
Abstract
Background:
Percutaneous gallbladder drainage (PTGBD), endoscopic ultrasound-guided gallbladder drainage (EUSGBD), and endoscopic transpapillary gallbladder drainage (ETGBD) are used for the treatment of patients with acute cholecystitis who are at high surgical risk. However, it is unclear which procedure is associated with the best outcomes.
Methods:
We systematically searched records in PubMed, Embase, Web of Science, the Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov up to March 1, 2020. Studies that compared at least two of PTGBD, ETGBD, and EUSGBD were included.
Results:
A total of 13 studies were included in the present analyses. PTGBD, EUSGBD, and ETGBD were associated with similar clinical success, adverse event, recurrent cholecystitis, reintervention, and mortality rates. PTGBD was associated with a higher technical success rate than EUSGBD (odds ratio [OR] = 0.75, 95% confidence interval [CI] = 0.40–1.41) or ETGBD (OR = 0.73, 95% CI = 0.35–1.53). EUSGBD was associated with the highest probability of clinical success (67.5%), and the lowest prevalences of adverse events (57.0%) and recurrent cholecystitis (60.9%). ETGBD was associated with the best reintervention outcomes (81.8%).
Conclusions:
Compared with PTGBD and ETGBD, EUSGBD appears to be preferable with respect to both safety and efficacy for the treatment of patients with acute cholecystitis who are at high surgical risk.
Introduction
Acute cholecystitis requires appropriate management in its acute phase. Early cholecystectomy should be considered if patients are in an appropriate condition. However, some patients are at high surgical risk and are unsuitable for cholecystectomy. 1 Urgent biliary drainage is of particular importance for these patients. Percutaneous gallbladder drainage (PTGBD) has been the standard procedure to date for emergency gallbladder drainage. 2 However, it can be associated with tube dysfunction, bile leakage, the necessity for reintervention, and a reduction in the patient's quality of life.3,4
Recent studies have shown that endoscopic gallbladder drainage is a viable alternative option for the therapy of acute cholecystitis.5,6 Endoscopic transpapillary gallbladder drainage (ETGBD) was described in 19847 and endoscopic ultrasound-guided gallbladder drainage (EUSGBD) was first described in 2007. 8 ETGBD and EUSGBD have the advantage of internal drainage, which improves postoperative quality of life. However, endoscopic gallbladder drainage is associated with several potential complications, such as perforation, bleeding, pancreatitis, and stent migration, and requires a high level of technical expertise.9–11
Several previous studies have compared the use of PTGBD, ETGBD, and/or EUSGBD.5,12–14 However, the results of these studies conflicted, the sample sizes were small, and no network meta-analysis has been performed to compare these three procedures. In addition, several new studies have recently been published. Therefore, we conducted the first network meta-analysis of the efficacy and safety of PTGBD, ETGBD, and EUSGBD for the treatment of patients with acute cholecystitis who are at high surgical risk.
Methods
Search strategy
The present study is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15 Two independent authors performed a systematic search of records in the PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov databases up to March 1, 2020. Consistent combinations of the following search terms were used: EUSGBD, EUS-guided gallbladder drainage, PTGBD, ETGBD, endoscopic gallbladder drainage, percutaneous cholecystostomy, and PTGBD. The search was restricted to studies conducted in humans and English-language articles. Any discrepancies regarding study selection were resolved by discussion between the authors.
Eligibility criteria
Only studies that compared at least two of PTGBD, EUSGBD, and ETGBD were included in the review. The exclusion criteria were: (1) studies that did not compare at least two groups; (2) letters, case reports, editorials, and review articles; and (3) studies that did not provide sufficient data regarding the outcome measures.
Outcome measures
The primary outcomes of interest were technical success, clinical success, and adverse events. The secondary outcomes of interest were the prevalences of reintervention, recurrence of cholecystitis, and mortality. Technical success was defined as the correct placement of a stent or drainage tube, confirmed by appropriate drainage of bile. Clinical success was defined as the resolution of symptoms and the normalization of laboratory data within 7 days.
Data extraction
Two authors extracted the original data from the literature. Data were collected using a standardized selection form, which included the first author, year of publication, type of study, country in which the study took place, type of intervention, and sample size. Conflicts in the data obtained were resolved by discussion and by referring to the original article. The extracted data were entered into a pregenerated Microsoft Excel file (Microsoft Corporation, Redmond, WA).
Risk of bias assessment
The quality of the literature was assessed using the Newcastle–Ottawa scale (NOS), according to three parameters: selection, comparability, and exposure/outcome, which had maximum scores of 4, 2, and 3 points, respectively. 16 Studies with a total NOS score >7 were defined as being of high quality.
Statistical analyses
The meta-analysis was performed according to the PRISMA extension statement, incorporating Network Meta-analyses of Health Care Interventions. 17 Statistical analyses were performed using STATA version 13.0 software (Stata Corp, College Station, TX). Odds ratios (ORs) and 95% confidence intervals (CIs) are used to report dichotomous outcomes. The surface (area) under the cumulative ranking (SUCRA) curve was calculated as a measure of the probability that each approach would be the best option. We calculated the safety (adverse event rate)/efficacy (clinical or technical success rate) ratio using the SUCRA values. Publication bias, inconsistency, and heterogeneity were assessed according to the PRISMA extension statement, incorporating Network Meta-analyses of Health Care Interventions. 17 Inconsistency was evaluated using the “loop” approach 18 and heterogeneity was assessed using tau-squared (variance of the random effects distribution). 19 We also assessed the potential for publication bias by visually inspecting funnel plots for asymmetry. A two-tailed P value of <.05 was considered to represent statistical significance.
Results
Study selection and characteristics
A flowchart of the literature search process is shown in Figure 1. We identified a total of 498 articles in our initial screen of titles and abstracts. Of these, 101 were excluded because of duplication, and 396 studies were examined further, of which an additional 373 were excluded for various reasons. Therefore, 13 studies of 2203 participants met the eligibility criteria.12–14,20–29
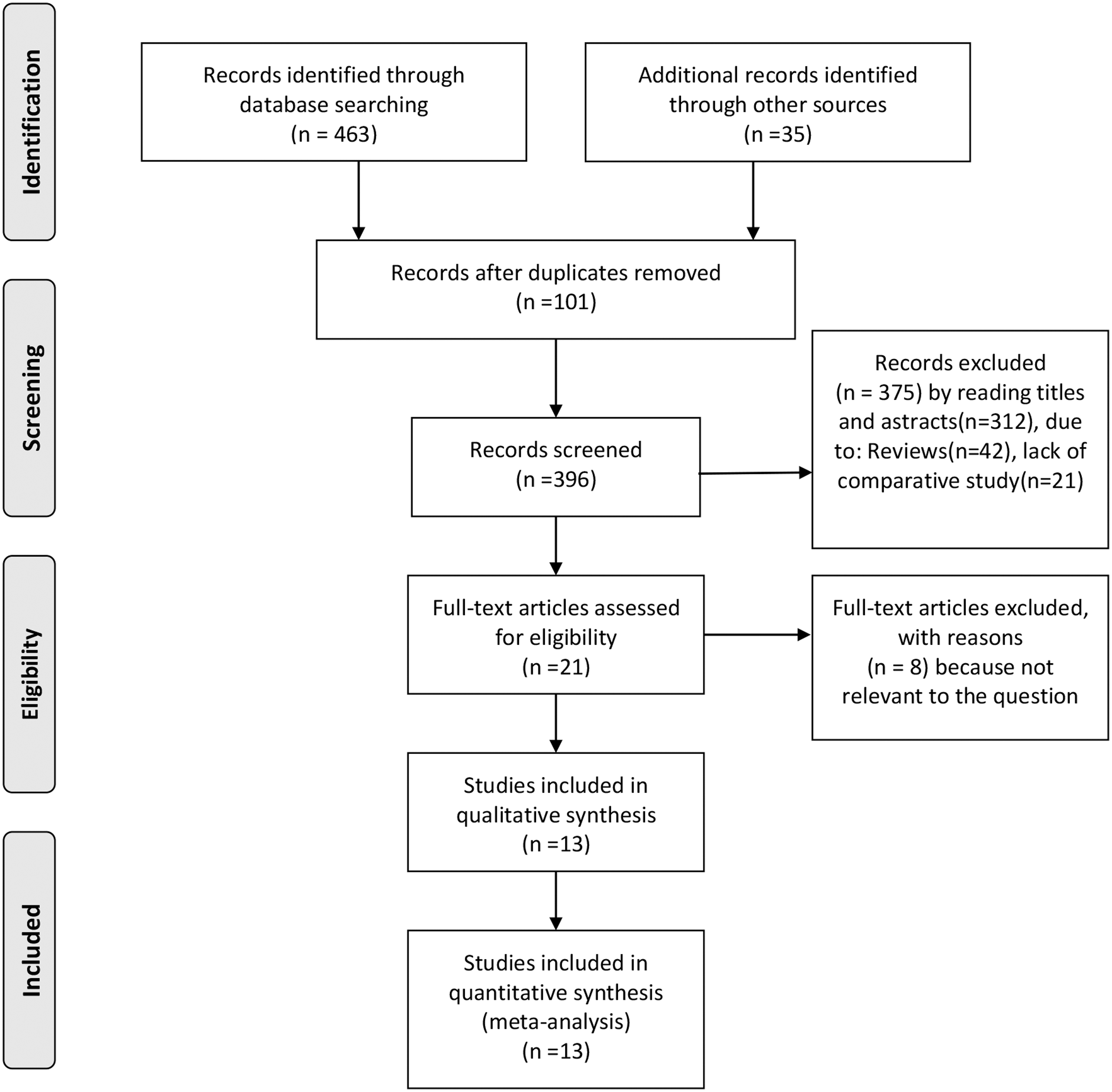
Flow diagram of the published articles evaluated for inclusion in the present meta-analysis.
The characteristics and quality evaluation of the included studies are shown in Table 1. A total of 12 retrospective studies12,13,20–29 and one randomized controlled trial (RCT) were included in the present meta-analysis. 14 Seven studies compared PTGBD with EUSGBD, four compared EUSGBD with ETGBD, three compared ETGBD with PTGBD, and one compared all three interventions. A total of 755 patients underwent PTGBD, 478 underwent EUSGBD, and 970 underwent ETGBD. The quality of the included studies, assessed using the NOS, is summarized in Table 1. All of the included studies were found to be of high quality, with NOS scores >7.
The Characteristic of Included Studies
ASA, American Society of Anesthesiologist; CCI, Charleston Comorbidity Index; ETGBD, endoscopic transpapillary gallbladder drainage; EUSGBD, endoscopic ultrasound-guided gallbladder drainage; NOS, Newcastle–Ottawa scale; PTGBD, percutaneous transhepatic gallbladder drainage; RCT, randomized controlled trial; Retro, retrospective study.
Primary outcomes
Clinical success
As shown in Figure 2a, 12 studies provided clinical success rate data for 1969 patients. Network estimates showed that there were no significant differences in the clinical success rate of the three endoscopic methods (EUSGBD versus PTGBD: OR = 1.14, 95% CI = 0.48–2.70; ETGBD versus PTGBD: OR = 0.67, 95% CI = 0.26–1.74; ETGBD versus EUSGBD: OR = 0.58, 95% CI = 0.24–1.43) (Fig. 3a). However, EUSGBD tended to be the most clinically successful technique (SUCRA, 67.5%), followed by PTGBD (SUCRA, 56.1%) and ETGBD (SUCRA, 26.4%) (Table 2).
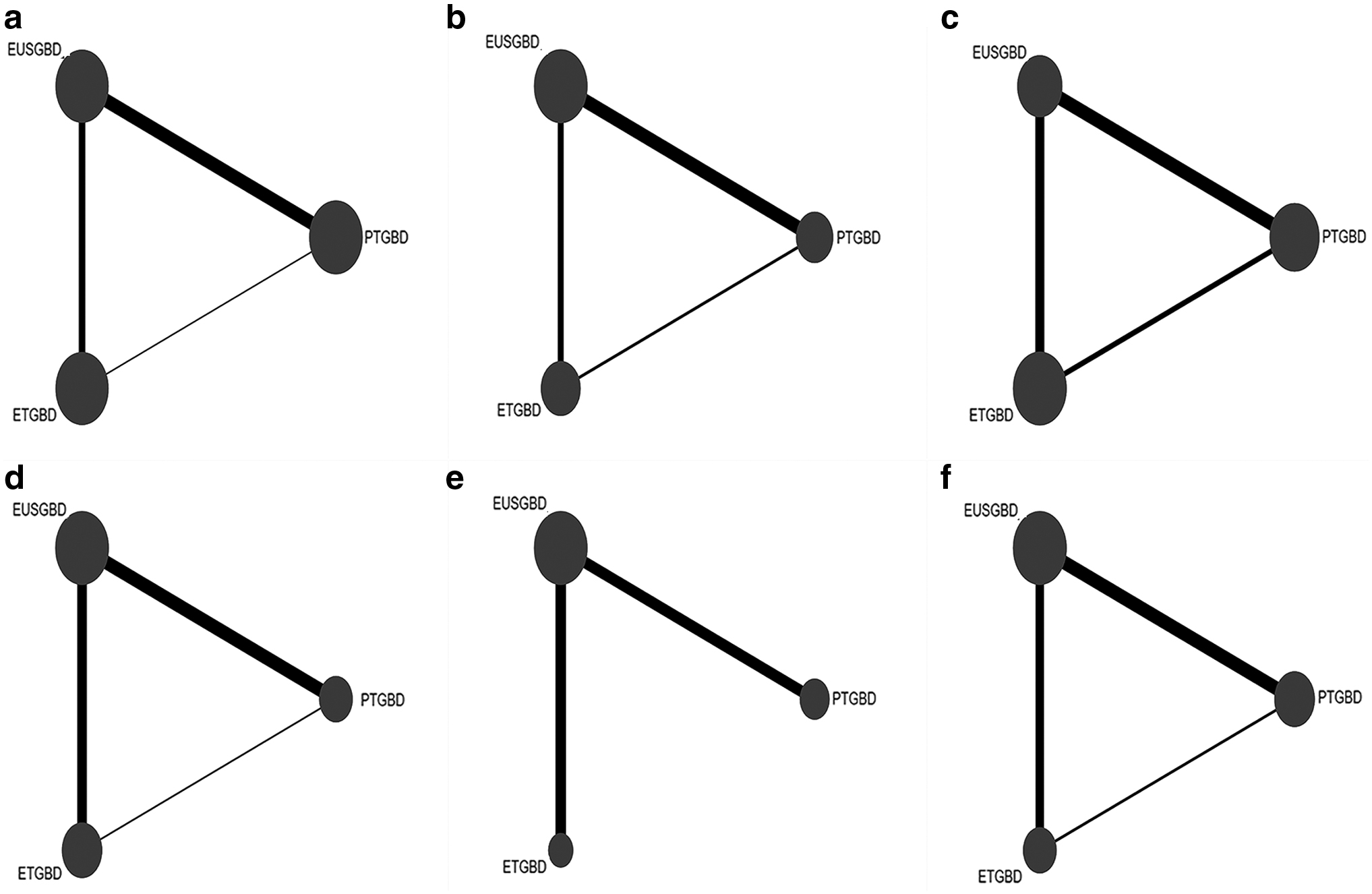
Network geometry for all the outcomes.

Forest plots for all the outcomes.
Surface (Area) Under the Cumulative Ranking Values for All Outcomes
ETGBD, endoscopic transpapillary gallbladder drainage; EUSGBD, endoscopic ultrasound-guided gallbladder drainage; PTGBD, percutaneous transhepatic gallbladder drainage.
Technical success rate
The technical success rate was reported for 12 studies of 1607 patients (Fig. 2b). PTGBD had a higher technical success rate than EUSGBD or ETGBD (OR = 0.33, 95% CI = 0.13–0.80 and OR = 0.07, 95% CI = 0.02–0.23, respectively) and EUSGBD had a higher technical success rate than ETGBD (OR = 0.22, 95% CI = 0.08–0.60) (Fig. 3b). The SUCRA values for the technical success rates were 98.4%, 51.1%, and 0.5% for PTGBD, EUSGBD, and ETGBD, respectively (Table 2).
Adverse events
As shown in Figure 2c, all 13 studies provided data regarding adverse events. There were no significant differences among the three methods with regard to the prevalence of adverse events (EUSGBD versus PTGBD: OR = 0.75, 95% CI = 0.40–1.41; ETGBD versus PTGBD: OR = 0.73, 95% CI = 0.35–1.53; ETGBD versus EUSGBD: OR = 0.98, 95% CI = 0.49–1.95) (Fig. 3c). However, EUSGBD tended to be associated with the fewest adverse effects (EUSGBD SUCRA, 70.6% versus ETGBD SUCRA, 57.5% and PTGBD SUCRA, 21.9%) (Table 2).
Secondary outcomes
Recurrent cholecystitis
A total of 9 studies of 1386 patients calculated the prevalence of recurrent cholecystitis (Fig. 2d). There were no significant differences in the prevalences of recurrent cholecystitis among the three methods (EUSGBD versus PTGBD: OR = 0.71, 95% CI = 0.17–2.94; ETGBD versus PTGBD: OR = 1.90, 95% CI = 0.18–6.68; ETGBD versus EUSGBD: OR = 1.54, 95% CI = 0.38–6.25) (Fig. 3d). However, EUSGBD tended to be associated with the lowest prevalence of recurrence (EUSGBD SUCRA, 60.9%, versus ETGBD SUCRA, 43.0% and PTGBD SUCRA, 46.2%) (Table 2).
Reintervention
The reintervention rate was reported for eight studies (Fig. 2e). There were no significant differences in the reintervention rate among the three methods (EUSGBD versus PTGBD: OR = 0.38, 95% CI = 0.11–1.31; ETGBD versus PTGBD: OR = 0.17, 95% CI = 0.02–1.57; ETGBD versus EUSGBD: OR = 0.45, 95% CI = 0.08–2.62) (Fig. 3e). However, ETGBD had the highest SUCRA (79.8%), followed by EUSGBD (SUCRA, 53.4%) and PTGBD (SUCRA, 16.8%) (Table 2).
Mortality
Mortality data were available for 9 studies of 1386 patients (Fig. 2f). There were no significant differences among the three methods with regard to mortality rate (EUSGBD versus PTGBD: OR = 2.54, 95% CI = 0.49–13.19; ETGBD versus PTGBD: OR = 2.23, 95% CI = 0.31–16.19; ETGBD versus EUSGBD: OR = 0.88, 95% CI = 0.25–3.08) (Fig. 3f). The SUCRA values for PTGBD, EUSGBD, and ETGBD were 81.8%, 29.1%, and 39.2%, respectively (Table 2).
Cluster ranking of the three methods
Using the clinical success rate as an indicator of efficacy and the adverse event rate as an indicator of safety, EUSGBD was found to be the best method with respect to both safety and efficacy, followed by PTGBD and ETGBD (Fig. 4a). A similar result was also obtained when using the technical success rate as an indicator of efficacy and the adverse event rate as an indicator of safety (Fig. 4b).

Cluster ranking combining the SUCRA curve values.
Inconsistency, heterogeneity, and publication bias
The inconsistency and heterogeneity for each procedure are shown in Table 3. There was no significant local inconsistency within the networks with respect to any of the outcome measures. The heterogeneities of the data for technical success and mortality data were low (τ < 0.1), but were high for the clinical success, adverse event, recurrent cholecystitis, and readmission rate data. The comparison-adjusted funnel plots suggested that there was no significant publication bias.
Loop Inconsistency and Heterogeneity
A, percutaneous transhepatic gallbladder drainage (PTGBD); B, endoscopic ultrasound-guided gallbladder drainage (EUSGBD); C, endoscopic transpapillary gallbladder drainage (ETGBD); CI, confidence interval; ROR, logarithm of the ratio of 2 odds ratios.
Discussion
To our knowledge, this is the first network meta-analysis to compare the success and safety of PTGBD, EUSGBD, and ETGBD. In the present study, we have shown that EUSGBD tends to be associated with the highest rate of clinical success, the fewest adverse events, and the lowest incidence of recurrent cholecystitis. PTGBD was associated with the highest rate of technical success and tended to be associated with the least mortality. If clinical or technical success is used as an indicator of efficacy and the frequency of adverse events as an indicator of safety, EUSGBD was associated with the best safety and efficacy overall. However, high-quality head-to-head RCTs are required to confirm these findings.
Previous studies did not reach a consensus with regard to the clinical success of each technique. A previous meta-analysis of five studies containing a total of 495 patients in which EUSGBD and PTGBD were compared revealed similar clinical success rates (OR = 1.07, 95% CI = 0.36–3.16; P = .90). 30 This result is consistent with those obtained in several previous studies, including one RCT.14,22,29 In the present study, EUSGBD tended to be associated with a higher clinical success rate than PTGBD, although the difference was not significant. The results of comparisons of EUSGBD and ETGBD have also been contradictory. A recent study conducted by Teeratorn et al. showed similar clinical success rates for EUSGBD and ETGBD, 27 but after the inclusion of recent studies, the present network meta-analysis showed that EUSGBD tends to be more clinically successful than ETGBD, and a similar result was also obtained in the study conducted by Krishnamoorthi et al. 31 The use of lumen-apposing metal stents in EUSGBD can increase its clinical success, and the reported clinical success rate was variable in previous studies, probably as a result of selection bias and differences in the type of stents used in EUSGBD.
There have been few comparisons of PTGBD and ETGBD with respect to clinical success rate. Siddiqui et al. showed that ETGBD is less clinically successful than PTGBD, 26 whereas Itoi et al. showed that the two techniques have a similar clinical success rate. 21 The present study shows that PTGBD may be preferable to ETGBD, but the difference was not statistically significant. It is worth noting that the definition of clinical success varied among the previous studies; therefore, further high-quality head-to-head studies are required to circumvent this issue.
The present study has shown that PTGBD is associated with a higher technical success rate than EUSGBD or ETGBD. PTGBD has been shown to be associated with high technical success rates of 98%–99%,26,29 but the results of comparisons of technical success between techniques have been contradictory. A meta-analysis of five studies published in 2019 showed no significant difference in the technical success rates of EUSGBD and PTGBD. 30 Similar to the results of several previous studies, the present study has shown that EUSGBD is associated with a higher technical success rate than ETGBD. Technical success was achieved with EUSGBD in 91.5%–100% of patients in previous studies, compared with 50%–100% for ETGBD. There are several possible explanations for this difference, such as obstruction of the cystic duct due to gallstones and the technical difficulty of endoscopic retrograde cholangiopancreatography. The Tokyo guidelines recommend the use of EUSGBD as a first-line method of drainage, especially in highly experienced hands. 32
The present meta-analysis has also shown that PTGBD, ETGBD, and EUSGBD are comparable with regard to adverse event and mortality rates. However, there are suggestions that EUSGBD may be preferable with regard to the prevalence of adverse events and that PTGBD may be preferable with regard to mortality rate. There are several possible explanations for these trends. The principal complications of PTGBD include obstruction or migration of the drain and infection around the drain, but these infrequently lead to death. In contrast, the postoperative complications of EUSGBD and ETGBD include perforation, bleeding, and pancreatitis, which are more likely to lead to death. The present analysis has demonstrated that EUSGBD is less likely to be associated with recurrent cholecystitis than PTGBD or ETGBD. The use of a wide metal stent improves drainage and allows the passage of stones, which reduces the frequency of recurrence of cholecystitis.
With regard to efficacy and safety, the present meta-analysis has shown that EUSGBD is preferable to either PTGBD or ETGBD. However, the heterogeneity of the constituent studies was high with respect to both clinical success rate and the prevalence of adverse events. The publication year, country, and the experience of the clinicians may have contributed to this heterogeneity.
This present study had several strengths, including that it was the first network meta-analysis to compare the efficacy and safety of PTGBD, ETGBD, and EUSGBD. In addition, it included several recent studies and did not feature significant local inconsistency. Nonetheless, this study also had several limitations. First, most of the included studies were retrospective and there was only one RCT. This could have resulted in selection and time bias. Second, the definition of the outcomes, including technical success and clinical success, varied among the included studies. Third, the samples in most of the included studies were small and there were few head-to-head comparisons of the three procedures.
Conclusions
Despite its limitations, the present network meta-analysis has shown that EUSGBD appears to be superior to PTGBD and ETGBD with regard to both safety and efficacy for the treatment of patients with acute cholecystitis who are at high surgical risk. However, high-quality head-to-head RCTs should be conducted to confirm these findings in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.