
Abstract
Background:
Impassable caustic esophageal strictures (CES) can be rendered passable through sophisticated dilatation techniques, hence avoiding the esophageal replacement surgery and its complications.
Patients and Method:
Patients with impassable CES who were presented to our hospital between January 2015 and April 2020 underwent a combined balloon and bougie dilatation. This technique aims at doing an initial partial dilatation of the proximal segment of the stricture, using a balloon catheter to pave the way for the endoscope to be advanced more distally. Therefore, a guide wire could be passed down to the stomach to complete the dilatation session using bougie dilators.
Results:
Seven patients out of 138 patients who underwent endoscopic dilatation for CES at the pediatric surgery department were enrolled in this study. Their ages ranged from 2.5 to 6 years. This technique was successful in 6 patients indicating technique reproducibility of 85.7%. These 6 patients continued their next dilatation sessions using bougie dilator only, whereas 4 patients were completely cured from dysphagia indicating technique efficiency of 57%, 1 is still on dilatation, and 1 patient had a resistant stricture. The dilatation through the proposed technique failed in 1 patient, who was referred for a replacement surgery.
Conclusion:
Combined dilatation is safe and effective to preserve the native esophagus in some difficult CES.
Introduction
Caustic esophageal strictures (CES) are regarded as a major health problem especially in the developing countries. Endoscopic dilatation is a fundamental treatment and it is successful in the majority of cases. 1 Both Savary-Gilliard and balloon dilatations are safely and effectively used for dilatations of benign esophageal strictures.2,3
In the current study center, the endoscopic bougie dilatation under fluoroscopic guidance is adopted as a standard technique for management of CES. Balloon dilatation, which is traditionally designed to treat patients with achalasia, is believed to be more suitable for localized postanastomotic strictures, rings, and webs. Moreover, Savary-Gilliard dilators are reusable, which reduces the cost of the repeated dilatation sessions. 4 Nonetheless, balloon dilatations still have some indications.
The inability to pass the guide wire in tortuous, long, or the multiple strictures represent a great challenge. Whereas retrograde dilatation through gastrostomy opening is a valid and safe option in these difficult cases. 5 Despite that, the guide wire may be trapped as well in some cases. Moreover, some patients may not have a pre-existing gastrostomy.
Materials and Methods
In this study, we aimed to assess the feasibility and the effectiveness of the combined balloon and bougies dilatation technique in management of esophageal strictures labeled as impassable and nondilatable strictures. This technique was used for patients who encountered a failed bougie dilatation because the guide wire could not be safely advanced through the stricture (Fig. 1). This study was approved by the institutional review board at pediatric surgery department, Ain Shams University.
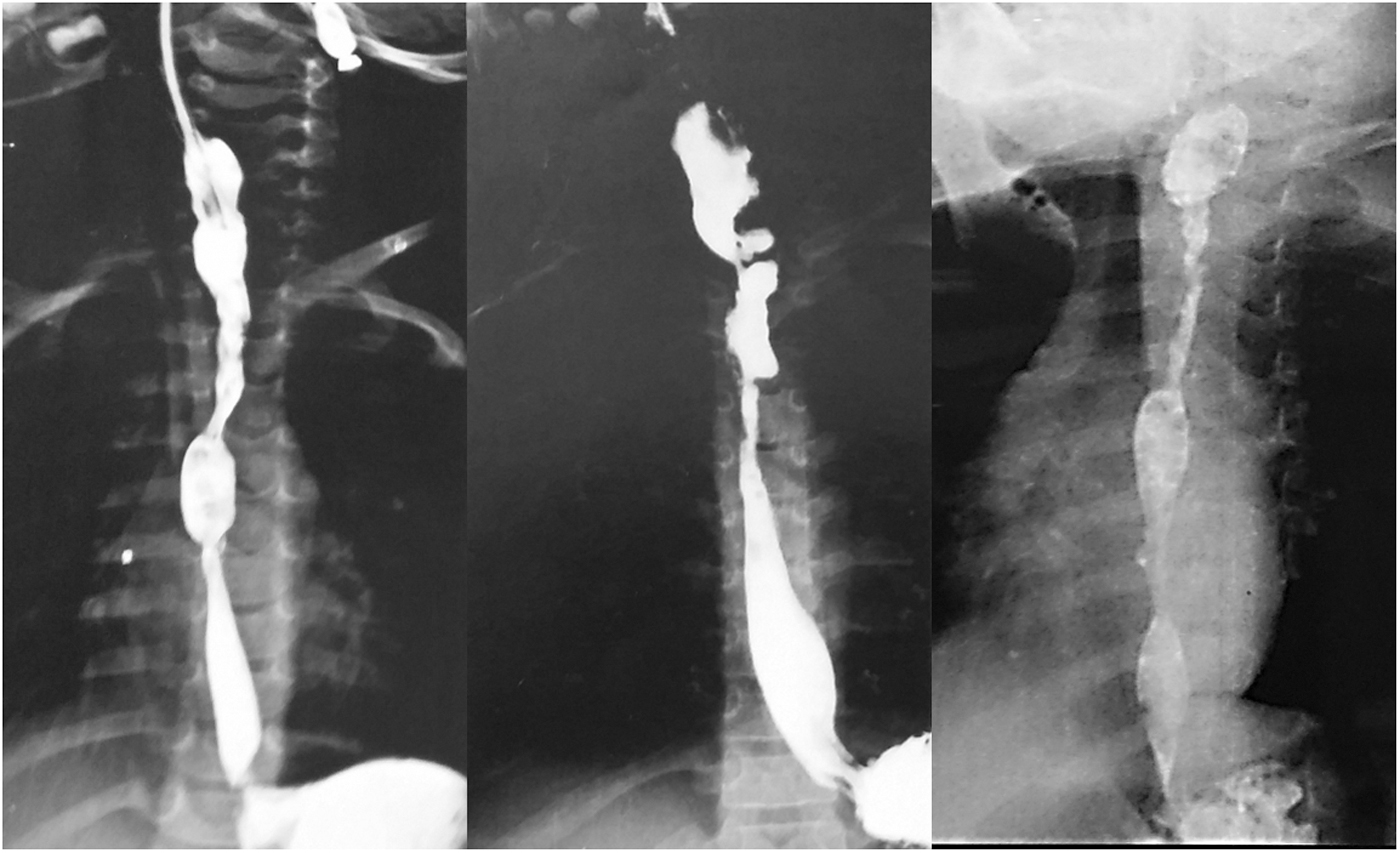
Contrast swallow studies of 3 patients with impassable multiple and/or tortious caustic esophageal strictures who were managed by the combined balloon and bougie dilatation.
Endoscopic technique
After the induction of general endotracheal anesthesia, a trial of antegrade endoscopic dilatation was first attempted. In cases where advancing the guide wire distally without resistance was unsuccessful, they were converted first to the retrograde approach if the patient has already preformed gastrostomy using the technique that was described in our previous publication. 5 In case of failed retrograde dilatation, as well as in case of patients without a gastrostomy, the combined balloon and bougie dilatation was tried. Those patients mostly had tortuous, angulated, long, or multiple strictures.
In such cases, the guide wire usually passes through the proximal segment of the stricture, then it gets stuck at a distal one. The mechanism of the technique is to perform an initial partial dilatation of the proximal segment of the stricture, using a balloon catheter to pave the way for the endoscope to be advanced quite more distally. Therefore, the guide wire is passed one more time through the distal segment of the stricture for bougie dilatation of the entire stricture length.
For this approach, the patient is kept in a supine position; a 9 mm flexible esophagoscope (Pentax® Europe GmbH EPM-3500, Hamburg, Germany) was introduced till the beginning of the stricture. A deflated balloon catheter (Hercules® Wilston-Cook Medical, Inc., Ireland), size no. 10 was passed through the side channel of the endoscope, and was lodged inside the proximal segment of the stricture under endoscopic guidance. The inflation of the balloon was done three times; each 3 minutes. Inflations were separated by 1 minute of deflation. After the withdrawal of balloon catheter, the endoscope was advanced more distally through the proximal segment and another trial to pass the guide wire to the stomach was attempted. If the guide wire passed smoothly and its location in the stomach was confirmed by fluoroscopy, a serial dilatation using Savary-Gilliard dilators® (Wilson-Cook Medical, Inc., Winston-Salem, NC, USA) under fluoroscopic guidance can be done after determining the appropriate size according to each case. The size of the child's thumb was used as a rough measure of the target dilator size. If any resistance was encountered while passing the guide wire, the procedure is aborted. Moreover, a routine postendoscopy chest X-ray was done to all cases to exclude iatrogenic esophageal perforation.
The dilated cases successfully continued their dilatation program with adjuvant topical mitomycin C application (1 mg/mL), starting from the subsequent sessions, to decrease the incidence of stricture recurrence. Mitomycin C was topically applied using the rigid esophagoscope as it was described in our previous publication. 6
Results
Between January 2015 and April 2020, 138 patients with CES were referred to our department for endoscopic dilatation. Whereas 122 patients were managed by traditional dilatation using antegrade bougie dilators, the guide wire failed to pass in 16 patients. Out of these 16 patients 11 had already a pre-existing gastrostomy, whereas the other 5 did not. A trial of retrograde dilatation was done for patients with gastrostomy, which was successful in 9 of them. Seven cases were enrolled in this series: 5 patients who did not have a pre-existing gastrostomy and had failed antegrade passage of the guide wire, and the 2 cases who had failed both antegrade and retrograde passage of the guide wire (Fig. 2). A trial of a combined balloon and bougies dilatation, as previously illustrated, was attempted in those 7 patients: 5 boys and 2 girls, whose ages ranged from 2.5 to 6 years. All of them had a CES with a history of accidental alkali ingestion.

A flowchart illustrating the patient's selection for the dilatation procedure.
This technique was successful to dilate 6 patients and failed in 1 patient. The reproducibility of the technique was 85.7%. These 6 patients continued their next dilatation sessions, with the antegrade manner, using bougie dilators only. This dilatation technique failed in 1 patient as well, and he had an esophageal replacement surgery “colon interposition.”
Among the successfully dilated patients, through this approach, 4 patients were completely cured from dysphagia, a cured case is considered when the patient is dysphagia free for at least 1 year after the last dilatation session; 1 patient is still on dilatation with marked improvement and 1 patient had a resistant stricture, thus he was referred for an esophageal replacement surgery (Fig. 3).
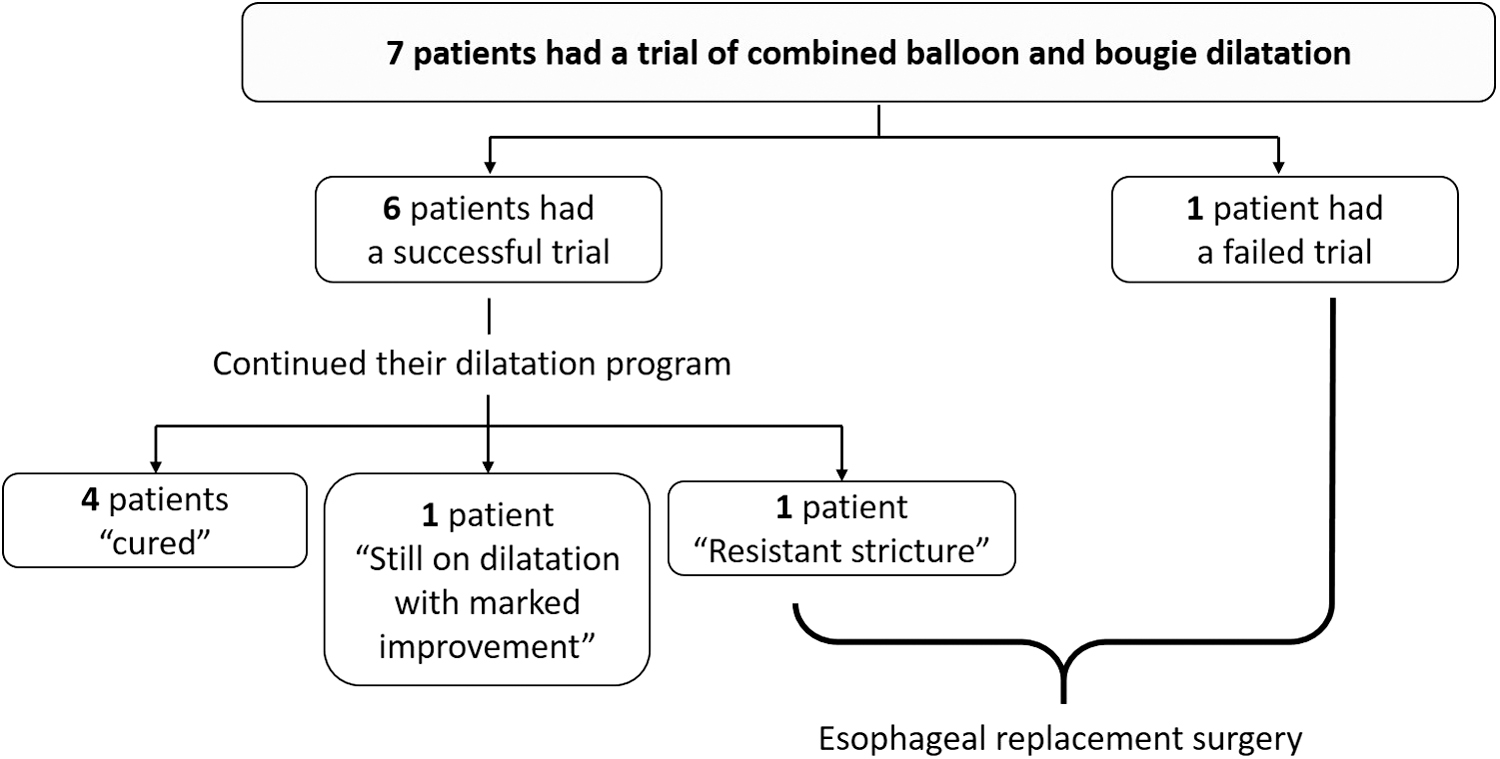
A flowchart illustrating the success of the combined balloon and bougie technique and the final outcome of the patient's dilatation program.
Eventually, 4 out of 7 participants were assisted to maintain their native esophagus. This means that the efficiency of this technique is estimated to be 57%. Besides, no esophageal perforations were encountered in this series.
Discussion
Caustic ingestion and its complications still represent a critical problem, especially in the developing countries, due to esophageal cicatrization, with variable degrees of stricture formation, which is regarded as the most common chronic sequelae. All the available modalities should be exhausted, to salvage the native esophagus as a result of the lack of the ideal substitute, and to avoid the drawbacks of esophageal replacement surgeries.1,7 Endoscopic dilatation of CES is usually preferred, if possible, over replacement surgery due to its safety and its ability to alleviate symptoms, in the majority of patients, with preservation of the native esophagus.8,9
Two types of dilators came into practice worldwide: bougie and balloon dilators. In the current study center, fluoroscopic-guided Savary-Gilliard dilators is the preferred approach for the endoscopic dilatation of CES. These dilators exert an axial force to dilate the stricture and permit easily controlled graded dilatation of both short and long passable strictures. Considering their reusability, the cost is low, compared with balloon dilatation. Savary-Gilliard dilators were proven as safe and effective maneuver since implementing the current protocol.1,10
Catheters for balloon dilatation were primarily used for the dilatation of cardiac achalasia cases. In 1981, London et al. reported two cases with severe esophageal strictures that could be successfully dilated by Grüntzig Balloon catheters. 11 In 1984, Ball et al. reported the first successful dilatation of an esophageal stricture in a child through balloon under fluoroscopic guidance. 12 Since then, many reports suggested the use of balloon; either fluoroscopic or endoscopic guided, for the dilatation of esophageal strictures in children.13–16 Balloon dilators are characterized by the ability to apply a precise radial pressure, over a localized stricture. 16 Currently the choice of the dilatation technique depends on the operator's preference and experience. There is no consensus in the literature; neither to favor balloons over bougies nor vice versa. A recent meta-analysis studied the difference between bougies and balloon dilatation, and it was found out that there is no difference between both modalities, regarding symptomatic relief, recurrence of symptoms, and complications rate. Only patients who underwent balloon dilation express less severe postprocedural pain. 2
Long tortuous strictures are problematic as they are very difficult to dilate. Some authors prefer balloon dilatation to treat multiple CES. 17 Some of these strictures may require a combination of the two different types of dilators in the same session. In 1990, Shemesh and Czerniak reported 4 tortuous cervical strictures and multiple closely placed strictures that were managed by the initial use of balloon followed by Savary dilators. 18 They used the same technique that was initially described by Webb in 1988. 19
An alternative approach of impassable stricture is the retrograde dilatation that succeeded in 82% of patients. 5 Multiple angulations could hinder the safe passage of the guide wire, therefore safe dilatation, through Savary-Gilliard dilatation, could not be performed, either by antegrade or retrograde manner. Those patients were previously referred for surgical replacement without being listed for dilatation program.
The idea of the current technique is to employ the balloon catheter to perform partial dilatation, of the proximal segment of the stricture, to a sufficient degree that allows a better visualization of the distal segment, therefore the guide wire could be safely advanced to the stomach to continue the dilatation session by Savary-Gilliard dilators. In this technique, the balloon dilatation was performed under endoscopic guidance, rather than a fluoroscopic guidance that allowed direct visualization during the placement of the catheter, within the proximal segment of the stricture.
In our center, the view shifted concerning the long tortuous caustic, since the topical use of mitomycin C. Fifteen years ago, cases with long tortuous strictures were directly referred to a replacement surgery. Long tortuous strictures were considered as a relative contraindication for the endoscopic management trial. 1 After adding topical mitomycin C to the dilatation protocol, long, tortuous, and resistant strictures could be managed, with endoscopic dilatation, achieving good results.10,20
The impassable strictures were successfully turned to passable, through the suggested combination of balloon and Savary-Gilliard dilators, and accordingly dilatable strictures in 6 patients (85.7%). Nevertheless, one of the enrolled patients is still under dilatation sessions. The use of balloon catheters to pave the way for further Savary-Gilliard dilatation sessions, with the aid of topical mitomycin C, was effective to preserve the native esophagus in 4 patients (57%).
No complications were faced during the management of these patients. It is worth mentioning that the prevention of the accidental ingestion of caustic substances is highly important.
Conclusion
Combined balloon and bougie dilatation technique is reproducible and effective in some children with impassable esophageal stricture to give them a chance for salvage of their native esophagus. Pediatric surgeons and endoscopists have to be aware of multiple dilatation modalities, technical tricks and maneuvers, when facing CES, attempting to preserve the native esophagus before referring to the esophageal replacement surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.