
Abstract
Background:
To investigate the application value of 4K high definition (HD) in laparoscopic gastrectomy by comparing the short-term outcomes and subjective perception with three-dimensional (3D) and HD vision systems.
Materials and Methods:
A retrospective study was conducted between September 2018 and February 2019; a total of 87 patients who underwent laparoscopic gastrectomy were enrolled and divided into three groups in terms of different type of vision system used for surgery: 4K, 3D, and HD. Demographic and clinicopathological data as well as short-term outcomes were collected and analyzed. A questionnaire survey was completed by the team of surgeons to evaluate the subjective perception of different vision systems.
Results:
There was no significant difference in gender, body mass index, age, American Society of Anesthesiologists (ASA) score and history of abdominal surgery, tumor location as well as type of operation, and anastomosis between the 4K, 3D, and HD groups. All patients underwent laparoscopic gastrectomy without conversion to laparotomy. There was no difference between the three groups regarding operation time (4K versus 3D versus two-dimensional (2D), 183.60 ± 52.5 versus 189.69 ± 69.87 versus 211.00 0 ± 49.33, P = .145) and estimated blood loss (4K versus 3D versus 2D, 123.60 ± 119.51 versus 150.62 ± 105.46 versus 129.00 ± 103.57, P = .602), no difference was found in time to first flatus and postoperative hospital stay between the three groups. No significant difference was found in postoperative complications between the three groups. As for pathological results, there was no difference in tumor size and tumor-node-metastasis (TNM) stage. In 4K group, the number of lymph node harvested was 32.60 ± 10.28, no difference was found compared with that of 3D (29.81 ± 8.94) and HD groups (27.69 ± 10.96). The score of group 3D was the lowest concerning asthenopia and motion sickness. On the contrary, 3D group achieved the highest score in topographical orientation and depth description. 4K group was graded the highest in terms of control co-ordination of visual angle, visual acuity, radiance, resolution ratio and frames, and refresh rate. HD group was graded significantly lower in sense of control compared with that of 4K and 3D group. No significant difference was found in color resolution and contrast.
Conclusions:
In conclusion, the short-term effect of 4K HD laparoscopic system is comparable with that of HD and 3D laparoscopy, whereas 4K could reduce adverse effect than traditional instrument and improve quality of surgery. The Clinical Trial Registration number is NCT01441336.
Introduction
Laparoscopic gastrectomy was first introduced by Kitano in 1994, 1 and studies have demonstrated the advantages of laparoscopic technique in terms of reduced pain, faster recovery as well as cosmetic appearance ever since.2–4 In addition to technique aspect, development of surgical instrument also plays a vital role in the progression of surgery. High-definition (HD)/two-dimensional (2D) is still the most commonly used system nowadays, whereas three-dimensional (3D) laparoscopic system has been reported to have several merits over 2D laparoscopy.5–7 A more advanced monitor with 4K UHD (ultrahigh definition; 3840 × 2160 pixels) was introduced to laparoscopic surgery recently; however, the application value of 4K laparoscopic system in laparoscopic gastrectomy remains unclear. This study was conducted with the aim to verify the short-term effect of 4K HD system in laparoscopic gastrectomy.
Materials and Methods
Patients
This was an Institutional Review Board-approved retrospective study; from September 2018 to February 2019, a total number of 87 patients diagnosed with gastric cancer underwent laparoscopic radical gastrectomy at Shanghai Minimally Invasive Surgery Center, Shanghai Ruijin Hospital affiliated to Shanghai Jiaotong University, School of Medicine. Exclusion criteria includes patients with pathology other than adenocarcinoma, patients with American Society of Anesthesiologists (ASA) score >3, patients with synchronal distant metastasis, patients <20 or >80 years. All patients enrolled have informed consents, and were divided into three groups in terms of different laparoscopic vision system used during surgery: Group 4K (n = 25), Group 3D (n = 32), and Group HD (n = 30).
Variables
Demographic and clinicopathological characteristics were collected, including age, gender, body mass index (BMI), ASA score, tumor location, and history of abdominal surgery. Surgical and pathological data were also recorded and analyzed, including operative and anastomotic method, operation time, estimated blood loss (EBL), conversion to laparotomy, time to first flatus, postoperative hospital stay, lymph node harvest, and tumor-node-metastasis (TNM) stage based on the American Joint Committee on Cancer (AJCC) Staging Manual 8th edition, total morbidity, and mortality.
Subjective perception was evaluated by questionnaire survey, content of which includes asthenopia, motion sickness, topographical orientation, control co-ordination of visual angle, visual acuity, radiance, resolution ratio, depth description, color resolution, sense of controls, optimum viewing distance, frames and refresh rate, and contrast. Each item was scored with 5-Grade criteria: Grade 1: unable to operate; Grade 2: severe impact on operation; Grade 3: moderate impact on operation; Grade 4: mild impact on operation; Grade 5: no impact on operation.
Optimum viewing distance was defined as following: Grade 1: <50 cm; Grade 2: 50–100 cm; Grade 3: 100–150 cm; Grade 4: 150–200 cm; Grade 5: >200 cm.
Questionnaires were distributed and completed by surgeons, first assistants, and endoscopists, respectively, right after surgery, then all data were collected and analyzed.
Statistical analysis
IBM SPSS 25.0 statistical software (SPSS, Inc., Chicago, IL) was used for statistical analysis. Variables was expressed as mean ± standard deviations and compared using one-way analysis of variance (ANOVA) test or Kruskal–Wallis test in terms of variance homogeneity. P values <.05 was considered statistically significant.
Results
A total of 87 patients were enrolled in this study, general data were summarized in Table 1. There was no significant difference in gender, BMI, age, ASA score and history of abdominal surgery, tumor location as well as type of operation, and anastomosis between the 4K, 3D, and HD groups.
Demographic and Clinicopathological Characteristics
3D, three-dimensional; ASA, American Society of Anesthesiologists; BMI, body mass index; HD, high-definition; LATG, laparoscopy-assisted total gastrectomy; LDTG, laterodorsal tegmental nucleus.
All patients underwent laparoscopic gastrectomy without conversion to laparotomy. Surgical and pathological results are demonstrated in Table 2. There were no differences between the three groups regarding operation time (4K versus 3D versus 2D, 183.60 ± 52.5 versus 189.69 ± 69.87 versus 211.00 0 ± 49.33) and EBL (4K versus 3D versus 2D, 123.60 ± 119.51 versus 150.62 ± 105.46 versus 129.00 ± 103.57); meanwhile no difference was found in time to first flatus and postoperative hospital stay between the three groups. Postoperative complications were observed in four cases (16.0%) in 4K group, six cases (18.75%) in 3D group, and eight cases (26.7%) in HD group, respectively. One case of postoperative bleeding occurred in 4K group, who was treated conservatively, HD group also has one case of postoperative bleeding and another laparoscopic exploration had to be conducted for this patient. There was one case of duodenal stump leakage in 3D group and two cases in HD group, who received conservative treatment. One patient in HD group underwent anastomotic leakage, who was treated successfully with continuous irrigation. No statistical difference was found in postoperative complications between the three groups. As for pathological results, there was no difference in tumor size and TNM stage. In 4K group, the number of lymph node harvested was 32.60 ± 10.28, no difference was found compared with that of 3D (29.81 ± 8.94) and HD groups (27.69 ± 10.96).
Surgical and Pathological Outcomes
3D, three-dimensional; EBL, estimated blood loss; HD, high-definition; TNM, tumor-node-metastasis.
Subjective perception results are summarized and compared in Table 3. The score of group 3D was the lowest concerning asthenopia and motion sickness. On the contrary, 3D group achieved the highest score in topographical orientation and depth description. 4K group was graded the highest in terms of control co-ordination of visual angle, visual acuity, radiance, resolution ratio and frames, and refresh rate. HD group was graded significantly lower in sense of control compared with that of 4K and 3D group. No significant difference was found in color resolution and contrast.
Subjective Perception Score
3D, three-dimensional; HD, high-definition.
Discussion
In recent years, laparoscopic gastrectomy was more extensively accepted by institutions across the world, with indication expanding from early-stage to advanced gastric cancer.8–10 HD system was still the mainstream vision system used in clinic; however, the downsides of which were quite clear: lack of perception and limiting of resolution. The introduction of 3D laparoscopy was believed to overcome the shortcomings of HD laparoscopy. In previous literature, 3D was reported to show favorable results over HD both in laparoscopic simulation tasks and actual surgery.6,7 However, 3D vision system has not been as widely applied as HD, mainly because of the defects concerning wearing additional eyeglasses, dizziness, eye fatigue, even nausea or vomiting, and a long-time surgery such as gastrectomy is more likely to cause such side effects for surgeons.11,12 4K technique has been used commonly in television and computer monitors, and recently introduced into laparoscopic surgery.
Abdelrahman et al. 11 compared the surgical performance under HD, 3D, and 4K vision system in simulation tasks in their study, the results of which indicated that candidates from 4K and 3D groups could complete tasks in shorter performance time, with fewer errors and lesser number of repetitions. Moreover, 4K vision system improved candidates' performance in complex tasks, by significantly reducing number of operative errors compared with 3D and HD groups. In this study, despite that no difference was found in operation time, those in 3D and 4K groups were shorter than that of HD group. In addition, no significant difference was found in terms of EBL, recovery of bowel movement, postoperative hospital stay, and complications between the three groups, the results illustrated the safety and feasibility of 4K vision system.
4K vision system has an ultrahigh resolution four times as HD, which enabled it to present color display much closer to naked eye and improve the ability of recognition and detection of anatomical details such as nerves, membranes, and vessels or lymphatic tube with diameter <1 mm. In this study, we summarized the merits based on our experience using 4K vision system in laparoscopic gastrectomy: (1) in the step of dissection of NO.6 lymph node, pancreas tissue is often confused with adipose tissue and injured mistakenly, especially in patients with high BMI, which could be identified more accurately under 4K vision system, thus incidence of potential pancreas injury and postoperative pancreas fistula could be reduced. 4K vision system has better performance in resolution ratio and color resolution, as shown from the results of subjective perception, which could reveal the distinct color difference between pancreas and adipose tissue. (2) Lymph node was easier to be identified in the monitor with high resolution (Fig. 1), facilitating the radical clearance of lymph node. Despite that the total number of harvested lymph node showed no significant difference between the three groups, the number in 4K group was the highest. (3) 4K vision system could help surgeons dissect along the anatomical membrane and stay in the correct plane, the effect was significant when dissecting NO.11p lymph node (nodes along the proximal splenetic artery), the Gerota's fascia could be recognized precisely and ensure the border of dissection in the suprapancreatic space. (4) Intraoperative bleeding is commonly seen in gastrectomy and capillary bleeding is sometimes troublesome, due to a sudden loss of clear view. The reproduction of natural color and expanded horizon could help surgeons locate the bleeding site rapidly and precisely. (5) During the utilization of 4K vision system, we found that despite the two-dimensional nature, it could simplify complex operations such as intracorporeal suturing or lymphadenectomy in narrow space.
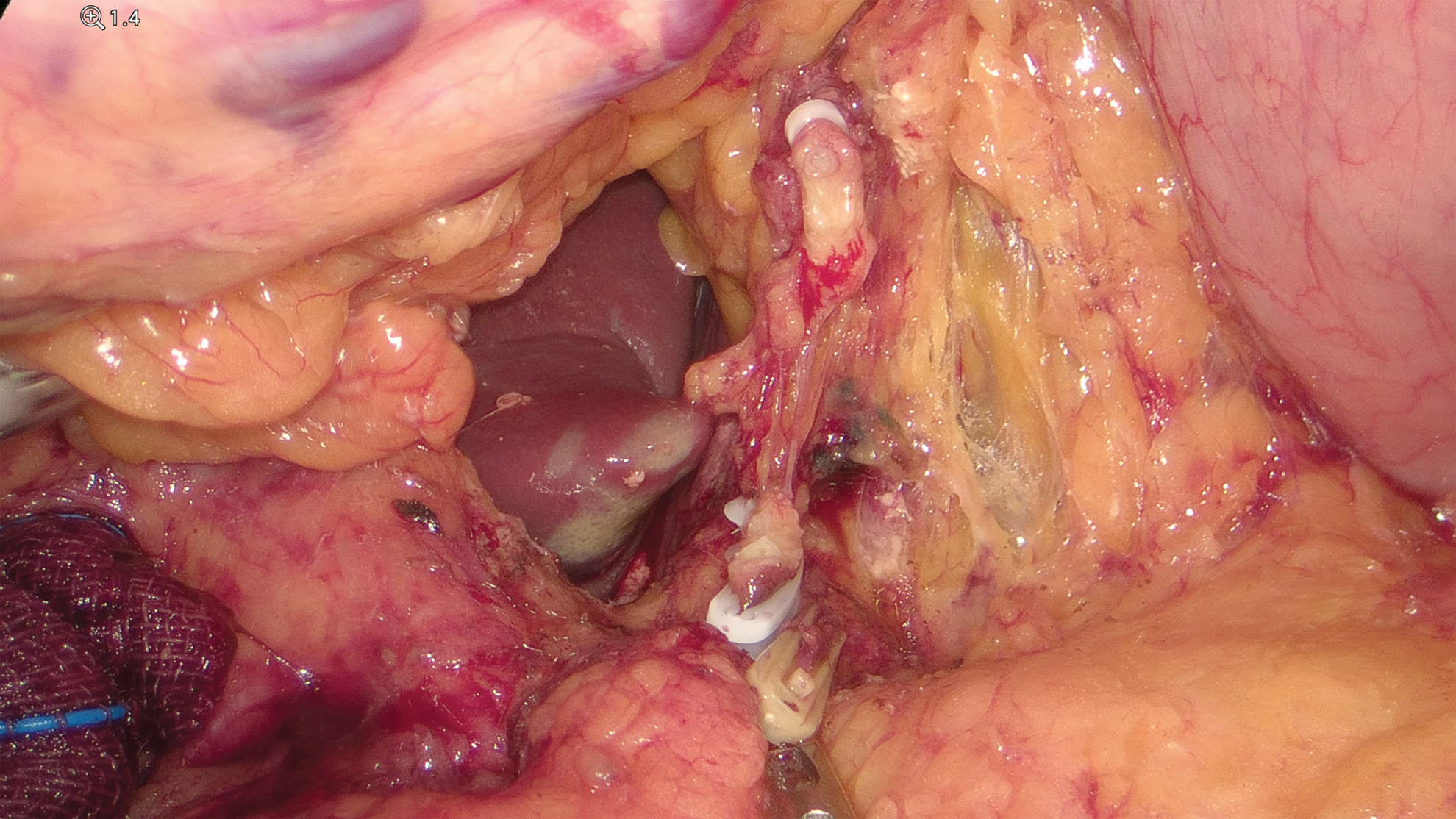
Lymph node shown in 4K laparoscopy. Color images are available online.
Same results were illustrated in Abdelrahman's study, 11 4K group had significantly less errors than the 3D group regarding the task of intracorporeal suturing. Harada et al. 13 also discovered that in complex tasks (knotting thread and suture in narrow space), the performance of 4K group was not inferior to that of 3D group. It could be explained that in 2D condition, depth perception was achieved by the contrast between the target and surrounding objects. Subjective perception questionnaire survey further indicated that 3D vision system was more favorable in terms of topographical orientation and depth perception, whereas 4K vision system achieved significantly higher score in major items in the questionnaire. We assume that 4K laparoscopy could make up the inadequate depth description by enhancing the clarity of surrounding contrast. In addition, the performance in asthenopia and motion sickness in 4K group was found to be much better than 3D group, which illustrated that 4K vision system was more comfortable and acceptable for surgeons.
Limitations exist in our study. It was a retrospective study conducted in one single center. A well-designed prospective randomized controlled trial may be needed to further evaluate the value of 4K laparoscopy.
In conclusion, the short-term effect of 4K HD laparoscopic system is comparable with that of HD and 3D laparoscopy, whereas 4K could reduce adverse effect than traditional instrument and improve quality of surgery.
Footnotes
Disclosure Statement
We declare that we have no conflict of interest in the authorship or publication of this contribution. No competing financial interests exist.
Funding Information
This study was funded by Shanghai Jiao Tong University Science and Innovation Fund (YG2019QNB24), and 3-Year Action Plan for Promoting Clinical Skills and Clinical Innovation in Municipal Hospitals, Shanghai Shen Kang Hospital Development Center Clinical Research Plan (SHDC2020CR3034B).*