
Abstract
Background:
Indocyanine green (ICG) fluorescence imaging has been extensively used in a variety of applications in visceral surgery. In minimally invasive liver resections, the detection of small superficial hepatic lesions using an intravenous injection of ICG before surgery represents a promising application.
Methods:
We analyzed 18 consecutive patients who underwent laparoscopic liver resection for superficial malignant tumors, namely 11 patients with hepatocellular carcinoma (HCC), 5 patients with colorectal liver metastases (CRLM), 1 patient with intrahepatic cholangiocarcinoma (ICC), and 1 patient with thyroid cancer metastasis, using ICG fluorescence as an adjuvant tool to intraoperative laparoscopic ultrasound (LUS).
Results:
An optimal ICG 15-minute clearance retention rate (R15 < 10%) and ICG plasma disappearance rate (<18%/minute) were present in 11 patients (61.1%) and in 14 patients (77.7%), respectively. Liver tumors were 29 in total, including 14 HCCs (48.3%), 13 CRLMs (44.8%), 1 ICC (3.4%), and 1 thyroid cancer metastasis (3.4%). Twenty-nine tumors (100%) were correctly visualized with ICG/fluorescence, as compared with 21 tumors identified with LUS (72.4%). After complete liver mobilization, ICG staining allowed to identify more superficial lesions (early HCC and small CRLM) in posterolateral segments (Segments 6 and 7) as compared with LUS (14 versus 10 lesions). In addition, in segments usually treated laparoscopically (e.g., left lateral segments), ICG was superior to LUS (10 versus 6 lesions) to identify superficial early HCC in patients with macronodular cirrhosis.
Conclusions:
ICG visual feedback might substitute the tactile feedback of the hand and might in some cases act as a “booster” of LUS for superficial hepatic lesions.
Introduction
Indocyanine green (ICG) fluorescence imaging has been extensively used in a variety of applications in visceral surgery.1–3 Fluorescence-based cholangiography is among the most popular and promising ones. It aims to prevent bile duct injuries, thanks to an enhanced visualization of the extrahepatic biliary anatomy during cholecystectomy.4–7
Another promising application of fluorescence imaging is the detection of small superficial hepatic lesions using an intravenous injection of ICG before surgery. The first application of this technique was reported in 2009 by Ishizawa et al. 8 and Gotoh et al. 9
A single dose of ICG (generally 0.5 mg/kg) used for routine liver function tests (with the LiMON® device) is sufficient to identify tumors using intraoperative fluorescence imaging.
Detection of hepatic lesions by fluorescence is based on the contrast between tumoral or peritumoral fluorescent tissue and the nonfluorescent remaining liver parenchyma.
ICG-based fluorescence takes advantage of the preserved uptake but impaired washout of the dye from the hepatocellular carcinoma (HCC) into bile, owing to the downregulation of ligandin and other transporter proteins in damaged liver tissue. 10
Fluorescence patterns are related to the type of cancer and to its grade of differentiation. Well-differentiated HCCs show strong and homogeneous fluorescence emission, in contrast to moderately and poorly differentiated HCCs that produce partial or peritumoral fluorescence imaging. For tumors formed by nonhepatocyte cells, such as colorectal liver metastases (CRLM), the rim-type fluorescence signal is owing to compressed hepatocytes surrounding the metastatic lesion with a decreased bile excretion ability. 9 There is little evidence regarding other primary hepatic tumors containing predominantly epithelial cells such as cholangiocarcinoma. A recent study 11 described two different patterns of fluorescence for two distinct types of intrahepatic cholangiocarcinoma (ICC). Mass-forming ICC showed peritumoral fluorescence, whereas mixed-type ICC (mass forming plus periductal infiltration pattern) revealed segmental fluorescence owing to dye retention in the involved bile duct.
In this study, we reported our preliminary experience in minimally invasive liver resection using a preoperative intravenous injection of ICG as a visual feedback adjuvant to laparoscopic ultrasound (LUS) for the detection of superficial hepatic tumors.
Materials and Methods
Ethics
This study was conducted in accordance with the Declaration of Helsinki (6th revision, 2008) of the World Medical Association. The study was approved by the Institutional Review Committee (IRC) of the Department of Health Sciences, University of Milan, Italy. All patients signed an informed consent.
Study design
From April 2019 to January 2020, all patients undergoing laparoscopic liver resection (LLR) for superficial (<8 mm from the hepatic surface) malignant tumors at our HepatoBilioPancreatic Surgical Unit, using ICG fluorescence imaging as an adjuvant tool to intraoperative LUS were consecutively enrolled in the study. Hepatic tumors included HCC (n = 14), colorectal liver metastases (CRLM; n = 13), ICC (n = 1), and noncolorectal liver metastases (NCRLM; n = 1). Patients presenting with deeply seated lesions and those with contraindications to ICG injection such as allergy to iodinated contrast medium or thyroid dysfunction were excluded. Before surgery, all patients underwent a computed tomography (CT) scan and magnetic resonance (MR) of the abdomen with hepatobiliary contrast. During preoperative admission, an ICG clearance test measured with the LiMON device (Pulsion, Germany) was performed in all subjects. The ICG plasma disappearance rate (PDR %/minute) and ICG 15-minute clearance retention rate (R15%) were measured by means of pulse spectrophotometry after an intravenous bolus injection of ICG dye at a dose of 0.5 mg/kg of body weight. The ICG test was performed 5 days before CRLM or NCRLM and 7 days before HCC or ICC resection. No additional ICG was injected intraoperatively.
Surgical technique and intraoperative imaging modalities
A standardized laparoscopic surgical technique was performed in all cases by extensively trained hepatobiliary surgeons with experience in intraoperative LUS. To evaluate the number and the location of the lesions, all patients underwent laparoscopic staging with both LUS and ICG fluorescence imaging by means of a 4 k magnified ultra-high-definition video system optimized for near-infrared visualization (KARL STORZ, Tuttlingen, Germany). The video system captured the fluorescence signal of the residual ICG, which was entrapped in the tumor lesions. ICG staining was also used to provide a real-time feedback of the surgical margin status.
Results
Patient characteristics are given in Table 1. An optimal ICG 15-minute clearance retention rate (R15 < 10%) and ICG PDR (<18%/minute) were present in 11 patients (61.1%) and in 14 patients (77.7%), respectively. A total of 29 liver tumors were found, including 14 HCCs (48.3%), 13 CRLMs (44.8%), 1 ICC (3.4%), and 1 NCRLM (3.4%). Lesions were divided into three groups according to their size: <1 cm (24.1%), 1–2 cm (44.8%), and >2 cm (31.1%).
Patients Characteristics
CRLM, colorectal liver metastases; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; ICG, indocyanine green; NCRLM, non colorectal liver metastases; PDR, plasma disappearance rate.
All 29 tumors (100%) were correctly visualized with ICG/fluorescence, as compared with 21 with LUS (72.4%).
No additional malignant tumors were identified using intraoperative LUS or ICG/NIR fluorescence imaging. There were no false-positive uptakes of ICG in the liver parenchyma. Distribution of liver tumors and the total number of lesions detected with LUS and ICG/fluorescence in each segment (according to the Couinaud classification) were analyzed; data are provided in Table 3. After complete liver mobilization, ICG staining allowed to identify more small superficial lesions in the right posterolateral segments (Segments 6 and 7) as compared with LUS (14 versus 10 lesions), including both HCC (Fig. 1 and Supplementary Video S1) and CRLM lesions (Fig. 2 and Supplementary Video S2).
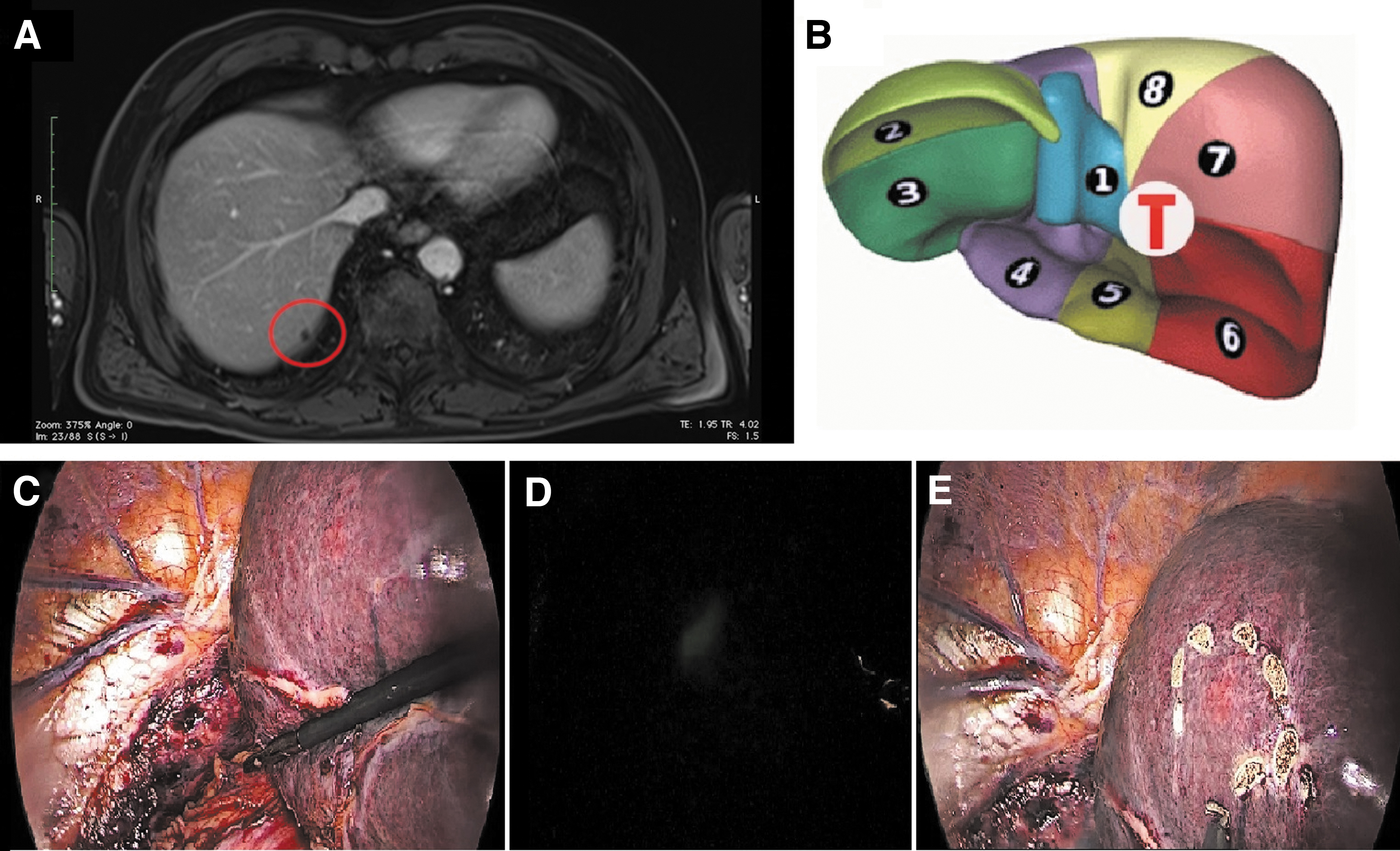
Patient with a lesion in S6.
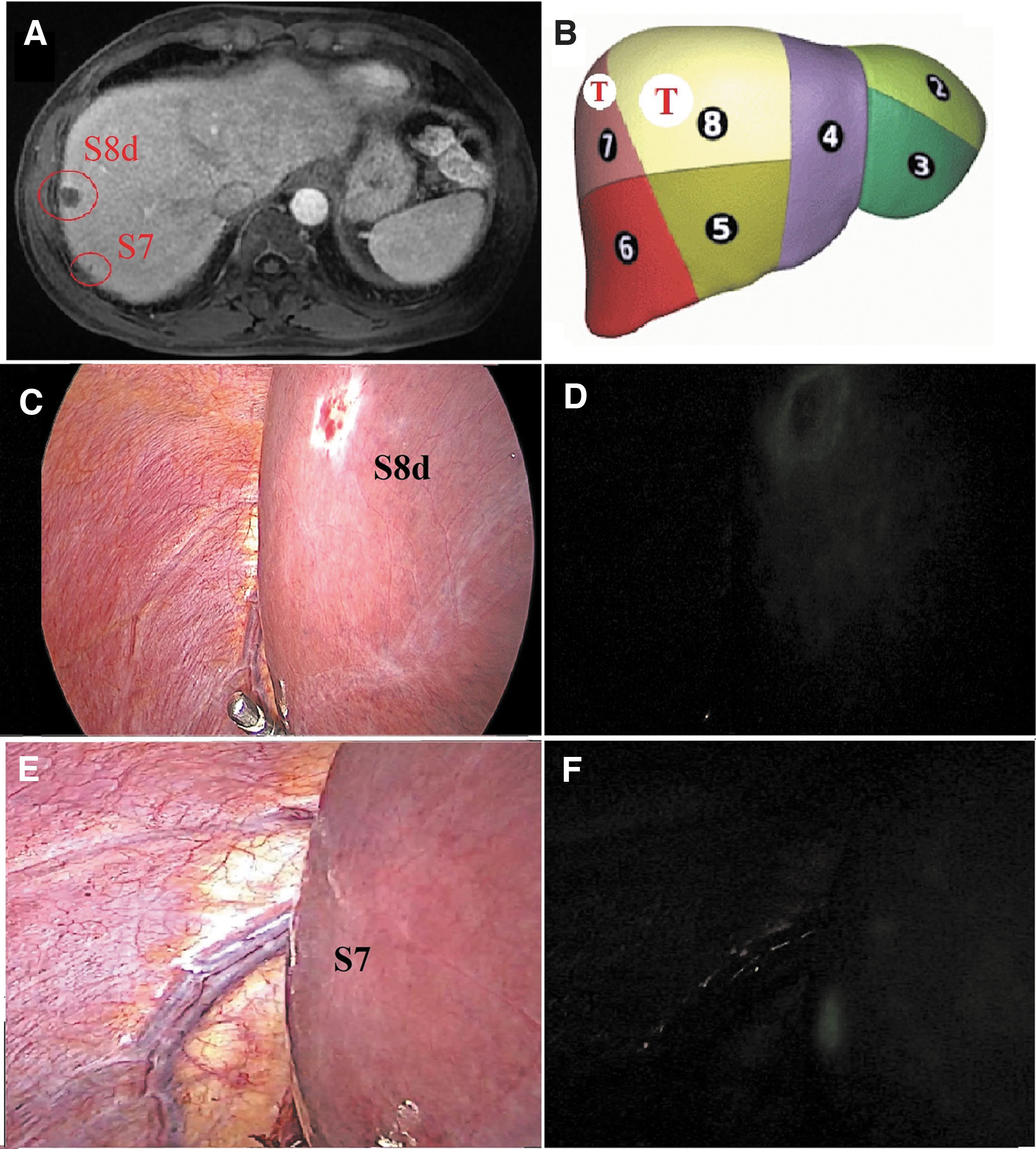
Patient with a lesion in S8d and in S7.
Distribution of Hepatic Lesions Detected by Preoperative Imaging, Laparoscopic Ultrasound and Indocyanine Green Staining
ICG, indocyanine green; LUS, laparoscopic ultrasound.
In addition, in segments usually treated with laparoscopy such as left lateral segments (Segments 3 and 2), ICG was superior to LUS in the detection of superficial early HCC (10 versus 6 lesions) in patients with macronodular cirrhosis (Fig. 3 and Supplementary Video S3).
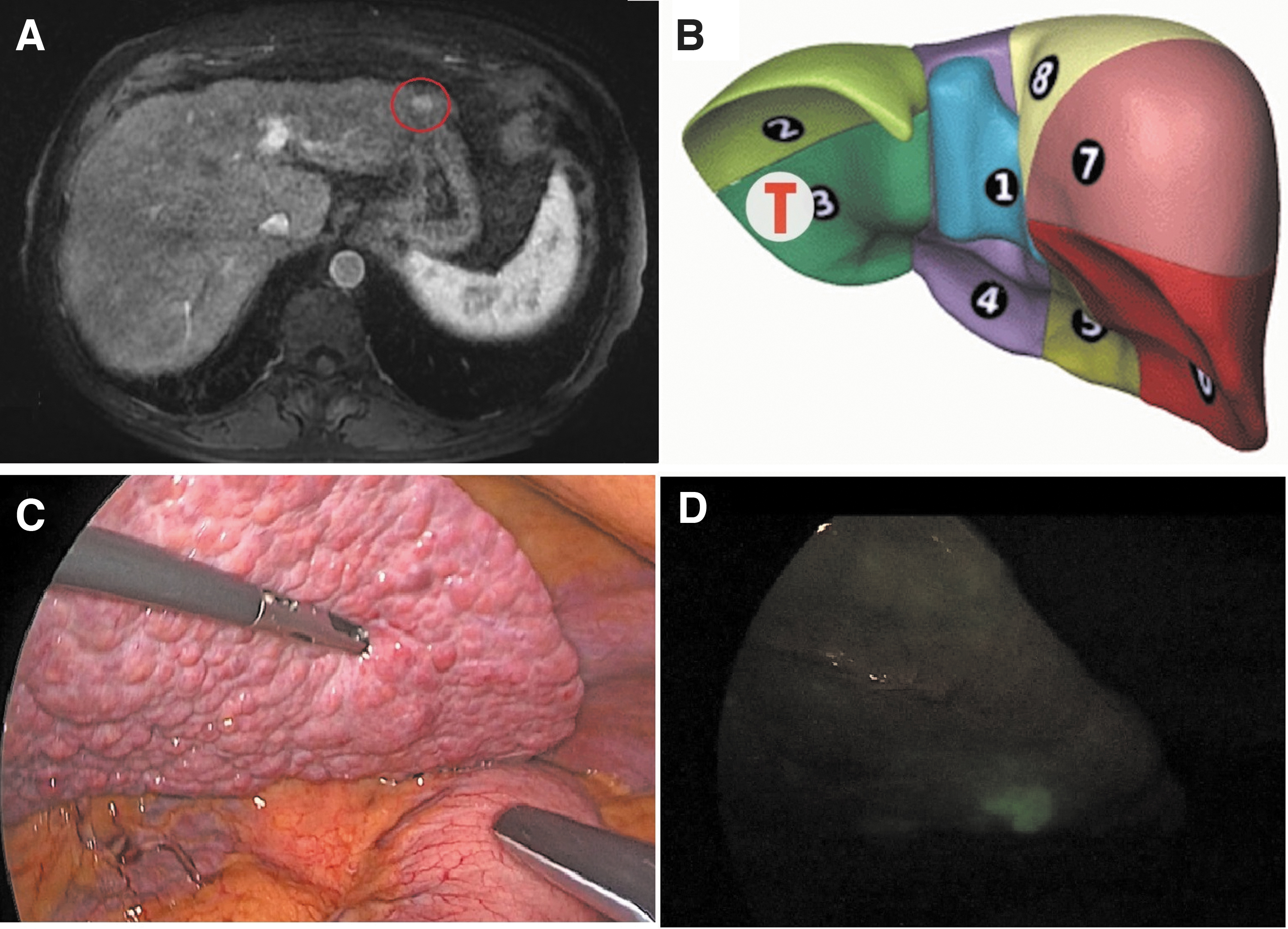
Patient with a lesion in S3.
There were no adverse events caused by ICG intravenous injection. The majority of patients underwent a wedge or a minor liver resection (Table 2). Mean operative time was 238 minutes. There were no conversions from laparoscopy to laparotomy. R0 resection was achieved in 100% of cases, with a median margin width of 10.7 mm. None of the patients required blood transfusion intraoperatively. Postoperative complications were classified according to the Clavien-Dindo classification. Three patients (16.7%) developed grade II complications: acute kidney injury owing to intraoperative hypoperfusion, successfully treated with infusion therapy, heart failure, and a biliary leak. A grade IIIa complication occurred in 1 (5.5%) patient who developed an intra-abdominal fluid collection, which required percutaneous drainage. Mean hospital stay was 7 days.
Surgical Procedure, Intra- and Postoperative outcomes of Patients
Discussion
In laparoscopic surgery where tactile feedback is missing, the use of intraoperative ultrasound plays a critical role. Introduced for the first time in 1981 by Fukuda, 12 LUS has shown a remarkable diffusion over time, both as a staging technique and as a guide for liver resections or thermal ablation procedures. 13 However, LUS has drawbacks and limitations, and difficulty in interpreting images is one of the most important ones. The learning curve of the operators is not defined by any validated protocol. 14 The accuracy of LUS is not only dependent upon the operator's skills, but it is also affected by the size of the lesions and the quality of the hepatic parenchyma. An irregular hepatic surface can modify ultrasound images, because of the interposition of air between the probe and the liver surface.15,16
The accurate mapping of the lesions is also limited by the position of the trocars, which affects the angle of incidence of ultrasonic waves. 17
Today, ICG fluorescence imaging is a promising method for navigation surgery, which allows to overcome the abovementioned limitations.
In a minimally invasive setting, ICG fusion images can mimic the tactile feedback of the hand, in some cases act as a “booster” of LUS for the detection of superficial nodules, also in patients with macronodular cirrhosis and irregular liver surface.18–20
In our series, LUS and ICG staining were routinely performed to evaluate the site of the hepatic lesions. Twenty-nine tumors (100%) were correctly visualized with ICG/fluorescence, as compared with only 21 with LUS (72.4%). The lesions that were unidentified with LUS were smaller (size <1 cm) and localized in posterolateral segments (Segments 6/7) or at the edge of Segments 3 and 2 in patients with macronodular alterations. Although they represent a promising finding, conclusions cannot be drawn at this point, given the small number of patients included.
So far, only a few authors have evaluated the application of ICG fluorescence as an adjuvant to LUS.18,21
In a prospective study including 22 patients affected by primary and metastatic liver tumors, Boogerd et al. 18 compared standard preoperative imaging work-up (CT and MR of the abdomen) with intraoperative imaging modalities, such as visual inspection, LUS, and ICG/Near Infrared (NIR) fluorescence.
The authors reported that ICG/NIR fluorescence imaging had the highest sensitivity rate among all imaging modalities (92.3%). A combination of NIR fluorescence with LUS allowed for the detection of all lesions (100%). In addition, three occult colorectal liver metastases (CRLM), which were not identified using preoperative modalities, were detected intraoperatively by using the combined modality (LUS plus NIR).
In our study, neither LUS nor ICG imaging allowed to identify any additional lesions. As already mentioned, this is probably because of the limited number of patients included.
There were no adverse events related to ICG injection, which is known to have a high safety profile, with a reported incidence of adverse events as low as 0.003%. 8
ICG imaging is very rapid and perfectly integrated in the surgical workflow because fluorescent images of liver tumors are obtained by simply targeting the liver surface with the camera and switching the camera system to the near-infrared function.
In our series, a single dose of ICG (generally 0.5 mg/kg), used for routine liver function tests (LiMON test) up to 1 week before surgery, was sufficient to obtain sharp images. This is definitely an advantage, because no additional ICG injections are required intraoperatively.
In addition, the ICG fusion image modality allowed to define a sharp transection line, providing a real-time feedback of the surgical margin status.
However, there are two important drawbacks of this technique, namely the depth of fluorescence penetration (up to 8 mm from the liver surface) and the relatively high false-positive rate (from 24% to 40%).15,22 In fact, ICG retention can also occur in benign nodules, such as high-grade dysplasia, regenerative nodules, biliary hamartomas, and focal nodular hyperplasia.18,21
According to some authors, 23 the resection of nodules newly identified with fluorescence should be considered only for superficial lesions >8 mm in diameter and with a strong fluorescence.
New technologies have recently been developed, which can measure the intensity of the fluorescent signal in this regard. Other authors have suggested that the additional resection of ICG fluorescent nodules of unclear nature may be considered only when surgery of the hepatic segment involved does not increase morbidity. 19
The timing of ICG injection may also affect the rate of false positives, even if a correct timing has not yet been standardized (ranging from 24 hours to 17 days before surgery in the literature).18–24
As a result, further technological improvements are necessary. Experimental studies involving intrahepatic artery ICG injection using celiac trunk catheterization have been published recently, with the aim of achieving precise detection of liver segmentation that was not time dependent. 25
Conclusions
Lesion identification during LLR remains challenging. Our preliminary results suggest that the addition of ICG fluorescence to LUS increases intraoperative visualization, especially of smaller lesions, posteriorly located, in the setting of nodular cirrhosis. The ICG visual feedback could substitute the tactile feedback of the hand and could in some cases act as a “booster” of LUS for superficial hepatic lesions. We believe that this technique could play a major role in minimally invasive hepatic surgery in the future.
Footnotes
Disclosure Statement
M.D. is a member of the Advisory board of Diagnostic Green and is the recipient of the ELIOS Grant. The following doctors, that is, G.P., M.B., E.L.M., G.E, F.L., R.S., and E.O. have no conflicts of interest or financial ties to disclose.
Funding Information
The authors received no funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.