
Abstract
Aim:
To evaluate the effect of laparoscopic-assisted resection and colorectal anastomosis with a stapling technique in the treatment of Hirschsprung disease (HSCR) in infants.
Methods:
From June 2018 to January 2019, 25 cases of HSCR diagnosed by clinical examination and pathology were selected at the Children's Hospital, School of Medicine, Zhejiang University, China. All children were treated with standard laparoscopic-assisted transanal endorectal pull-through surgery (the modified Swenson technique). The short segment type and the typical type with a descending colon–rectum anastomosis were both included. The long segment type had an ascending colon–rectal anastomosis after ascending colon turnover. The colorectal anastomosis was divided into traditional manual anastomosis and straight intraluminal stapler (SIS) anastomosis. According to the different methods of anastomosis, the patients were divided into a traditional group and a SIS group. Age, gender, body weight, operation time, blood loss, postoperative anal exhaust and defecation time, postoperative hospitalization time, and postoperative short-term complications were analyzed retrospectively.
Results:
A total of 25 children were diagnosed with HSCR. There were 17 boys and 8 girls, and their average age was 10.20 months (interquartile range, 8.60–11.30). Their average body weight was 7.90 kg (interquartile range, 7.50–8.40). There were 17 cases of the typical type, 5 cases of the short segment type, and 3 cases of the long segment type. The different colorectal anastomosis methods were divided into 10 cases in the traditional group and 15 cases in the SIS group. There were no intraoperative complications, wound infections, or anastomotic fistula. Compared with the SIS group, children in the traditional group had an increased operative time (129.5 versus 103.00 minutes; P < .0001), increased intraoperative blood loss (20.00 versus 7.00 mL; P < .0001), increased postoperative hospitalization time (12.00 versus 9.00 days; P = .0003), and increased postoperative defecation time (18.40 versus 13.20 hours; P < .0001). After 6–12 months of follow-up, there was no anastomotic stenosis or enterocolitis in the SIS group. In the traditional group, 1 child had anastomotic stenosis, which improved 6 months after anal dilatation. One case of enterocolitis occurred 4 months after the operation and was cured after enema and infusion.
Conclusion:
Laparoscopic-assisted resection combined with colorectal anastomosis with the stapling technique in the treatment of HSCR in infants is feasible. It had a short operation time, less bleeding, less trauma, and a rapid recovery of postoperative intestinal function. The anastomosis was smooth, wide, and reliable, and anastomotic fistula and stenosis did not occur.
Introduction
Hirschsprung disease (HSCR)
After >20 years of development, laparoscopic-assisted HSCR radical surgery has resulted in various approaches, each of which has unique advantages and disadvantages. The traditional porous laparoscopic-assisted pull-through operation is more mature and extensive. Umbilical single-channel laparoscopy is more difficult because of the limitations of the operation space, but there is almost no scar on the abdominal wall after the operation.
Regardless of the type of operation, the transfer of the lithotomy position is basically manual anastomosis. Although intraluminal staplers have been used routinely in adult digestive tract surgery, there are few reports of intraluminal stapler anastomosis performed in children. On the basis of performing a large number of traditional laparoscopic-assisted HSCR radical surgeries, we used laparoscopic-assisted HSCR radical surgery combined with the colorectal stapling technique in infants and obtained better clinical results, which are reported as follows.
Materials and Methods
Ethical Statement
Our article is a clinical case report about the discussion of different surgical methods, not a clinical trial. Before the operation, we had communicated with the family members of the children and followed their independent choices. All operations were in compliance with the specifications and approved by the hospital ethics committee.
Clinical information
From June 2018 to January 2019, 25 cases of HSCR diagnosed by clinical examination and pathology were selected at the Children's Hospital, School of Medicine, Zhejiang University, China. According to the diagnosis and an expert consensus of HSCR and the operating guidelines for laparoscopic HSCR surgery (2017 edition), a standardized diagnosis, treatment procedures, and postoperative complications diagnosis and treatment strategy were adopted.
The preoperative diagnosis was based on the clinical manifestations, barium enema, rectal anal manometry, and rectal mucosal suction biopsy. Intraoperative frozen sections were used to quickly determine the resection site, and postoperative routine pathological sections further confirmed the diagnosis. After 2–7 days of colon lavage with warm saline before the operation, abdominal distension was obviously improved. There was no fecal mass retention in the colon by B ultrasound examination, and broad-spectrum antibiotics were used intravenously 30 minutes before the operation.
Postoperative anal defecation and a fluid diet were resumed 2 weeks later, and the expansion of the anus lasted 1 month.
This study was approved by the ethics committee of the Children's Hospital, School of Medicine, Zhejiang University. All of the parents of the children included in this study signed informed consent forms, and the operation method was chosen voluntarily by the parents of the children.
Surgical methods
We used laparoscopic-assisted transanal endorectal pulling through the diseased intestinal segment (modified Swenson technique). The children underwent general anesthesia with tracheal intubation in the supine position and three 5 mm trocars laparoscopic technique was performed (Fig. 1A). The first trocar is placed on the edge of the umbilicus for observation of the field of view. The second trocar was placed at the umbilical level of the midclavicular line of the left abdomen. The third trocar is at the midpoint of the umbilicus of the right abdomen and the anterior superior iliac spine. Insufflation pressure was 8–10 mmHg. We explored the abdominal cavity under laparoscopy to observe the transition area and biopsied two to three serosa muscle layers to determine the normal intestinal position. According to the different pathological types, different ways of dissociating the HSCR were used. When dealing with the short segment type and typical type cases, we used an ultrasonic knife to dissociate the rectum, sigmoid colon, and part of the descending mesocolon and lateral ligaments.

The scope of surgical separation included proximal separation to the proximal end of the normal bowel of ∼5 cm, distal anterior wall separation to the opening of the peritoneal reflex, and posterior wall separation to the distal presacral level of the rectum. When dealing with the long segment type cases, we used an ultrasonic knife to free the rectum, sigmoid colon, descending mesocolon, transverse mesocolon, greater omentum, and part of the ascending mesocolon. We preserved the ascending colon artery branch and ileocolonic artery and preserved the ascending colon of ∼10 to 15 cm, which was then ready for anastomosis.
The operation was transferred to the anus, and the child's lithotomy position was used to drag the free colon out of the anus using the intussusception dragging method. Then, we cut it off in the middle of the rectum, dragged the diseased colon out of the body for excision, and pulled the proximal end of the colon down to perform the anastomosis.
Colorectal anastomosis performed with the stapling technique: after dovetail cutting, the 3-0 absorption line was sutured along the edge of the broken end of the intestinal tube, and the intestinal cavity was opened for use. We chose the appropriate model of a straight endoluminal stapler according to the diameter of the intestinal tube, inserted the free-end nail drill bit inside the purse string, and tightened the purse string suture to fix it. After the distal rectum was turned out from the anus, the anterior wall was retained to a distance of 2.5 cm from the dentate line, and the posterior wall was retained to a distance of 1.5 cm from the dentate line. The two sidewalls of the rectum were also wedge shaped, and the 3-0 absorption line was placed along the intestine. The end edge was closed by a purse-string suture, and finally, the free-end nail drill rod was passed out at the midpoint of the purse-string suture. After the stapler connecting rod was inserted, the colorectal nail anastomosis was completed outside the anus to form an oblique anastomosis, with preserved rectum anterior walls of 1.5–2 and 0.5–1.0 cm in the posterior wall (Fig. 1D, E). An anal canal was routinely indwelled, without a urinary catheter or an abdominal drainage tube.
Traditional manual anastomosis: We used the same invaginating drag-out method to drag the free colon out of the anus and cut it off in the middle of the rectum. Then, we dragged the diseased colon to the outside of the body and cut the proximal end of the lower colon with dovetail cutting. After the distal rectum was turned out from the anus, the anterior wall was retained to 1.5 cm from the dentate line, and the posterior wall was retained to 0.5 cm from the dentate line. Both sidewalls of the rectum were also wedge shaped, and the intestines at both ends were sutured with a single layer of 4-0 absorption thread.
The Mann–Whitney nonparametric t test was used to compare the differences between groups, and P < .001 was considered statistically significant.
Results
A total of 25 children were diagnosed with HSCR. There were 17 boys and 8 girls, and their average age was 10.20 months old (interquartile range, 8.60–11.30). Their average body weight was 7.90 kg (interquartile range, 7.50–8.40). There were 17 cases of the typical type, 5 cases of the short segment type, and 3 cases of the long segment type. There were 10 children in the traditional group, including 7 boys and 3 girls, with an average age of 9.90 (7.98–11.35) months and an average weight of 8.15 (7.73–8.95) kg. There were 15 children in the straight intraluminal stapler (SIS) group. Among them, 10 were boys and 5 were girls, with an average age of 10.70 (8.80–11.30) months and an average weight of 7.80 (7.30–8.20) kg (Table 1).
Comparative Analysis of Clinical Data Characteristics (Straight Intraluminal Stapler Group Versus Traditional Group)
SIS, straight intraluminal stapler.
There were no intraoperative complications, wound infections, or anastomotic fistulas. Compared with the SIS group, children in the traditional group had an increased operative time (129.5 versus 103.00 minutes; P < .0001), increased intraoperative blood loss (20.00 versus 7.00 mL; P < .0001), increased postoperative hospitalization time (12.00 versus 9.00 days; P = .0003), and increased postoperative defecation time (18.40 versus 13.20 hours; P < .0001).
After 6–12 months of follow-up, there was no anastomotic stenosis or enterocolitis in the colorectal stapling group. There was no anastomotic stenosis or enterocolitis in the observation group. In the traditional group, 1 child had anastomotic stenosis, which improved 6 months after anal dilatation. One child had enterocolitis 4 months after the operation and was cured after dilatation of the anus and an enema. The children in the SIS group received water 13 hours after surgery, followed by a full-fluid diet 24 hours later, had loose stools four to seven times per day after the operation, and a gradual decrease to one to three times per day after 1 month (Table 2 and Fig. 2).
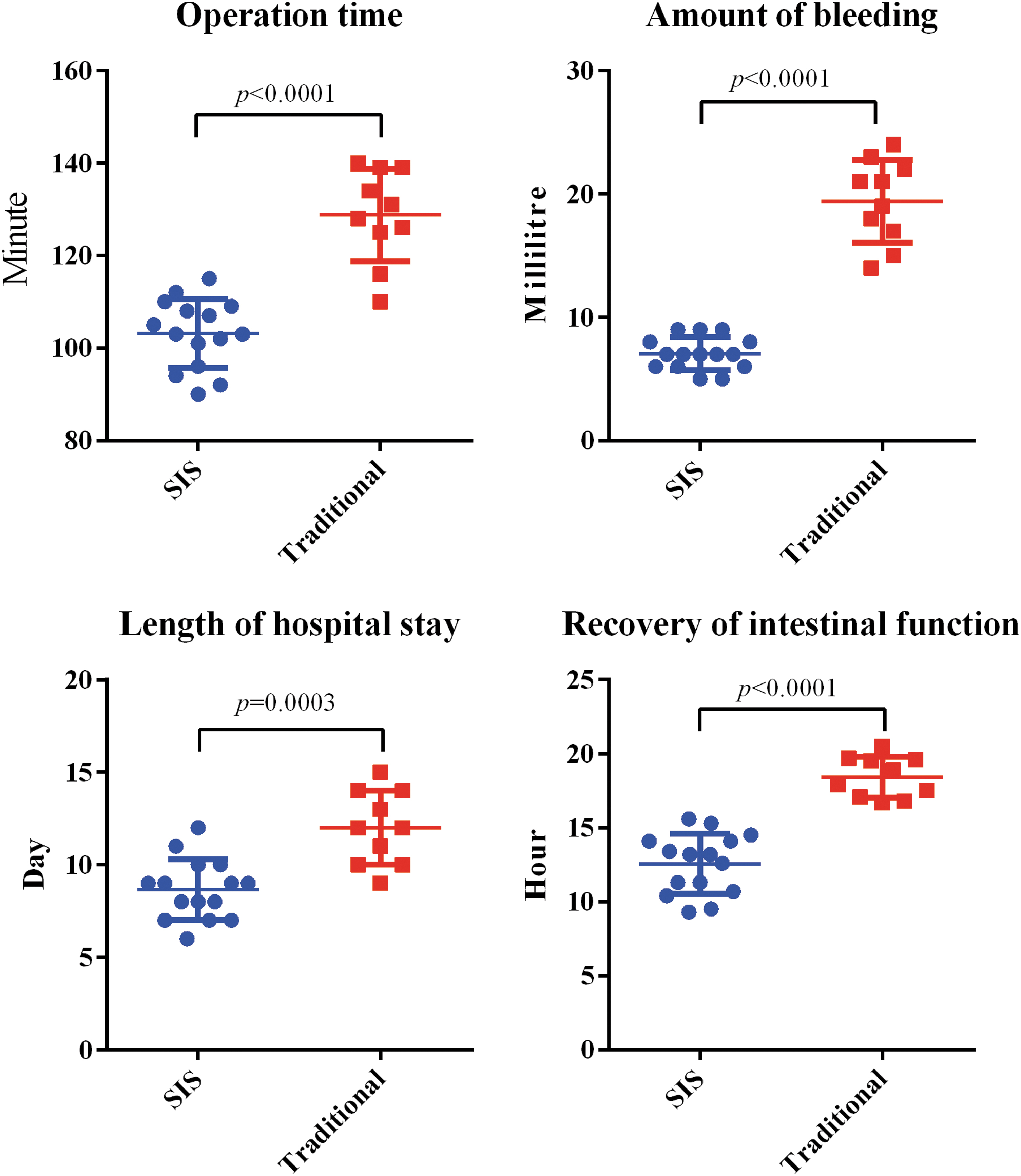
Comparison of perioperative data of SIS group versus traditional group. SIS, straight intraluminal stapler. Color images are available online.
Comparison of Perioperative Data of Colorectal Nailing Group Versus Traditional Group
SIS, straight intraluminal stapler.
Discussion
HSCR is also known as aganglionosis, the incidence of which is ∼1/5000, but the exact etiology is still not very clear. Most scholars believe that it involves enteric neural crest cells that proliferate, migrate, and differentiate abnormally to the distal end of the intestine during embryonic development of the enteric nervous system. This would lead to the absence of ganglion cells in the distal muscular layer and submucosa of the bowel, a persistent spasm in the distal bowel, compensatory hypertrophy and dilatation of the proximal bowel, and symptoms such as constipation, abdominal distension, and bowel obstruction, which seriously affect the growth and development of children.4–6
Traditional children's HSCR surgery methods include Soave, Swenson, Rehbein, and Duhumel. In 1995, Georgeson carried out laparoscopic-assisted transanal drag surgery, and soon, this concept was widely promoted. 7 In 1998, DelaTorre–Mondragon reported a simple transanorectal drag operation,8,9 but this operation can only be performed close to the intestinal wall to process the mesangial vessel. Strong pulling on the anus can easily cause damage to the external sphincter. Therefore, it was limited to the free rectum and sigmoid colon, especially for newborns and infants. If the lesion was longer, it needed to be combined with a laparoscope or a small incision through the umbilical region to complete the operation.
Therefore, the current mainstream surgery for children with HSCR has evolved from traditional transabdominal and transanal surgery to laparoscopic-assisted minimally invasive surgery. However, laparoscopy only completes the freeing of the intra-abdominal colon, which is only part of the Hirschsprung surgery.
Most of the anastomosis operations have been performed by hand sutures, and relatively few staplers have been used. Van der Zee et al. reported that the Endo-GIA suture device was used in Duhumel surgery for HSCR in infants, and the results were satisfactory. 10 There are also reports suggesting the value of Endo-GIA in resection of HSCR. 11 The stapler has been widely used in adult digestive tract reconstruction surgery.12,13
After years of experience, our department has completed hundreds of laparoscopic-assisted modified Swenson operations and has accumulated rich clinical experience in Hirschsprung surgery. Therefore, we attempted to use laparoscopic-assisted Hirschsprung resection combined with colorectal nail anastomosis to treat HSCR in infants. This surgical method not only used the advantages of laparoscopic free colon but also combined the fast, convenient, efficient, and firm characteristics of using a stapler to perform the anastomosis, which has shown good treatment results.
Our research showed that the two groups had significant differences in operation time, intraoperative blood loss, postoperative bowel function recovery time, and hospital stay. Therefore, the use of staplers had certain advantages in these aspects.
Attention should be given to the process of intestinal resection and colorectal nailing and anastomosis when dragging out of the anus orifice:
Choose the right-sized SIS (Ethicon). According to our experience, the model SDH21A-SDH25A (lumen size 12.4–16.4 mm) is suitable for children from 6 months to 1 year old, and the SDH21A is appropriate for babies ∼6 months old, the SDH25A can be used for infants ∼1 year old, whereas the SDH29A (lumen size 20.4 mm) can be selected for babies >1 year old or with a larger intestinal diameter and a thicker intestinal wall. The model of the stapler is selected and adjusted according to the age of the child and the condition of the intestine during the operation. In the early stages of the use of the stapler, we mainly chose infants and young children. Since the dilatation of the intestines and intestinal wall hypertrophy of infants and young children are relatively not serious, the difference in the diameter of the proximal and distal ports of the anastomosis is small. After accumulating a certain amount of surgical experience, on the premise of choosing a suitable stapler, you can try to expand the indications. An oblique anastomosis with a high anterior wall and a low posterior wall can still be performed with the stapler. During the anastomosis, the distal rectum could be turned out from the anus, the anterior wall is kept 2.5 cm away from the dentate line, and the posterior wall is kept 1.5 cm away from the dentate line. More of the intestinal wall is appropriately reserved than in manual anastomosis to prepare for the placement of the stapler. The intestinal wall tissues at both ends of the anastomosis are fixed with purse-string sutures to fix the free end of the spherical stapler. The purse-string suture is performed as far as possible along the edge of the intestinal tube. When closing the purse string, we should pay attention to all intestinal wall tissues that are collected in the stapler to prevent incomplete nailing. Nailing can be performed outside the anus, which is more conducive to checking the nailing effect. If the nail is off or bleeding occurs, it can be partially reinforced with absorbable sutures. According to our experience, if the stapler is firmly nailed, no nail removal occurs, and no case requires manual suture reinforcement. The key is to make a good purse string so that the proximal and distal intestinal wall tissues are all collected into the stapler to prevent the occurrence of anastomotic leakage caused by incomplete nailing.
We believed that it is necessary to indwell the anal canal after the operation. The anal canal helps to discharge gas and liquid from the colon, reduces edema and narrowing, and protects the anastomosis. Two weeks after the operation, the anus could be expanded for 1 month to prevent anastomotic stenosis and to train defecation.
The incidence of postoperative Hirschsprung-related enterocolitis is related to anastomotic stenosis. 14 One case of postoperative enterocolitis occurred in the traditional group, which may be related to anastomotic stenosis, so we used expansion of the anus to address it. In another case, anastomotic stenosis occurred after the operation, which might be related to scar healing after anastomotic inflammation. Therefore, we believe that the incidence of enterocolitis is low after using an appropriately sized stapler, which is related to forming a wide and smooth anastomotic stoma, which does not cause inflammation, which leads to scars and stenosis.
Owing to the large differences in the diameter of the intestinal tube in children of different ages, the diameter of the intestinal tube and the hypertrophy of the intestinal wall in children with HSCR are variable. We needed to prepare several different types of staplers. At present, our number of cases is still small. The follow-up time is still short. After more cases are accumulated, additional statistical analysis could be performed.
In summary, laparoscopic-assisted resection combined with colorectal nailing in the treatment of HSCR in infants is feasible. It is associated with a short operation time, less bleeding, minimal trauma, and rapid recovery of postoperative intestinal function. The anastomosis is smooth, wide, and reliable, and anastomotic fistula and stenosis rarely occur.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
The funding was provided by the Scientific research project of Zhejiang Provincial Department of Education (N20160011).