
Abstract
Surveillance colonoscopies for patients with ulcerative colitis (UC) are necessary to monitor for the development of cancer and its precursor, dysplasia. The management of dysplasia in the setting of UC has been evolving over the past two decades. This is in large part due to higher resolution colonoscopes and development of advanced endoscopic techniques, such as chromoendoscopy, endoscopic mucosal resection, and endoscopic submucosal dissection. Mucosal evaluation, as well as identification and removal of dysplastic tissue, has improved markedly, such that the majority of dysplasia is now considered visible. Whereas previously random biopsies were deemed necessary for surveillance, currently their value is uncertain. Surveillance with high-definition colonoscopes is recommended and consideration of chromoendoscopy is suggested. During colonoscopy, if visible dysplasia is identified and removed completely, continued surveillance is appropriate. If dysplasia is unresectable or there are other high-risk factors such as primary sclerosing cholangitis or multifocality, patients should undergo colectomy. If random biopsies are taken and high-grade dysplasia is identified, that is, invisible dysplasia, patients should similarly consider colectomy. Surgical options include total proctocolectomy with end ileostomy versus ileal pouch–anal anastomosis. Patients undergoing pouch surgery must continue surveillance for dysplasia of the rectal cuff and the pouch. Although surgical management remains an important option for dysplasia in the setting of UC, endoscopic surveillance and resection have improved tremendously, leading to a shift in the overall management strategies for these patients.
Introduction
It is well known that patients with ulcerative colitis (UC) are at high risk of developing colorectal cancer (CRC) when compared with the general population. The increased risk is estimated to be between 2 and 16 times higher for inflammatory bowel disease (IBD) patients, and it accounts for upward of 15% of mortality in patients with IBD.1–5 The average interval from diagnosis of UC to development of cancer is ∼16–21 years, and specifically, the risk of developing invasive cancer is ∼7% at 20 years, 7%–14% at 25 years, and 30% at 35 years.3,4,6–9
Chronic inflammation in the colon leads to the development of dysplasia, defined as neoplastic changes within the colonic epithelium without invasion into the lamina propria, which, in turn, may progress to invasive cancer. Surveillance and prompt identification of dysplasia allow for appropriate intervention and prevention of progression to cancer. Although the management of invasive cancer is well established, the management of dysplasia in UC has markedly evolved over the past two decades. Newer guidelines reflect the improvement in endoscopic image quality and the development of techniques such as chromoendoscopy and advanced endoscopic polypectomy.
Pathogenesis
The pathogenesis of cancer in the setting of IBD differs from that of the non-IBD patients. In traditional sporadic CRC, the adenoma–carcinoma sequence results in the transformation of normal colonic mucosa into adenomatous tissue, followed by the progression to invasive cancer. This is based upon the alterations in a stepwise progression of oncogene activation and inactivation of tumor suppressor genes. In IBD, the adenoma–carcinoma sequence is replaced with the inflammation–dysplasia–carcinoma sequence. 10 The background setting of chronic inflammation results in cytokine-induced oxidative stress leading to the development of mucosal neoplasia. The sequence of events is similar to other inflammatory conditions in that there are repeated cycles of inflammation, healing, and regeneration of epithelium. This results in the development of hyperplastic epithelium, followed by the development of flat dysplasia, and eventually, invasive carcinoma. Alterations in p53 result in the initial dysplasia due to chromosomal instability, and finally alterations in p16 and APC result in the development of invasive cancer. 11 Field effect, the formation of molecularly altered premalignant patches in normal appearing tissue, may underly the development of synchronous dysplasia, as pancolonic chromosomal instability has been demonstrated in patients with UC.12,13
Risk Factors
The same risk factors that exist for the development of IBD are also thought to be implicated in the development of CRC within this patient population. IBD is believed to be the result of environmental triggers acting upon a combination of pre-existing genetic and intestinal factors that induce a compromised intestinal immune response, which is then followed by mucosal inflammation. These risk factors can be grouped into patient-specific risk factors and disease-specific risk factors. Patient risk factors can be further subdivided into nonmodifiable and modifiable. Nonmodifiable risk factors include a younger age at diagnosis and family history of CRC, especially when diagnosed before the age of 50 years. Male gender has also been shown to carry a 60% higher risk of developing CRC. 14 The microbiome has been implicated in the development of IBD and CRC, but the true effect of this is still unclear. Intestinal barrier function is essential in protecting against inflammation and tumor development. Alterations in the microbiome, including a loss of Faecalibacterium prausnitzii, result in the reduction of short chain fatty acids, specifically butyrate and propionate, which are essential for the maintenance of intestinal homeostasis. This variation in microbiome combined with a Western diet, rich in processed foods and red meat and low in high-fiber foods, has been shown to increase the risk of the development of CRC. Disease-specific risk factors include the extent of the disease, duration of the disease, severity of the inflammation, and the presence of concomitant primary sclerosing cholangitis. Patients with quiescent disease and less inflammation are at a lower risk for developing malignancy than those with more severe cases of inflammation or who have more frequent and severe flares. The presence of pseudopolyps and/or strictures is also associated with an increased risk of developing invasive malignancy. 14
Historical Perspective
As mentioned previously, the management of colonic dysplasia in the setting of UC has markedly changed over time. It was previously thought that a significant portion of dysplasia was not visible during colonoscopy. Therefore, due to poor visualization, the recommendation for surveillance was 4-quadrant random biopsies every 10 cm, totaling at least 33 biopsies. A 1994 meta-analysis evaluating surveillance colonoscopy for UC demonstrated that if dysplasia was found, there was a high risk of concomitant CRC. 15 Of patients with low-grade dysplasia at colonoscopy who underwent immediate colectomy, 19% were found to have cancer; in those with high-grade dysplasia on colonoscopy, 42% were found to have invasive cancer on colectomy. These high rates of synchronous cancer on colectomy guided discussions with patients and recommendations for colectomy. However, it is important to note that these recommendations were in the era of standard-definition endoscopy, before the development of high-definition colonoscopes, implementation of advanced endoscopic techniques, and before the advent of biologic therapy. Because of these advances with resultant changing management strategies for patients with dysplasia, the SCENIC (Surveillance for Colorectal Endoscopic Neoplasia Detection and Management in Inflammatory Bowel Disease Patients: International Consensus Recommendations) international consensus statement on surveillance and management of dysplasia in IBD patients was published in 2015 (Table 1). The SCENIC guidelines 16 provide recommendations that focus on the method by which colonoscopy should be performed. In addition, the American College of Gastroenterology (ACG) published evidence-based guidelines in 2019 regarding CRC prevention in UC (Table 2). 17 The ACG guidelines focus on when to perform screening and how to manage the subsequent results and future surveillance.
Summary of SCENIC Consensus Statements
GI, gastrointestinal; IBD, inflammatory bowel disease; NBI, narrow band imaging; SCENIC, Surveillance for Colorectal Endoscopic Neoplasia Detection and Management in Inflammatory Bowel Disease Patients: International Consensus Recommendations.
Summary of American College of Gastroenterology Guidelines for Management of Colorectal Cancer Prevention in Ulcerative Colitis
CT, computed tomography; GI, gastrointestinal; PSC, primary sclerosing cholangitis; UC, ulcerative colitis; US, ultrasound.
Endoscopic Surveillance
Patients with UC are recommended to begin routine endoscopic surveillance starting 8 years after the initial diagnosis, except in cases of primary sclerosing cholangitis, in which case screening should start immediately. 17 The frequency of surveillance should be every 1–3 years and should be based upon the individual risk factors, including the severity of inflammation seen on prior endoscopic examinations.
High-definition endoscopy has been demonstrated to identify more lesions than standard endoscopy, and it is considered the standard of care. Standard-definition endoscopes were used commonly through the 1990s and early 2000s. In comparison, high-definition endoscopes, which were introduced ∼15 years ago, allow for a much more detailed visualization of the mucosa. It is important to underscore that these examinations should be performed by an experienced endoscopist, and that the colon preparation should be excellent to maximize detection of dysplastic lesions.
In addition to improved image quality with high-definition colonoscopes, chromoendoscopy is a technique that may help to identify dysplastic tissue. In this technique, dilute methylene blue or indigo carmine is sprayed on the mucosa and the endoscopist looks for areas that appear different from the surrounding area in terms of color, pattern, or level. Chromoendoscopy has not been shown in randomized controlled trials or meta-analyses to be better than high-definition white-light endoscopy, but there may be some benefit over standard-definition white-light endoscopy. 18 Both the SCENIC consensus statement and ACG guidelines suggest chromoendoscopy, though the latter argues for selective use.16,17 The utilization of narrow band imaging, though helpful for the detection of adenomas in otherwise normal colons, is not recommended in the setting of IBD given the background inflammation that may be present. 16
During colonoscopy, there are two ways biopsies are taken: targeted versus random. Targeted biopsies address a visible lesion that is either removed or biopsied. Random biopsies are taken when no lesion is seen, and the colon is instead randomly sampled. As mentioned, the prior recommendation for surveillance in UC was to perform 33 random biopsies throughout the colon. However, more recent data call this practice into question, as the ability to survey the colon has improved. It is now thought that only 10% of dysplasia comes from random biopsies and the remaining 90% comes from targeted lesions that are visible to the endoscopist on high-definition endoscopy. 19 Both the SCENIC consensus statement and the ACG guidelines call into question whether random biopsies are necessary, though there are no definitive recommendations.16,17
Pathology
When dysplasia is identified, it should be confirmed by two appropriately trained pathologists, given a high rate of interobserver variability. When there are disagreements regarding the presence of dysplasia, the patient should undergo medical optimization and repeat endoscopy in 3–12 months. 20
Dysplasia: Invisible and Visible
Dysplasia is characterized according to appearance and this helps to guide management decisions. The term dysplasia associated lesion or mass was previously utilized, but found to be confusing, and it was recently abandoned in favor of a more specific classification of endoscopically detected dysplasia.16,21 Invisible dysplasia is defined as dysplasia that is identified on random biopsies without an associated visible lesion, whereas visible dysplasia is associated with an endoscopically visible lesion. Visible dysplasia can then be subdivided into polypoid (pedunculated or sessile) and nonpolypoid (superficial, flat, and depressed). Further characterizations include the presence of ulceration and whether the borders are distinct or indistinct. The management of dysplasia depends upon (1) the visibility of the lesion on endoscopy, (2) the ability for complete endoscopic excision, and (3) the histologic findings of the biopsy. If lesions are visible, then they should be excised completely, and advanced endoscopic techniques can be employed when necessary. Previously, recommendations were to biopsy the normal mucosa surrounding visible lesions to ensure no dysplasia was remaining; however, this is proving to be unnecessary given advances in visualization and studies that demonstrate low rates of residual dysplasia in this surrounding tissue. 22
For patients with resected visible polypoid dysplasia (Fig. 1), whether by snare polypectomy or an advanced endoscopic polypectomy technique, there does not seem to be a high risk of subsequent CRC; these patients can forego colectomy and instead be surveyed. In a meta-analysis of 10 studies containing 376 patients with polypoid dysplasia, the incidence of subsequent CRC was 2%, and the pooled CRC rate was 5.3 cases in 1000 years of patient follow-up. 23 These patients can be followed with repeat endoscopy at 1 year or sooner depending on the size of the lesion.
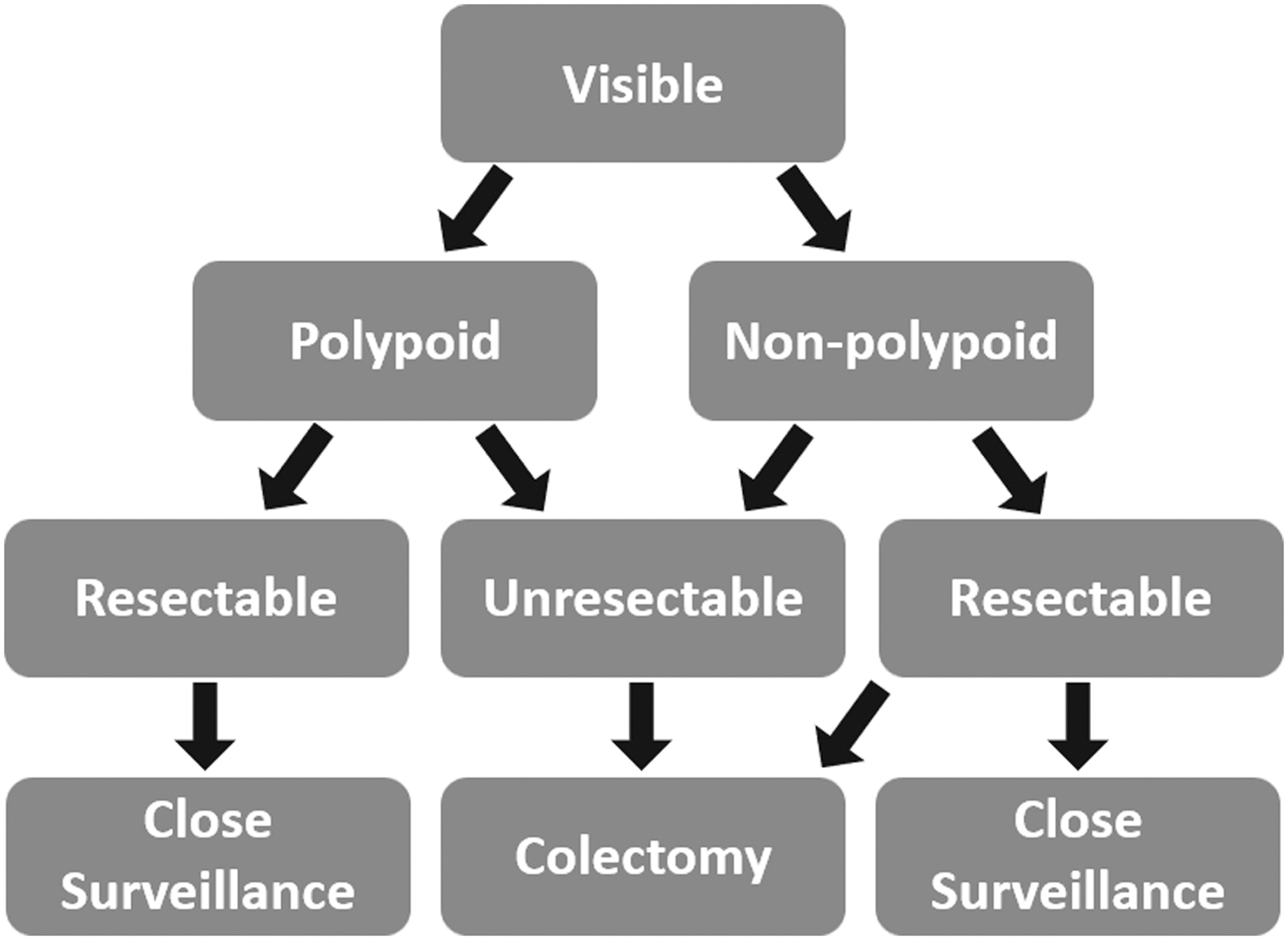
Visible dysplasia treatment algorithm in patients with ulcerative colitis.
Nonpolypoid dysplasia (Fig. 1) that is seemingly resectable can present more of a challenge and may need to be removed by an advanced endoscopist using techniques such as endoscopic mucosal resection or endoscopic submucosal dissection. The borders of these lesions may be less distinct. Options for these lesions include close surveillance at 3 months versus colectomy taking into account the lesion itself, multifocal disease, and/or patient-specific factors. For polypoid or nonpolypoid dysplasia that is unresectable, surgical resection is the obvious choice.
When dysplasia is found on random biopsies (invisible dysplasia), referral should be made to an IBD endoscopist to undergo high-definition endoscopy with chromoendoscopy. 16 If invisible dysplasia is still present, the grade of dysplasia—high-grade versus low-grade dysplasia—may play a role (Fig. 2). For patients with high-grade dysplasia, colectomy should be considered. The approach to low-grade dysplasia is less clear, but patients should have close surveillance at the very least with repeat colonoscopy after 3–6 months and consideration of colectomy. If a patient has primary sclerosing cholangitis or multifocal invisible low-grade dysplasia, colectomy should be strongly considered.
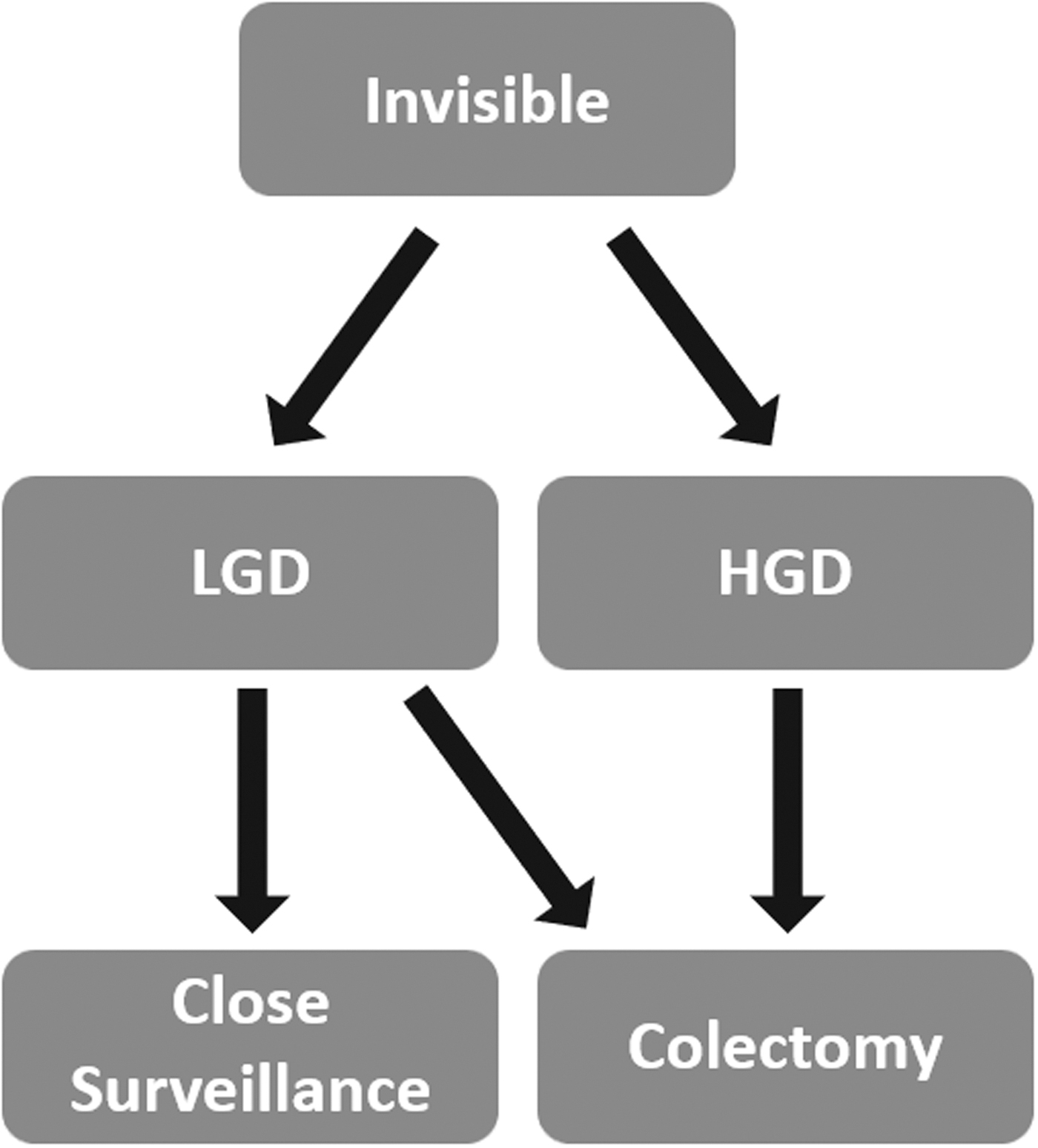
Invisible dysplasia treatment algorithm in patients with ulcerative colitis. HGD, high-grade dysplasia; LGD, low-grade dysplasia.
Surgical Management
The standard surgical recommendation for dysplasia in UC is total proctocolectomy. Total proctocolectomy removes all or nearly all of the potential dysplastic tissue, resulting in significant cancer risk reduction. Total proctocolectomy has several reconstruction options, which include ileal pouch–anal anastomosis (IPAA) or end ileostomy, and less commonly, continent ileostomy (Koch pouch). Segmental colectomy or total colectomy has been explored as options for dysplasia, but should only be performed in well-selected patients and is contraindicated in the setting of active inflammation. Segmental colectomy has been shown in small retrospective studies to have a low rate of metachronous cancer.24,25 These procedures should be reserved for rare instances where total proctocolectomy is considered prohibitively risky.
Dysplasia in Patients with IPAA
Patients who have undergone total proctocolectomy with creation of IPAA remain at risk, although low, of developing malignancy. There are two common methods for creation of IPAA: the double-stapled technique and the hand-sewn technique. The double-stapled technique utilizes a stapler to transect the rectum distally and an end-to-end anastomosis stapler to create the pouch to anal anastomosis and is associated with improved functional outcomes.26,27 The hand-sewn technique includes performing a mucosectomy followed by a hand-sewn pouch to anal anastomosis. Although these procedures substantially reduce the risk of development of UC-related dysplasia and malignancy, they do not completely eliminate it as the anal transition zone still contains rectal mucosa that remains at risk. A large review of >3000 patients found that the risk of developing neoplasia of the pouch increases from 0.9% to 5.1% at 5–25 years after creation of the pouch, but only 0.36% of patients developed invasive adenocarcinoma. 28 The only risk factor identified for the development of dysplasia was a history of CRC before pouch creation. 29 When a mucosectomy is performed at time of pouch creation, it does not eliminate the development of subsequent dysplasia.28–30 Despite the low risk of development of dysplasia, routine surveillance of the pouch is still recommended, though there are no universally accepted guidelines for surveillance. In general, pouchoscopy is recommended at 1 year after surgery. Subsequent pouchoscopy frequency is recommended anywhere from 1 to 5 years. If there is a history of neoplasia, frequency of pouchoscopy should increase accordingly. 31 A recent study suggests patients who are asymptomatic may require no endoscopic pouch surveillance. 32
When dysplasia does occur, it may occur within the pouch itself, within the residual rectal cuff, or within the anal transition zone, but it most commonly occurs in the anal transition zone. There are no official guidelines for the management of pouch neoplasia. In the setting of any invasive adenocarcinoma, appropriate staging studies should be obtained, and surgical excision and/or chemotherapy may be considered. In the setting of squamous cell carcinoma, appropriate staging should be performed and Nigro protocol and pouch excision have been described. 33 Regardless, the management of patients with neoplasia of the pouch should be discussed in the setting of a multidisciplinary tumor board and/or IBD clinic.
Conclusions
The evolution of dysplasia management in UC remains ongoing as a result of newer endoscopic technology and polypectomy techniques. Situations that previously necessitated colectomy are now being managed with advanced endoscopic techniques and more aggressive surveillance. Unresectable dysplasia and invasive cancer remain indications for total proctocolectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.