
Abstract
Background:
Laparoscopic Nissen fundoplication is the gold standard antireflux procedure in pediatric age group. Intrathoracic migration of the fundic wrap is a common cause failure, leading to recurrence of gastroesophageal reflux disease (GERD) symptoms.
Objectives:
To investigate the impact of wrap-crural fixation and minimal esophageal dissection in prevention of wrap transmigration after laparoscopic Nissen fundoplication in children.
Methods:
Prospective randomized study of 46 pediatric patients with refractory GERD who underwent laparoscopic Nissen fundoplication divided into two equal groups. In Group A, wrap crural fixation was done, whereas in group B no fixation was done. Minimal esophageal dissection with preservation of the phrenoesophageal ligament was done in both groups. Approval of the Ethics Committee of our Faculty was obtained.
Results:
There was no difference between both groups regarding operative time, intraoperative complications, or length of hospital stay. Two patients in group B without wrap fixation suffered recurrence of GERD symptoms. On contrast study, they both showed intrathoracic wrap migration. One of them was reoperated. Whereas in group A, no recurrence of symptoms and no wrap transmigration were noticed in follow-up.
Conclusion:
In laparoscopic Nissen fundoplication, with minimal esophageal dissection and preservation of the phrenoesophageal ligament, there is no additional benefit from wrap-crural fixation in prevention of wrap transmigration.
Introduction
Failure after fundoplication is difficult to define due to discrepancy between patient-perceived symptoms and results of objective investigations. It has been noted that only 29.3%–39% of patients with persistent symptoms after fundoplication have an abnormal 24-hour pH study, 1 whereas 11.9% of asymptomatic patients have pathological scores. 2 Clinically, fundoplication failures include the recurrence of gastroesophageal reflux disease (GERD) symptoms or the development of new symptoms that did not exist preoperatively. Recurrent GERD [60%] and dysphagia [30%] are the most frequent symptoms of failure. 3
Fundoplication failures are classified into three categories based on endoscopic, radiological, and operative findings. Type 1A; herniation of the fundoplication into the chest reported in 30%–80% of cases, type 1B; slipped Nissen fundoplication occurs in 15%–30% of cases, type II failures; posterior paraesophageal hernia accounted for 23% of redo operations in one series and type III failure occurs as a result of malposition of the wrap at the initial operation, accounting for about 10% of failures.4,5
Postoperative wrap transmigration [Type IA] into the chest is the most common major complication of laparoscopic fundoplication. Herniation is usually induced by an inadequate crural closure and/or excessive traction on the gastroesophageal junction and an unrecognized short esophagus. Repair under tension is probably the main cause of failure.6–8
To prevent wrap herniation, Horgan et al. recommended wrap fixation to the esophagus and to the undersurface of crura, 9 whereas Hunter et al. stated that fixation did not seem to prevent this complication. He proposed that scarce formation of adhesions on the posterior side of esophagus after laparoscopic fundoplication and a short esophagus may predispose to wrap herniation and suggested thorough esophageal mobilization and firm crural closure. 10 Recent recommendations to avoid wrap transmigration suggest minimal mobilization of the intra-abdominal esophagus and placement of esophageal-crural sutures. 8
In this study, we investigate the impact of wrap-crural fixation and minimal esophageal dissection in prevention of wrap transmigration after laparoscopic Nissen fundoplication in children.
Materials and Methods
A prospective randomized study was conducted on 46 children who underwent laparoscopic Nissen fundoplication for GERD in our tertiary pediatric surgery center in the period from January 2015 to December 2018.
Inclusion criteria
Cases with GERD not responding to optimal medical treatment
Age between 3 months and 18 years.
Exclusion criteria
Cases with hiatal hernia
Cases for redo fundoplication
Cases requiring feeding gastrostomy in addition to fundoplication
Cases with neurological impairment.
Patients were randomly divided into two groups [each group included 23 patients] using block randomization [ABAB]: Group A where the wrap was fixed to diaphragmatic crura and Group B without wrap crural fixation. Minimal esophageal dissection with preservation of the phrenoesophageal ligament were done in both groups.
The sample was calculated using G Power 3.1.9.4, 2018. Based on an effect size of 0.85, alpha error of 0.05, power of 80%, ratio of intervention group to comparison group of 1:1, the required sample size was 46 patients [23 patients in each group].
Operative technique
With the patient placed in a modified lithotomy position, five trocars were inserted as follows: one transumbilical, two in right and left midclavicular lines one to two fingers-breadth below costal margin, one just below xiphisternum, and fifth one in left anterior axillary line at umbilical level.
Dissection was started from left side. Gastric fundus was mobilized by dividing short gastric vessels and detachment of retrofundic area till left crus was visible. We then turn our attention to right side, starting by division of pars flaccida of gastrohepatic ligament above left gastric vessels. Minimal posterior esophageal mobilization to create a retroesophageal window. Preservation of the phrenoesophageal ligament was a critical step in all cases.
Hiatus was then closed using two nonabsorbable interrupted figure of eight sutures. Then, a short wrap is formed with two or three interrupted nonabsorbable sutures, using 2/0 Ethibond to achieve a fundoplication ∼2–3 cm in length. Stitches were passed through esophagus to fix the fundoplication.
In group A, the wrap was fixed to both crura with two interrupted sutures using 2/0 Ethibond (shown in Figure 1). Whereas in group B no wrap crural fixation was done. Finally, the abdomen was re-explored, hemostasis was assured, and ports were removed under direct vision.

Intraoperative image of the wrap.
Postoperatively, proton pump inhibitors (PPI) was prescribed for 2 weeks to all cases and then stopped or continued according to symptoms. Follow-up visits were after 1 week, 2 weeks, 2 months, 6 months, and then when needed. Routine oral contrast study was done 1 year postoperatively.
Primary outcome measure was detection of wrap transmigration and herniation into chest with a contrast study 1 year postoperative, secondary outcome measures were operative time, intraoperative complications, hospital stay, postoperative complaints and duration of antireflux medications.
Results
This study was conducted on 46 patients in our pediatric tertiary center. Patients were randomly divided into two groups [A and B]; each group included 23 patients. In group A wrap crural fixation was done, whereas in group B no fixation was done. In group A age range was 0.5–8 years with mean of 2.39 years, whereas in group B age range was 0.5–12 years with mean of 3.85 years. In group A mean weight was 11.58 kg and range was 3.8–30 kg, whereas in group B mean weight was 15.10 kg and range was 6–30 kg (Table 1).
Comparison Between Studied Groups According to Age, Weight, and Operative Time
U, Mann–Whitney test; T, Student's t-test.
In group A mean operative time was 101 minutes, ranged between 80 and 130 minutes, whereas in group B mean was 94.5 minutes, ranged between 45 and 150 minutes.
All cases were completed laparoscopically without conversion to open surgery. There were no operative complications in both groups. Oral feeding was started on the first postoperative day in all cases, and hospital stay ranged from 3 to 6 days without difference between the two groups.
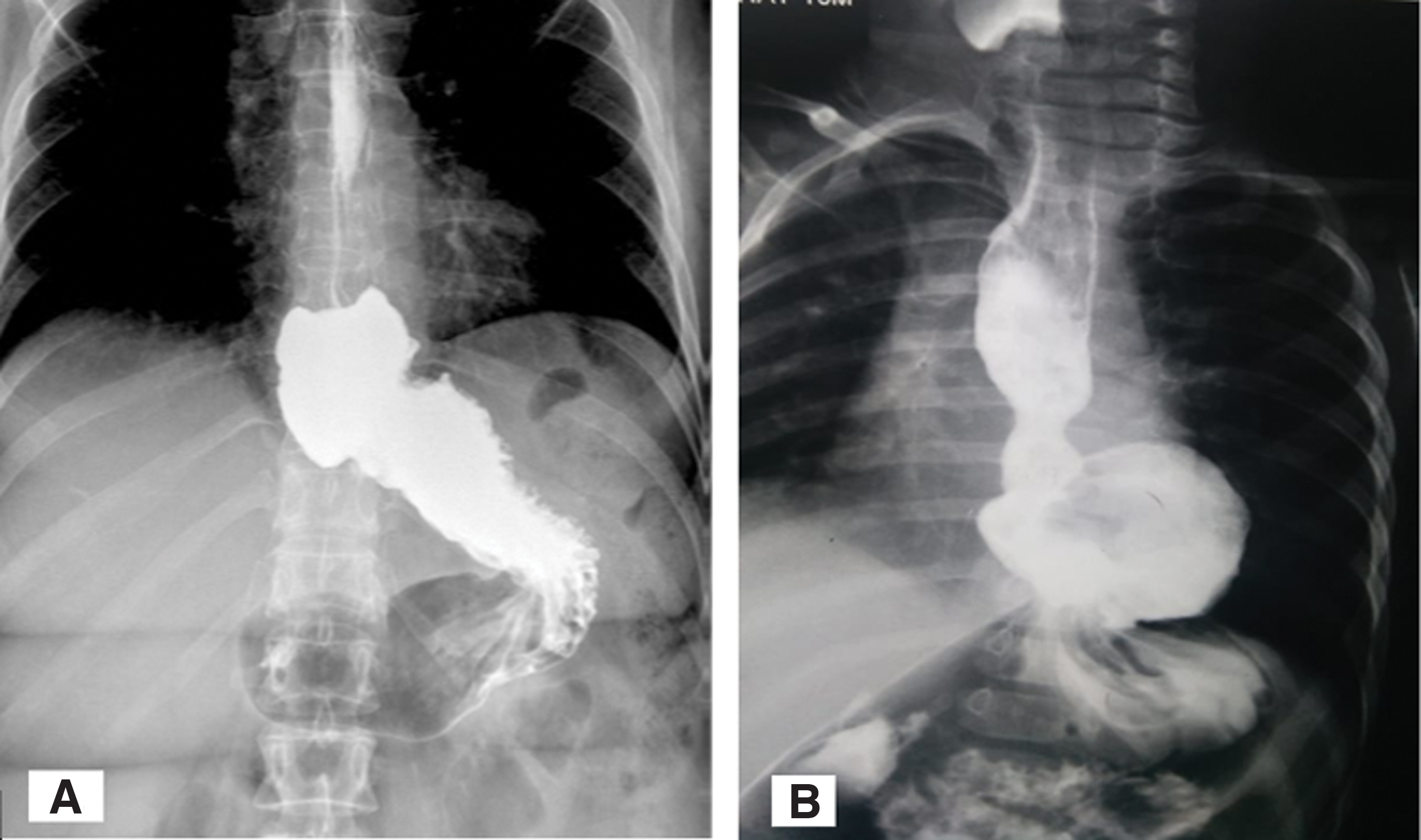
In group A symptoms disappeared and PPI stopped in a range of 2–4 weeks, whereas in group B range of postoperative PPI was 2–9 weeks and two cases showed recurrence of symptoms. These 2 cases showed wrap transmigration in postoperative contrast study (shown in Figure 2) and 1 of them required reoperation due to intractable severe GERD (Table 2).
Comparison Between Studied Groups According to Postoperative Findings
χ 2 , chi square test; FE, Fisher's exact test.
Discussion
Age and weight of our patients in each group were almost similar and there were no statistically significant differences in demographic data. Similar characteristics between groups add strength to our findings. Also, there was no significant difference in mean operative time between groups, although it was slightly longer in group A as expected.
Appropriate intra-abdominal esophageal length is an important component of antireflux mechanism.11,12 In adults, 3 cm or greater intra-abdominal esophageal length provides a competent lower esophageal sphincter 100% of the time. 13 Reflux has been shown to be more likely at the respiratory inversion point when lower esophageal sphincter length is <2 cm, of which <1 cm is intra-abdominal. 14 This evidence has led surgeons to believe that failure to mobilize an adequate esophageal length for intra-abdominal positioning can lead to unsuccessful results.
In contrast, Holcomb and colleagues 8 stated that these concepts have never been investigated in children. In contrast to adults, creation of retroesophageal window in children is easy with a gentle spreading maneuver that provides space to bring the fundus posterior to the esophagus. They concluded that minimal dissection around the esophagus is one of the factors that decrease risk of wrap transmigration after laparoscopic Nissen fundoplication in children. In the adult population, minimal esophageal dissection has excellent results in control of reflux symptoms, which provides a strong basis for a similar technique in children.15,16
Rothenberg 17 recommended adequate creation of intra-abdominal esophagus with limited hiatal dissection leaving the phrenoesophageal ligament and stressed on that dissection should not extend through phrenoesophageal ligament and up into hiatus as this increases risk of secondary hiatal hernia formation. In agreement with this, we performed minimal esophageal mobilization posteriorly to create retroesophageal window to adapt the fundus.
No operative complications were reported. This low complication rate can be explained because laparoscopic fundoplication is a minimally invasive clean surgery without gastrointestinal tract resection or bowel anastomosis. Therefore, common complications of laparoscopic surgery such as intraoperative bleeding, infectious complication, and port-site hernia are reported to be very rare.
Hospital stay ranged from 3 to 6 days with no difference between groups. Also, Rothenberg 17 reported 1–4 days as range of hospital stay for those patients admitted for fundoplication.
Postoperative results can be objectively assessed with different modalities, including barium swallow, endoscopy, pH monitoring, and manometry. 18 Although radiological failure is not always translated into clinical failure and vice versa, we can see postoperative recurrence of symptoms in otherwise radiologically normal child; we chose barium swallow test as our routine follow-up tool 1 year postoperatively because it is readily available, cheap, low fallacies, nonoperator dependent, and more acceptable to patient than other methods. Donkervoort et al. 19 and Dunne et al. 20 used barium swallow tests at 2 years postoperatively as part of their follow-up.
It is worth mentioning that recurrent GERD was detected by upper contrast studies in 2 of our cases in nonfixation group, but only one of them required redo surgery due to clinically significant recurrent GERD. Whereas group A showed persistently intra-abdominal wrap in all cases. Dunne et al. 20 stated in their study, “Even though there may be evidence of anatomical failure, the symptomatic outcome following laparoscopic antireflux surgery remains successful.”
In their studies, Hunter et al. 10 reported that intrathoracic wrap migration as one of the most frequent failure mechanisms after laparoscopic fundoplication. They stated that avoidance of intrathoracic wrap migration can be achieved by adequate esophageal mobilization, secure diaphragmatic closure, and avoidance of events leading to increased intra-abdominal pressure without mentioning wrap fixation. Also, Zucker 21 suggested the same causes for immediate postoperative intrathoracic wrap migration and they added that severe retching soon after surgery and/or sudden increase in intra-abdominal pressure due to a fall or blow can lead to late wrap migration.
Wu et al. stated that wrap-crural fixation is associated with significant decrease in transmigration and need for secondary intervention or reoperation. 22 Also, Peter et al. 8 has shown that placement of esophagocrural sutures and minimal dissection around the esophagus results in a more than twofold reduction in wrap transmigration after laparoscopic Nissen fundoplication but in their more recent study, 23 they found that with minimal phrenoesophageal dissection, there is no additional benefit from esophagocrural sutures.
Based on the results of this study, there is no significant statistical difference between the two groups regarding the incidence of wrap transmigration [P = .489] and the need for reoperation [P = 1].
Conclusion
In laparoscopic Nissen fundoplication, with minimal esophageal dissection and preservation of the phrenoesophageal ligament, there is no additional benefit from wrap-crural fixation in prevention of wrap transmigration.
Footnotes
Acknowledgment
Special thanks for Dr. Marwa Shawky [High Institute of Public Health, University of Alexandria] for her great assistance in methodology design and statistical analysis.
Authors' Contribution
All authors attest that they meet the current ICMJE criteria for authorship.
Concept and supervision by S.S. and A.K.; design by M.Z. and A.K.; materials by M.Z.; data collection and processing and written by M.Z. and A.F.K.; analysis and interpretation by M.Z. and K.A.; critical review by M.A. and M.E.S.
Statement of Ethics
Approval of the Ethics Committee of our Faculty was obtained. The researchers complied with the International Guidelines for Research Ethics. Anonymity and confidentiality of participants were maintained. An informed consent was taken from the guardians of participants.
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.