower rate of recurrence reflects the importance of adhering to a single, standardized technique for LIHR, as well as the culmination of the learning curve for this procedure. These may be difficult to achieve universally, depending on how specialized centers performing LIHR are, as well as the volume of training being carried out at these centers. However, this study reflects a long-term experience in a district general teaching hospital, with a moderate volume of incisional hernia repairs being performed. This would seem to appropriately fit the description of most centers in the United Kingdom.
Patient satisfaction and QoL
Eighty-six percent of patients in this study rated their experience undergoing LIHR as either “Excellent” or “Good.” There are few other studies reporting on patient satisfaction and are highly heterogenous. The randomized clinical trial by Rogmark et al. provided the most comparable results, with 92% of patients reporting being “definitely satisfied” or “satisfied.” 24
In relationship to the return to day-to-day activities, there are few previous studies. Olmi et al. included 85 patients undergoing LIHR, in which the median time to return to work was 13 days, which was significantly lower than in this study (28 days). 25 It is important to consider that in this study, most patients had a higher BMI (32 versus 28), and a larger proportion were being operated for a recurrent incisional hernia (20% versus 5%), which could explain a more prolonged postoperative recovery time. Itani et al. also presented better outcomes for time to return to normal daily activities (14 versus 8 days) and return work (28 versus 23 days). 23 However, their study included all ventral hernias, not just incisional hernias, for which recovery time would be expected to be lower.
The main long-term objective of an incisional hernia repair is to improve patients' QoL. In this study, QoL was assessed using the Carolinas Comfort Scale, which is well-validated for several types of hernias, including ventral hernias. The fact that 82% of patients had a total CCS score ≤10 and that mean scores for sensation of mesh, pain, and movement limitation for each routine activity were <1, strongly suggest a high QoL in patients following LIHR. However, interpretation here is limited by the fact that preoperative scores were not recorded for comparison, hence it is difficult to attribute the results specifically to the hernia repair. On the contrary, the fact that there is moderate correlation between patient satisfaction and CCS scores in these patients would suggest that those scoring low on the CCS are more satisfied directly as a result of LIHR.
We could not identify any other studies that had used the CCS to assess QoL following LIHR. Saijo et al. and Rogmark et al. used the 36-item Short Form Health Survey (SF-36). Both showed an overall significant improvement of QoL as a result of LIHR. However, the SF-36 has not been specifically validated for LIHR. 26 Although the CCS has not been validated specifically for LIHR, either its well-validated application to ventral hernias or its focus on the use of a mesh makes it seem acceptable to extrapolate its validity to LIHR. Furthermore, it is unclear, given the nature of the CCS questionnaire, how it could be utilized preoperatively.
Study limitations
This study does, however, have a few limitations. As an observational study, it has limited value by itself for comparison with other techniques for incisional hernia repairs. The 97 patients included in this study reflect a moderate-sized case load (∼8 per year) for LIHR, considering the fact that they were all performed by a single surgeon at a district general hospital. Several of the later patients are yet to undergo further follow-up, during which incidence of complications, patient satisfaction, and QoL may still vary. With regard to the assessment of QoL, we are confident that the validity of CCS holds for LIHR. it is unfortunate that the CCS was not determined before surgery as well, as this would have allowed us to objectively attribute causality to the operation for any change in QoL after LIHR. However, patients are likely to have unconsciously made this comparison while answering the questionnaire.
Overall, the long-term results of this observational study indicate that the technique described for LIHR is safe and effective, with an acceptable rate of complications and low recurrence rate. Furthermore, this cohort of patients was generally highly satisfied and had a good QoL as a result of the procedure. The author would therefore suggest that LIHR be opted where possible. Furthermore, larger studies with an experimental design would be required to further establish the impact of LIHR on QoL and appropriately validate the use of the CCS for this cohort of patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.