
Abstract
Background:
Patients, surgeons, and payers are interested in reducing hospital length of stay. Outpatient laparoscopic fundoplication (LF) can be done safely and cost effectively. There is low acceptance of this practice due to fear of readmission and patient dissatisfaction. Our aim was to identify factors predicting failure of same-day discharge after LF.
Methods and Procedures:
We simulated an outpatient setting for patients who underwent LF from 2017 to 2018 and collected the data prospectively. A perioperative pain and nausea protocol was utilized. Postoperatively, patients were given a liquid diet and oral medications, observed overnight, and then discharged after standard criteria were met. Failure was defined by the need for physician intervention after 3 hours or failure to discharge. Univariate and multivariable logistic regression analyses were performed assessing factors associated with failure. Two-sample t-test and chi-squared tests were used for significance.
Results:
Ninety-eight patients were included. Twenty patients failed, primarily due to the need for intravenous medications. Seven were discharged on postoperative day 1 but required physician intervention after 3 hours. Thirteen patients stayed >23 hours. Two patients were readmitted within 1 week of discharge. There was one acute recurrence, requiring reoperation, and one conversion to laparotomy. We found no statistically significant patient risk factor, comorbidity, or perioperative variable that could reliably predict failure of same-day discharge.
Conclusion:
This study suggests that same-day discharge after LF is safe and feasible. However, 20% of patients will unpredictably fail to meet discharge criteria.
Introduction
Laparoscopic Fundoplication (LF) is the gold standard antireflux procedure for the surgical treatment of gastroesophageal reflux disease (GERD). It is a safe and effective procedure with a low rate of complications, especially in the hands of experienced surgeons. 1 Since its inception in 1991, the minimally invasive approach has allowed for a shorter hospital stay and enhanced recovery compared with the traditional open technique.2,3 Many studies have demonstrated that LF can be safely performed in an ambulatory surgery center or hospital-based outpatient surgery ward, resulting in significant cost savings.4–10 This improvement has been so dramatic that now some insurance companies will not approve an inpatient postoperative stay. Despite the evidence, this practice remains underutilized due to fear of increased readmission rates, patient dissatisfaction, and potential delayed presentation of complications. These concerns arise from reports of up to 20% of patients failing same-day discharge after LF, with up to 11% requiring a nonscheduled office visit, and up to 12% needing readmission to the hospital. 7 Studies are yet to identify risk factors that reliably predict which patients are unsuitable for same-day discharge after LF. Most of the literature thus far is focused on cost, patient satisfaction, and the safety and efficacy of same-day discharge after LF, and not on the predictors of those patients who will require a longer hospital stay.
In this controlled simulated experience, we were able to safely monitor all patients in an outpatient setting and gather data prospectively, then directly compare the success and failure groups for any notable differences. We theorized that these differences would be better recognized at our high-volume foregut center. The hypothesis of this study is that otherwise healthy patients with typical GERD symptoms, reasonable esophageal motility, and only small associated hiatal hernias can be safely treated on an outpatient basis. We aimed to identify factors predicting failure of same-day discharge after LF, and so, surgeons may better stratify patients into traditional hospital stay and outpatient groups.
Materials and Methods
In this IRB-approved prospective cohort study, patients with objectively confirmed GERD underwent routine elective LF in a large-volume hospital-based foregut practice from 2017 to 2018. Both partial and complete fundoplications were performed with routine type I hiatal hernia repair. Inclusion criteria were patient age between 18 and 85 years and the ability to provide informed consent. Exclusion criteria consisted of emergent surgeries or complex foregut surgery, including paraesophageal hernia repair. Pertinent comorbidities and operative variables previously documented to contribute to a prolonged or difficult postoperative course (NSQIP Surgical Risk Calculator) were recorded, as outlined in Table 1. 11 Same-day discharge was defined as any discharge that could have been completed within the same calendar day of the surgery, as per institution-specific discharge criteria and protocol. Morning surgery was defined as an incision time before 12:00. The primary objective was to observe LF patients in a simulated ambulatory surgical setting during an overnight hospital admission, while formally collecting data and measuring outcomes.
Variables Assessed to Identify Which Patients May Fail Same-Day Discharge After Laparoscopic Fundoplication
ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, chronic obstructive pulmonary disease; EBL, estimated blood loss.
All patients underwent a standardized perioperative pain and nausea protocol, comprising one 600 mg dose of gabapentin preoperatively, followed by one 8 mg dose of intravenous (IV) dexamethasone given immediately after induction of anesthesia, and 8 mg of IV ondansetron administered 20 minutes before the end of the procedure. No routine surgical drains were placed, and no routine postoperative imaging was obtained. Postoperatively, patients were kept nil per os (NPO) for 3 hours, after which the IV fluids were discontinued, and they were given a liquid diet with oral medications only, to simulate the outpatient setting. Patients were observed overnight with standing orders for discharge when standard same-day discharge criteria were met the following morning. Nurses were instructed to call the surgeon for orders for additional IV medications or fluids as requested. All additional therapies were recorded in the database along with indication and time of occurrence. Criteria for discharge included the following: pain and nausea controlled with oral medication, tolerance of a liquid diet, successful wean of supplemental oxygen, successful urination, and normal vital signs. Patients were educated and consented for the protocol during their preoperative office consultation. Prescriptions and discharge instructions were prepared in advance. There was no routine physician visit or rounding before discharge unless discharge criteria were not met or the nursing staff raised a safety concern. Failure during this period was defined by the need for postoperative physician involvement after 3 hours, such as the need for IV medication, further workup, additional intervention, or the development of abnormal vital signs. Results were tabulated, and both univariate and multivariable logistic regression analyses were performed assessing factors associated with failure. Two-sample t-test and chi-squared tests were used to test for significance.
Results
Our analysis demonstrated no statistically significant patient risk factor, comorbidity, or perioperative variable that could reliably predict failure of same-day discharge. The major findings from the study are illustrated in Figure 1. The reasons that patients failed to be discharged the same day after LF are described in Figure 2, with the most common reason being the need for IV medications. Two patients were readmitted, on postoperative days 4 and 6, resulting in a readmission rate of 2%. The number of potential risk factors from Table 1 was similar between groups (3.25 failures versus 2.95 successes, median 4 versus 2.5, respectively). Univariate and multivariable logistic regression analyses of each cohort's patient demographics, comorbidities, and perioperative variables are shown in Tables 2–4. All failures were those younger than 75 years, with no reported smoking, diabetes, steroid use, or cardiac events. There was a trend for more preoperative narcotic use in the failure group, as well as more female patients, although these findings were not statistically significant. Of the 20% of patients who failed same-day discharge, the average time to failure was 4 hours and 28 minutes postoperatively (standard deviation [SD] ±1 hour and 6 minutes), and the last medical provider intervention occurred on an average of 34 hours and 13 minutes postoperatively (SD ±26 hours and 10 minutes).
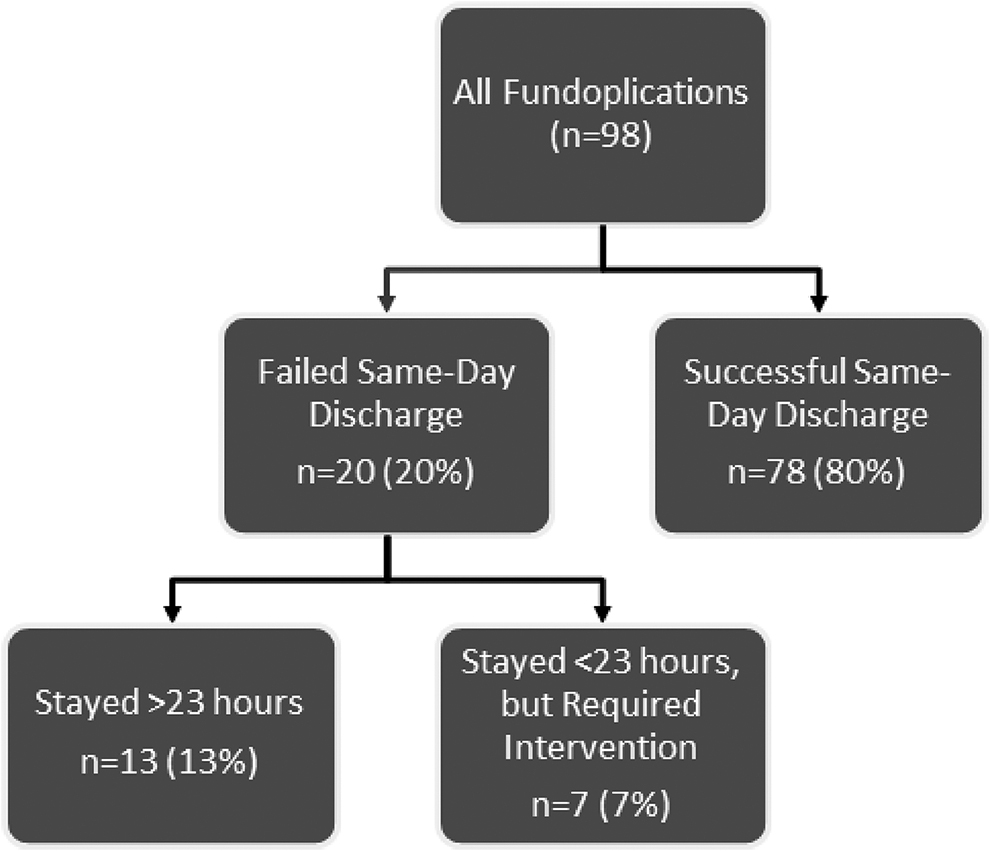
Schematic of results demonstrating rate of successful same-day discharge after laparoscopic fundoplication.

Causes of failure for same-day discharge after laparoscopic fundoplication. IV, intravenous.
Patient Demographics
ASA, American Society of Anesthesiologists; BMI, body mass index; F, female; M, male; SD, standard deviation.
Preoperative Comorbidities and Risk Factors
COPD, chronic obstructive pulmonary disease.
Operative Variables
SD, standard deviation.
Discussion
Considering the potential benefits of converting traditional inpatient surgeries to an ambulatory setting, we were hoping to provide clinicians with an evidence-based tool to predict which patients could be reliably scheduled for an ambulatory surgery center and be safely discharged after LF. In this controlled simulated experience, we were able to monitor clinical outcomes in the safety of the hospital while attempting to identify any potential risk factors for a prolonged hospital course or readmission. We found that 80% of them could have been successfully discharged within a few hours of surgery, similar to other published reports. However, 20% of patients required an inpatient level of care precluding a safe early discharge, although we were unable to identify any specific risk factors to predict who these patients were.
Surgeons are slowly growing more accustomed to performing more advanced laparoscopic procedures as a same-day case. This paradigm shift was apparent in 2018 when the Centers for Medicare and Medicaid Services, alongside the American College of Surgeons, removed laparoscopic paraesophageal hernia repair with mesh and fundoplication from the inpatient-only list. To successfully change the utilization pattern for a certain surgical procedure, it is essential for the surgeon to understand the differences between inpatient and ambulatory surgery criteria, and properly designate patients for each disposition. Ambulatory surgery centers typically cannot provide services that, under ordinary circumstances, would be expected to exceed 24 hours. The terms same-day, outpatient, and ambulatory are often used interchangeably, which can lead to confusion. For instance, a same-day surgery, which is suitable for ambulatory surgery centers without overnight capabilities, should be differentiated from outpatient or ambulatory surgery, which can also apply to 23-hour overnight recovery units that can provide outpatient services. These concepts are separate from a patient's designated hospital status, which is important for insurance coverage, reimbursement, and qualifying for rehabilitation or home health services, but was not the primary focus of this article. The goal was to attempt to predict which patients can be safely discharged from our facility after a reasonable postoperative observation period following an LF.
A thorough understanding of the surgical literature is also paramount when deciding whether to perform LF as a same-day operation. To better understand the applicability of same-day fundoplication, many researchers have attempted to compare this practice with other more common same-day procedures such as laparoscopic cholecystectomy or laparoscopic sleeve gastrectomy, for which formal Enhanced Recovery after Surgery protocols have been developed. A 2013 systematic review of randomized-controlled trials assessing the ability to perform laparoscopic cholecystectomy as a same-day surgery found no significant difference in the rate of readmission (0.5% versus 2.1%), or failure to discharge as planned (19.3% versus 20.1%), between patients who were sent home the same-day versus those staying overnight, respectively. 12 By comparison, the success rate for same-day discharge after laparoscopic sleeve gastrectomy is between 92% and 100%, and a recent review of the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database revealed the readmission rate following same-day laparoscopic sleeve gastrectomy to be 2.14%.13–15 These numbers are similar to those reported for same-day LF in a recent review of 13 cohort studies, which showed the overall success rate for planned same-day discharge after LF to be 93%, with a readmission rate of 5%. 8 However, in a prospective cohort study directly comparing same-day LF with same-day laparoscopic cholecystectomy, 32% of the LF patients came back to the emergency room and 9% were readmitted, compared with 12.5% and 6% for the cholecystectomy group, respectively. In a postoperative telephone survey, nearly twice as many of the fundoplication patients would have preferred a short hospital stay, when compared with the cholecystectomy group (66.7% versus 30.9%). 5 These findings raise the question as to whether there is value in attempting same-day discharge after LF, at the expense of patient dissatisfaction and/or increase health care spending on the patients who return to the hospital.
Fortunately, there have been several studies investigating these concerns. Similar to this study, Gronnier et al. discharged 101 patients on the same day of surgery after LF and matched these patients to historical inpatient stays, and found similar morbidity and mortality. 4 Interestingly, they reported a readmission rate of 7.9% for the same-day cases versus 0% for the overnight patients; however, the overall health care costs for the inpatient group were nearly three times that of the same-day discharge group. 4 Moreover, there have now been many large systematic reviews of patients undergoing same-day LF that report high postoperative patient satisfaction scores.7,8 A prospective French study of 40 patients undergoing same-day LF suggested that a standardized preoperative education program on ambulatory surgery may be helpful in setting the patients' expectations, and in improving acceptability of this practice. 16 These combined results suggest that patient dissatisfaction should no longer be considered a major obstacle in deciding whether to schedule a patient for same-day LF.
Although same-day LF has been found to be safe and effective, the surgical literature is yet to consistently highlight those factors that lead to failure. A retrospective cohort study from the United Kingdom attempted to address this issue, although the authors were unable to delineate any patient-specific or operative variables that reliably predicted failure to discharge the same day after LF. 9 Notably, American Society of Anaesthesiologists (ASA) grade >2, revisional surgery, and case end time after 13:00 predicted hospital readmission. Another 2012 retrospective study from Ireland corroborated these results, and found that an ASA score >2 and advanced age correlated with both failure to discharge and hospital readmission after planned same-day LF. 17 Our study, combined with the previously mentioned investigations, has likely not provided enough evidence to change the majority of clinical practice, and implementation of same-day LF will likely remain slow among most hospitals and providers.
Our failure to discharge rate of 20% is higher than the reported average after same-day LF of 7%. 8 It is thought that this could possibly be due to patients being more willing to ask for IV intervention for symptom control while in the hospital setting than they otherwise would while recovering at home. The design of the study made these services more readily available, and the patients did not have to travel back to the facility for triage or registration, making this inherent bias a limitation of our study. In addition, the average time to discharge for same-day LF has been reported to be ∼6.5 hours. 6 Therefore, if our protocol allowed patients to receive IV medications beyond the 3-hour time period, and made them NPO at 6.5 hours, for instance, the success rate would likely improve. In fact, in this scenario, 15% (n = 3) of our failure patients would have been moved to the success group. This certainly is a consideration for future prospective studies.
Conclusion
This study suggests that while same-day discharge after LF remains safe and feasible in 80% of patients, there is a 20% rate of failure that cannot be reliably predicted based on patient factors or perioperative data. Readmission rates are similar to other common day-case laparoscopic procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.