
Abstract
Background:
Cholecystectomy trends and outcomes have been reported extensively in the private sector. Despite being one of the most common procedures performed in the United States, there is a paucity of reports on the trends and outcomes of laparoscopic and open cholecystectomy in the veteran population.
Materials and Methods:
Veterans who underwent laparoscopic or open cholecystectomy from 2006 to 2017 were identified using current procedural terminology codes from the Veterans Affairs Surgical Quality Improvement Program (VASQIP) database. Multivariable analyses were used to compare laparoscopic and open outcomes. The primary outcome was mortality, and secondary outcomes were postoperative complications and length of stay (LOS).
Results:
In the VASQIP database, 53,901 patients underwent laparoscopic cholecystectomy and 8011 patients underwent open cholecystectomy during the study period. The laparoscopic approach increased from 82.0% (2006–2008) to 91.9% (2015–2017). Postoperatively, the open group had a significantly higher morbidity rate (15.4% versus 3.8%, P < .001). The 30-day mortality rate and mean LOS were also significantly higher in the open cholecystectomy group (P < .001). Earlier year of operation, diabetes diagnosis, and open approach significantly increased the likelihood of postoperative morbidity (P < .05).
Conclusions:
Similar to the private sector, minimally invasive cholecystectomy in the Veterans Health Administration (VHA) has increased over the last two decades. Diabetes was present in a significant percentage of the veteran population and was a predictor of all postoperative complications. Finally, the clinical outcomes in the VHA are comparable with those documented in the private sector.
Introduction
Cholecystectomy is one of the most common procedures in the United States, with ∼1.2 million cases per year and an estimated 92% of these cases are performed laparoscopically. 1 Before 1992, most cholecystectomies were performed using the open approach, but laparoscopy is now the standard of care. With increased training and experience, the rates of postoperative morbidity and mortality following a laparoscopic cholecystectomy have declined gradually. Although bile duct injuries (BDIs) still occur more commonly following a laparoscopic approach versus an open approach, the rate of major BDIs has declined over time.2,3
The outcomes of laparoscopic and open cholecystectomies in Veterans Health Administration (VHA) facilities were reported in 1998 and 2010.4,5 These studies suggest that laparoscopic intervention leads to an approximate four times reduction in morbidity and six times reduction in mortality. The objective of this study was to ascertain updated data within the VHA system for cholecystectomies using an array of morbidity and mortality metrics. This study also explores the impact of certain comorbid factors, such as diabetes, on cholecystectomy outcomes using data from the Veterans Affairs Surgical Quality Improvement Program (VASQIP) database.
Methods
Veterans who underwent laparoscopic or open cholecystectomy from 2006 to 2017 were identified using current procedural terminology (CPT) codes within the VASQIP database. CPT codes for inclusion were 47562, 47600, 47605, and 47563. Information on laparoscopic-to-open conversions was unavailable, thus open cholecystectomies include potentially converted operations. The Institutional Review Board at the Washington DC Veterans Affairs Medical Center approved this retrospective study.
Patient demographic data included year of operation, age at time of operation, sex, race/ethnicity, alcohol and tobacco use, body–mass index (BMI), and preoperative risk factors. Data regarding operational outcomes were also collected and included infectious and noninfectious complications, wound complications, length of stay (LOS), and mortality at 30, 90, and 180 days postoperatively.
Statistical analyses
A retrospective cohort study examined the association between laparoscopic cholecystectomy outcomes, compared with open approaches, which were stratified by time period. Patients were grouped according to whether they underwent a laparoscopic or open procedure and the operative time period (2006–2008, 2009–2011, 2012–2014, and 2015–2017).
Each VHA site is categorized within a Veterans Integrated Service Network and an associated geographic area. 6 These geographic locations were divided into four broad locales: Northeast, Midwest, South, and West.
Pearson's chi-square analysis, analysis of variance, t-tests, and Fisher's exact tests examined the relationship between several factors, including demographic information and groups of interest. Demographic information included age, sex, race/ethnicity, BMI, alcohol use, tobacco use status within 1 year of operation, and several preoperative risk factors. Preoperative risk factors included ascites, bleeding disorder, pneumonia, cerebrovascular accident, diabetes, dialysis use, dyspnea, emergent case, congestive heart failure, myocardial infarction, hypertension, and having two or more of these conditions.
Logistic regression analyses determined the relationships between demographic data and risk factors and outcomes. The main outcomes of interest included all-cause complications, infectious complications, noninfectious complications, wound complications, 30-day mortality, and LOS >7 days. The following variables were examined with respect to the main outcome measures: type of intervention, emergent operation, gender, diabetes status, and year of operation. Analyses controlled for age, race/ethnicity, alcohol use history, tobacco use within 1 year of operation, BMI, and preoperative risk factors, including American Society of Anesthesiologists (ASA) class.
SAS, version 9.4 (Cary, NC), was used for all data analyses, with P < .05 used to determine significance.
Results
Demographics
There were 61,912 patients who underwent a cholecystectomy between 2006 and 2017. Patient demographics are shown in Tables 1 and 2. Patients were stratified according to year of operation (Table 1) and procedure type (open versus laparoscopic technique; Table 2). The majority of patients were male (85.3%), of white (67.5%) or black (10.4%) ethnicity, and almost half had a BMI >30 (44.2%). Approximately 5% of the population used alcohol and approximately a quarter were smokers within 1 year of operation. The most common preoperative risk factor across all years, procedure types, and geographic areas was diabetes (24.2%), followed by dyspnea (10.4%).
Patient Demographics and Preoperative Risk Factors by Year
Table demonstrates significant difference in variation between years for demographic factors and preoperative risk factors (save for cerebrovascular accident, diabetes, and emergency case). These variations demonstrate that the prevalence of most risk factors decreased over time, save for cardiovascular events, which may be explained by better reporting introduced in the time period. The clinical significance is that on aggregate, these values demonstrate healthier and less complicated patients over time.
Percent may not add to 100 due to rounding. Chi-square analysis where bold indicates significance at P < .05.
Analysis of variance.
ASA, American Society of Anesthesiologists; BMI, body–mass index; SD, standard deviation.
Patient Demographics and Preoperative Risk Factors by Procedure Type (Open Versus Laparoscopic)
Significant variation existed in all demographic categories and preoperative risk factors (save for congestive heart failure and myocardial infarction), when stratified by open and laparoscopic approach. The proportion of operations done laparoscopically increased over time, and most patients who underwent laparoscopic intervention presented with fewer risk factors. Many of these factors are controlled for in the logistic analyses.
Percent may not add to 100 due to rounding. Chi-square analysis where bold indicates significance at P < .05.
t-Test.
BMI, body–mass index; SD, standard deviation; VISN, Veterans Integrated Service Network.
Change over time
Over time, there were significant decreases in all complications (7.0% in 2006–08 versus 3.8% in 2015–2017; P < .001), infectious complications (5.4% versus 2.6%; P < .001), noninfectious complications (2.0% versus 1.1%; P < .001), wound complications (3.3% versus 1.7%; P < .001), 30-day mortality (0.7% versus 0.3%; P < .001), and the percent of the population with LOS >7 days (10.4% versus 6.8%; P < .001) (Table 3). These same trends persisted when dichotomized by open and laparoscopic interventions, with overall complication rates remaining higher for open interventions throughout each time period (P < .001). Results are visualized in Figure 1.

Laparoscopic trends compared with open intervention over time. Univariate analyses of the operative approach and outcomes between 2006 and 2017 (χ
2
P < .001).
Postoperative Complications by Year
There was significant variation in postoperative complications when stratified by year (P < .05). All metrics showed fewer postoperative complications over time, save for dehiscence (separation of the layers of a surgical wound, which may be partial or complete, with fascia disruption), pulmonary embolism, cardiac arrest, and DVT. Additionally, mortality and LOS were significantly lower at later time periods. Clinically, these percentage decreases point to significant aggregate decreases in morbidity and mortality over time, which may be correlated with increased training and familiarity with laparoscopic interventions in addition to hospital facilities being more able to accommodate this style of intervention.
Chi-square analysis where bold indicates significance at P < .05.
DVT, Deep Venous Thombosis; LOS, length of stay; SSI, Surgical Site Infection.
Laparoscopic versus open
There were significant differences in preoperative risk factors between patients who underwent a laparoscopic and open approach (Table 2). Every risk factor was significantly more prevalent (P < .001) in the open category than the laparoscopic category, except for congestive heart failure (P = .126) and myocardial infarction (P = .941). Additionally, there was a threefold greater proportion of emergent open cases compared with emergent laparoscopic cases (P < .001).
Postoperative outcomes demonstrated that patients who underwent open procedures, compared with laparoscopic procedures, had significantly more overall complications (15.4% versus 3.8%; P < .001); more infectious complications (e.g., superficial, deep, and organ space surgical site infections) (11.2% versus 2.8%; P < .001); more noninfectious complications (e.g., dehiscence, reintubation, and pulmonary embolisms) (4.7% versus 1.1%; P < .001); and more wound complications (8.1% versus 1.6%; P < .001). Additionally, mortality at 30 and 90 days postoperatively was lower for laparoscopic interventions (0.3% and 0.1% versus 1.4% and 0.4%, respectively; P < .001) and fewer patients had a hospital LOS >7 days (mean LOS 2.6 ± 4.8 days versus 6.4 ± 7.1 days; P < .001). Results are visualized in Table 4 and Figure 2. Significant differences in all outcomes persisted when stratified by gender (P < .001) and year (P < .001), although there were significantly fewer complications and lower mortality in women than men (P < .001).
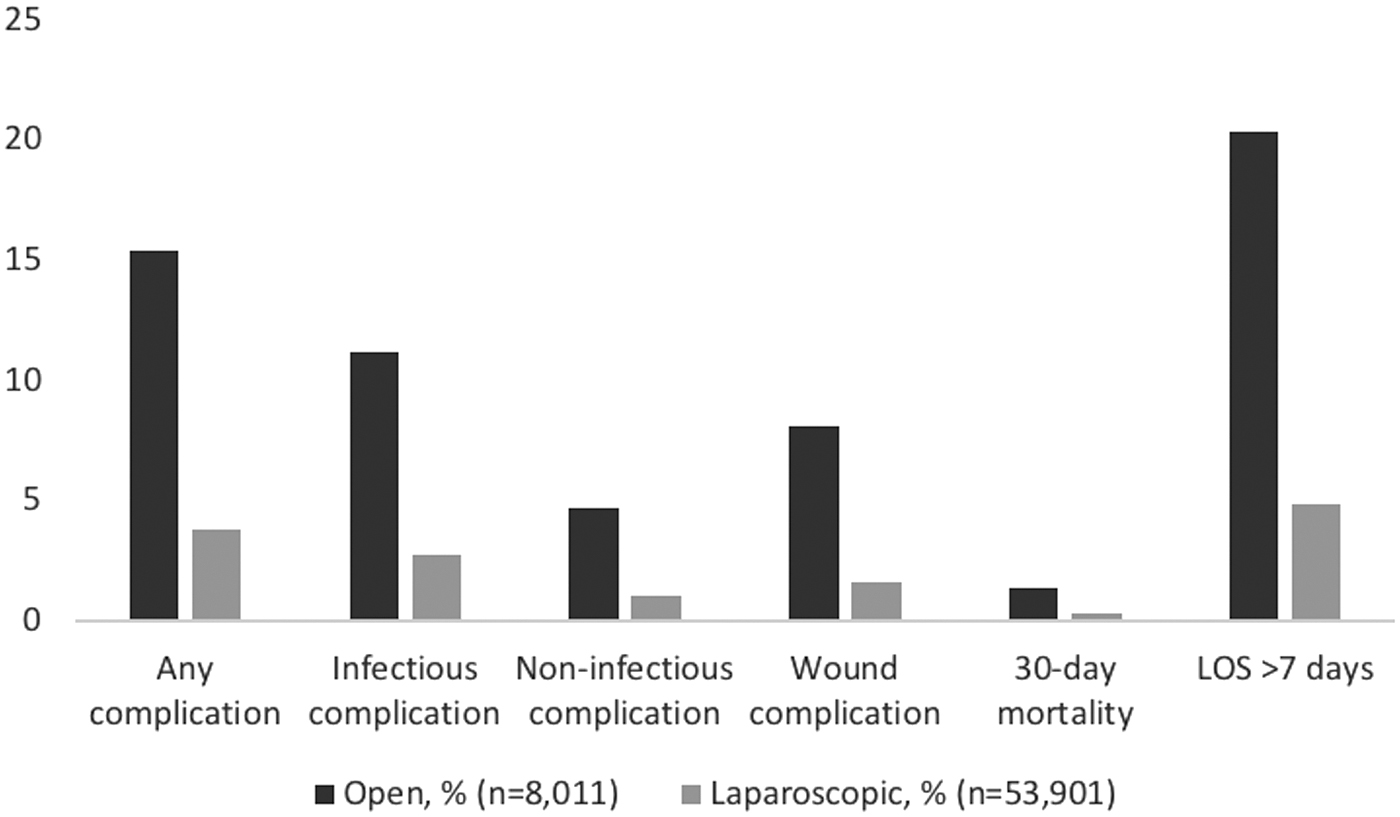
Complications by operation type. Univariate analyses of complications categorized between open and laparoscopic approaches, with significant differences for each complication (χ 2 P < .001).
Postoperative Complications by Procedure Type (Open Versus Laparoscopic)
There were significantly fewer (P < .001) postoperative complications across every outcome metric in the laparoscopic cohort than the open approach cohort. Patients who underwent laparoscopic procedures had fewer infectious, noninfectious, wound, and overall complications, as well as lower mortality and hospital LOS compared with patients who underwent open procedures. These clinically significant relationships are explored in more detail in the logistic regression analyses.
Chi-square analysis where bold indicates significance at P < .05.
t-Test.
LOS, length of stay; SD, standard deviation.
Regional demographic differences
Demographics and postoperative outcomes were stratified by geographic area. The majority of the surgeries occurred in the western states (n = 18,459), with the fewest in the Northeast (n = 13,312). Laparoscopy varied significantly (P < .001) with the greatest percentage in the West (88.3%) and the lowest percentage in the Northeast (85.9%). Among preoperative risk factors, nine varied significantly between geographical areas (P < .001). Diabetes varied significantly, with the most cases in the South (25.8%) and the fewest cases in the West (22.7%).
Logistic analyses
Upon logistic analyses, laparoscopic interventions demonstrated significantly lower adjusted odds ratios (AORs) for 30-day mortality (AOR = 0.5 [95% confidence interval, CI 0.4–0.7]; P < .001), any complications (AOR = 0.3 [95% CI 0.3–0.3]; P < .001), infectious complications (AOR = 0.3 [95% CI 0.3–0.3]; P < .001), noninfectious complications (AOR = 0.4 [95% CI 0.3–0.4]; P < .001), and wound complications (AOR = 0.2 [95% CI 0.2–0.2]; P < .001) after controlling for age, gender, year of operation, tobacco and alcohol use, BMI, comorbidities, functional status, emergent nature of operation, geographic region, and ASA class (Table 5). Laparoscopic techniques were associated with greater than 50% reduction in odds of complications across all morbidity and mortality criteria.
Adjusted Odds Ratio of Selected Outcome Metrics
Compared with the open approach, laparoscopic intervention was associated with a significantly lower odds of 30-day mortality (P < .001), any complication (<0.001), infectious complications (P < .001), and wound complications (P < .001). Emergent cases were compared with nonemergent cases and demonstrated significantly increased odds of any complication (P < .001) and noninfectious complications (P < .001). Female patients were compared with male patients and showed significantly reduced odds of wound complications (P < .001). Diabetes patients were compared with patients who did not present with diabetes and demonstrated significantly increased odds of any complication, infectious complications, noninfectious complications, and wound complications (P < .05). Finally, later year categories were compared with 2006–2008 and later years showed significantly reduced odds of all postoperative complications (P < .05), save for noninfectious complications in 2009–2011; additionally, 2015–2017 showed lower odds of 30-day mortality than 2006–2008 (P = .003). Controlling for how complicated patients can be on arrival further demonstrates the utility of the laparoscopic approach compared with the open approach.
Analyses adjusted for age, gender, tobacco and alcohol use, BMI, operative approach (laparoscopic versus open), comorbidities, functional status, emergent surgery, geographic region (Northeast, Midwest, South, and West), and ASA class.
Bold indicates significance at P < .05.
BMI, body–mass index; CI, confidence interval; OR, odds ratio.
Patients diagnosed with diabetes before their operation were significantly more likely to experience any complications (AOR = 1.1 [95% CI 1.0–1.2]; P = .003), infectious complications (AOR = 1.1 [95% CI 1.0–1.2]; P = .018), noninfectious complications (AOR = 1.2 [95% CI 1.1–1.4]; P = .009), and wound complications (AOR = 1.2 [95% CI 1.1–1.4]; P = .005). Women were significantly less likely to experience wound complications than men (AOR = 0.7 [95% CI 0.5–0.8]; P < .001). Geographic area was not a significant predictor of any major postoperative outcome (P > .05).
Discussion
The analysis of a nationwide sample of veterans across a 10-year period demonstrates that a laparoscopic versus an open cholecystectomy provides better outcomes after adjusting for various risk factors. Historically (2002–2010), open intervention is associated with greater odds of mortality (odds ratio = 3.3–6.0) and comorbidities than laparoscopy in both private and public hospital settings.7–10 Overall, the laparoscopic group in recent VASQIP cohorts demonstrated shorter hospital stays (mean LOS 2.6 ± 4.8 days versus 6.4 ± 7.1 days) compared with open intervention, which was lower than historical data. In addition, the data showed lower likelihood of mortality (AOR = 0.5 [95% CI 0.4–0.7]) and significantly fewer infectious (2.8% versus 11.2%), noninfectious (1.1% versus 4.7%), and wound (1.6% versus 8.1%) complications in the laparoscopic group compared with the open group. Decreased hospital LOS is associated with significant reduction in health care costs (as much as $300–2000 per day),11,12 opportunity cost from days taken off work, and potential reduction in morbidity. The decrease in complications and mortality may reflect improvements in surgical skill using laparoscopy along with hospital-wide improvements in managing and mitigating complications. 13
Open operations tend to be associated with more complicated patients 14 and this analysis did not have data for patients who underwent laparoscopic-to-open conversions; however, logistic analyses controlled for ASA class, emergent nature of operation, and functional status of patient. Future studies would benefit from inclusion of laparoscopic-to-open conversion data.
Studies suggest that hospital type plays a role in laparoscopic intervention and patient outcomes. A study from 2005 15 demonstrated an increased LOS, morbidity, and mortality following laparoscopic cholecystectomy in urban hospitals, teaching hospitals, and hospitals with a large number of beds. An additional study, 16 using 2011 data, reported that non-federal government facilities had lower major complication rates following cholecystectomy (8.3%) than for-profit (9.5%) and nonprofit (9.9%) private hospitals. Some of these data may derive from the American College of Surgeons National Surgery Quality Improvement Program, which collects data from private institutions. This contrasts with VASQIP, which pulls data from all VHA facilities. Our retrospective study of over 60,000 patients treated at VHA centers across the country demonstrates even lower complication rates at 5.3% across the entire time period. The complication rate decreased steadily across the study period from 7.0% in 2006–2008 to 3.8% in 2015–2017; additionally, all complication metrics decreased significantly over time. These findings further contribute to the discussion surrounding public and private health care systems, suggesting value in the VHA's approach and comprehensive health care offerings. The VHA has demonstrated greater processes of care than their non-VHA counterparts in a series of metrics, including with the management of diabetes, mental health, and preventative practices. 17 Again, the data appear to support the value of surgeon experience with laparoscopy over time and hospital-wide improvements in mitigating and treating complications. 13
Diabetes is one of the most commonly diagnosed chronic diseases in the United States and the seventh leading cause of death. 18 The Centers for Disease Control and Prevention estimates that 10%–13% of the U.S. population has some form of diabetes. 18 Diabetes is even more prevalent among veteran populations and may be twice the prevalence of the civilian population. 19 These statistics are corroborated by our findings, which suggest that approximately a quarter of veterans who underwent cholecystectomies were diabetics.
Diabetes is a significant risk factor for several gastrointestinal and postoperative complications, including gangrenous or emphysematous cholecystitis and wound dehiscence.20,21 Diabetes was additionally associated with a 1.1- to 1.2-fold greater risk of postoperative complications. Aggressive preoperative and postoperative glucose monitoring may mitigate the complications associated with diabetes following a cholecystectomy. This type of approach has been effective following coronary artery bypass surgery. 22 Further analysis would benefit from pre- and postoperative glucose values, which were not available for this study.
There were several limitations to this study. The data set does not delineate the difference between laparoscopic cases that were converted to open cases, nor does the data set discern the rationale for choosing an open approach especially during an emergent situation. Data were also missing for BDIs and future studies will need to elucidate these components. Unfortunately, the database does not discern the level of laparoscopic expertise, tenure of the surgeon, prior surgical history of the patient, or intraoperative anatomical findings. More refined geographical data, including zip code and income information, may have bolstered the results of this study. The retrospective nature of this study also limits the sampling capabilities. Potentially useful clinical variables, such as ultrasound-determined gallbladder thickness, conversion rates, or other laboratory indicators (including HbA1c levels) and BDIs, were unavailable with this data set. Conversion rates and BDIs may provide valuable insight into clinical outcomes for patients undergoing cholecystectomy and should be included in future research.
Conclusions
Our study suggests that veterans who undergo laparoscopic cholecystectomies versus an open technique encounter fewer complications and lower mortality. Clinical outcomes have improved over time possibly secondary to improvements in training, instrumentation, and postoperative care. Finally, preoperative diabetes is associated with increased morbidity postoperatively.
Footnotes
Authors' Contributions
Each author confirms that he or she made a meaningful contribution to the development of the manuscript. J.A.R. participated in data review and analysis, in addition to manuscript writing. S.C. collected data, assisted with analysis, and participated in conclusion formation. F.B. oversaw the project, participated in forming conclusions, and assessed the data.
Disclaimer
This material has not been published or submitted for publication elsewhere.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.