
Abstract
Background:
During transanal total mesorectal excision (TaTME), sustained dilation of the anal canal occurs, which can cause anatomical and functional damage to the sphincter complex. This study aimed to analyze the impact of laparoscopic total mesorectal excision (LaTME) and TaTME in anorectal sphincter function.
Materials and Methods:
An observational study was conducted comparing two cohorts of patients who underwent LaTME or TaTME for rectal cancer. The two groups were paired for comparison based on age, gender, and distance of the neoplasm to the anal margin. The anorectal function was assessed by manometry before surgery and at least 6 months after primary intervention or stoma closure. The intestinal function was assessed using the low anterior resection syndrome (LARS) score.
Results:
Twenty-two patients were included. There were no significant differences in baseline characteristics between groups except for the time between surgery and testing. A decrease in the mean resting and squeeze pressures between pre- and postoperative manometry was observed in both the treatment groups, the difference being only significant in the squeeze pressure values (TaTME P = .003; LaTME P = .004). After surgery, squeeze pressure reduction correlated with a worsening of the LARS point count (rho 0.587; P = .004). The time elapsed since surgery was negatively correlated with the LARS point count (rho −0.696; P = .001) and the difference between pre- and postoperative mean squeeze pressures (rho −0.499; P = .018).
Conclusion:
Manometric findings after TME are comparable between the laparoscopic and the transanal approach. Deterioration of both anal sphincter function and LARS improves with time after surgery.
Introduction
Low anterior resection with total mesorectal excision (TME) is currently considered the gold standard for the surgical treatment of middle and lower third rectal cancers, as it is associated with low local recurrence and high long-term survival rates.1,2 TME is technically demanding, with certain factors increasing the difficulty of the procedure, such as male gender, high body mass index, or the presence of a voluminous mesorectum.
Over the last decade, transanal TME (TaTME) has gained popularity, its primary purpose being to facilitate the dissection in the most distal portion of the rectum. 3 This surgical approach has proven to be feasible, reliable, and effective in the short term.4–6 Nevertheless, to adopt TaTME as a standard surgical technique, efficacy and safety in the long-term follow-up must be demonstrated in well-designed multicenter randomized trials, such as COLOR III and the North American Multicenter Phase II Study on TaTME.7,8
Rectal resection is frequently associated with a disordered bowel function, known as low anterior resection syndrome (LARS), leading to a decrease in patients' quality of life (QoL). 9 In this regard, TaTME, a technique that combines both prolonged anal dilation and increased distal dissection with a lower anastomosis, could be accompanied with worse functional outcomes than laparoscopic total mesorectal excision (LaTME).10,11 A recent systematic review, including studies that compared TaTME and LaTME, found no relevant differences in QoL and bowel function between them. 12 However, less evidence is available concerning anorectal function worsening after TaTME and its effect on functional outcomes.13–15
This study aimed to analyze the impact of TaTME and LaTME in anorectal sphincter function, assessed by anal manometry, and its correlation with the LARS score.
Materials and Methods
The present is an observational study based on a prospective database, comparing a cohort of rectal cancer patients treated by TaTME with another cohort of patients operated on using the conventional laparoscopic approach.
Patients undergoing surgery for cancer of the middle or lower rectum at La Mancha Centro General Hospital between 2014 and 2018 were included, excluding those with stage IV cancer, tumor recurrence, T4 neoplasm, synchronous or metachronous neoplasms, medical history of familial adenomatous polyposis coli, hereditary nonpolyposis colorectal cancer, Crohn's disease or ulcerative colitis, as well as stoma carriers at the time of the study or those who had not undergone stoma closure at least 6 months before the study. Patients in the TaTME group were pair-matched in a 1:1 ratio to a control LaTME group, according to age ±5 years, gender, and distance of the neoplasm to the anal margin. This study was conducted in accordance with the Declaration of Helsinki and was approved by our institutional review board.
The TaTME approach was carried out with two surgical teams working simultaneously (laparoscopic and transanal). For the transanal approach, a retractor to expose the anal canal (Lone Star Retractor; Lone Star Medical Products, Inc., Houston, TX) and the Gel Point Path transanal® platform (Applied Medical, Rancho Santa Margarita, CA) were used. The specimen was extracted transanally when the size of the tumor and the diameter of the pelvis made it possible, or through a suprapubic assistance incision. The anastomosis was undertaken manually or with a 28 or 31 mm circular stapler (DST Series EEA Stapler, Covidien). Diverting loop ileostomy was performed selectively.
The anorectal function was assessed by manometry (Solar GI HRM H20, 24p, Compact Pole; Medical Measurement Systems, Inc.) before surgery and at least 6 months after the operation or stoma closure in the case of a derivative ileostomy. The main parameters analyzed were mean resting and squeeze pressures, both measured in millimeters of mercury (mmHg). Intestinal function and QoL were assessed in the postoperative period, coinciding in time with manometry, using the validated Spanish versions of the LARS (v.1.0) and the European Organization for Research and Treatment of Cancer (EORTC QLQ-C30 v.3.0) questionnaires, respectively.9,16,17
For the statistical analyses, the Stata/ICv15.1 statistical package was used. The qualitative variables were summarized with relative and absolute frequencies, and the quantitative ones with measures of central tendency and dispersion according to the distribution of the variable determined by the Shapiro–Wilk test.
The comparisons between both treatment groups were made using the Mann–Whitney U-test for independent samples or the Pearson χ 2 and Fisher's exact tests as appropriate. For the before/after comparisons, the Wilcoxon matched-pair signed-rank test was used. The Spearman correlation coefficient was used to analyze the relationship between time elapsed from the intervention to the postoperative tests with manometry, bowel function, and QoL, as well as the relationship between manometric alterations and bowel function. The differences between variables were assessed with a limit of statistical significance P < .05.
Results
Seventy-four patients with middle or low rectal cancer were operated on over the study period; 21 underwent TaTME and 53 LaTME. Eleven patients in the TaTME group agreed to participate in the study and were pair-matched with 11 patients in the LaTME group.
The main clinical and demographic features of the 22 patients included in the study are described in Table 1. Nearly 86% of the patients received neoadjuvant treatment. There were no significant differences between groups except in the time between surgery and testing, which was longer in the LaTME group (LaTME 56.6 months [interquartile range (IQR) 41.7–79.8] and LaTME 35.2 months [IQR 26.7–49.5], P = .028).
Clinical and Demographical Characteristics of Patients
Values are presented as median (interquartile range) or n (%).
ASA, American Society of Anesthesiologists physical status classification; BMI, body mass index; CTx, chemotherapy; LaTME, laparoscopic total mesorectal excision; RT, radiotherapy; TaTME, transanal total mesorectal excision.
No differences were found between groups either in the mean resting pressure or the mean squeeze pressure values. When comparing pre- and postoperative results, a decrease in the mean resting and squeeze pressures was observed in both treatment groups, although this decrease was only statistically significant for the mean squeeze pressure (TaTME group P = .003 and LaTME group P = .004).
The size of the differences between pre- and postoperative results was also comparable between groups (mean resting pressure difference P = .670; mean squeeze pressure difference P = 1.000) (Fig. 1). Five (23%) out of 22 patients had mean resting pressures under the preoperative assessments' reference values, and 9 (41%) patients in the postoperative ones. For the mean squeeze pressure value, 1 (5%) patient presented a preoperative value under the normal range, and 5 (23%) patients in the postoperative measures did so.
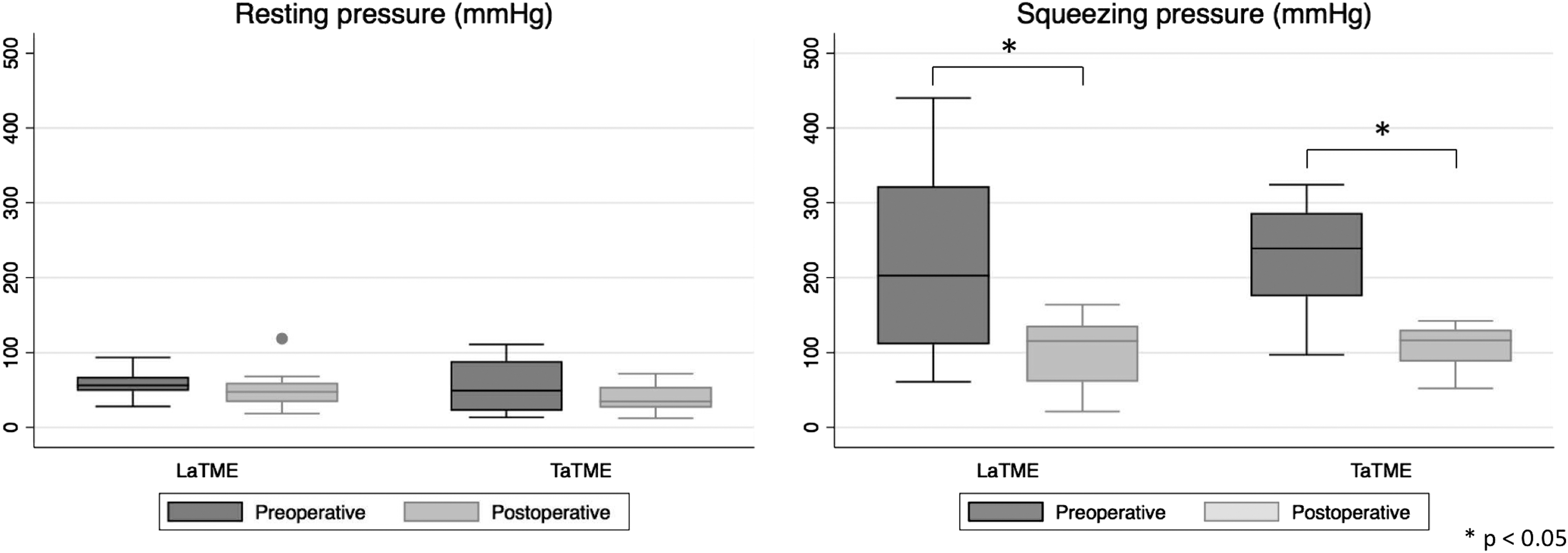
Box plot. Results of preoperative and postoperative manometry. LaTME, laparoscopic total mesorectal excision; TaTME, transanal total mesorectal excision.
When LARS was analyzed using the LARS questionnaire, no meaningful differences were found between the two groups, neither in the LARS point count (LaTME 34 [IQR 26–39] and TaTME 37 [IQR 27–39] P = .468) nor in the LARS score, not even in any of the five items included in the questionnaire. In the QoL study, no differences were found between groups in the global health status of the EORTC QLQ-C30 tool (LaTME 83.3 [IQR 83.3–100] versus TaTME 83.3 [IQR 75–91.7], P = .267). Figure 2 shows the comparisons of every single component of the EORT QLQ-C30 between the two groups.

Comparison of each component of EORTC QLQ-C30 between LaTME and TaTME. EORTC, European Organization for Research and Treatment of Cancer; LaTME, laparoscopic total mesorectal excision; TaTME, transanal total mesorectal excision.
Correlations
The difference between pre- and postoperative mean squeeze pressures, assessed among the 22 patients included in the study, was positively correlated with the functional outcomes, showing a worsening of the LARS point count as squeeze pressure decreased after surgery (rho 0.587; P = .004). A negative correlation was found between the time elapsed from surgery to completion of the postoperative tests and both the global LARS point count (rho −0.696; P = .001) and the difference between pre- and postoperative mean squeeze pressures (rho −0.499; P = .018). These results indicate that the longer the time since the intervention, the lesser the severity of the LARS and the smaller the decrease in postoperative mean squeeze pressures compared with preoperative values. Besides, the time elapsed since the intervention was positively correlated with the global QoL (rho 0.447; P = .037) (Table 2).
Correlations Between Time from the Intervention to the Postoperative Tests and Manometric, Functional, and Quality-of-Life Outcomes of the 22 Patients, and Between the Preoperative/Postoperative Difference in Squeeze Pressure and Functional Outcomes
EORTC, European Organization for Research and Treatment of Cancer; LARS, low anterior resection syndrome; LaTME, laparoscopic total mesorectal excision; TaTME, transanal total mesorectal excision.
Discussion
There is a growing interest in TaTME in rectal cancer among colorectal surgeons. Besides safety and efficacy considerations, this relatively new surgical approach should also prove comparable results with the standard anterior resection technique within other parameters of interest, such as QoL and functional outcomes. Concerns have also been raised regarding the potential risk of damage to the anal sphincter during TaTME. 12
Several studies have analyzed sphincter function after rectal cancer surgery assessed using anorectal manometry. Regardless of the open or laparoscopic approach, many authors have objectified a decrease in manometric parameters after rectal surgery, with a progressive recovery over time since the intervention.18–23 In addition to the tumor's location, other factors such as radiotherapy seem to have a bearing on these results.24,25
In our study, with nearly 86% of patients receiving radiation therapy, mean sphincter resting and squeeze pressures showed lower values after TaTME and LaTME, although these differences were only significant for the mean squeeze pressures. The fact that both approaches shared the same pattern of manometric alterations makes us believe that the transanal access platform might have little to none impact on these results. Likewise, some extent of deterioration in both resting and squeeze pressures has been found after other procedures where a transanal device is used, such as transanal endoscopic microsurgery or transanal minimally invasive surgery, also recovering normal values 1 year after surgery. 26 Moreover, in studies where the anal sphincter was evaluated with endoanal ultrasonography, similar changes were objectified in the anal sphincter after LaTME and TaTME.19,27
We only know of three other studies that have analyzed the manometric function of the anal sphincter after TaTME. Wu et al. studied 19 male patients with lower rectal cancer, in whom manometric assessment was performed 1 month after TaTME surgery. All the patients in this study presented resting and squeeze pressures within the normal range. 13
In a recently published observational study, Bjoern et al. compared postoperative manometric results between LaTME and TaTME. Although only postoperative measurements were performed, they found mean resting and squeeze pressures under reference values in 60% and 44% of the patients, respectively, with no significant differences between the LaTME and TaTME groups. 14 These results are in accordance with our findings, with a higher percentage of patients with mean resting pressures under reference values (41%), compared with mean squeeze pressures (23%) in the follow-up manometry. However, we also observed preoperative manometric mean resting pressures under the reference range in many patients (23%) compared with mean squeeze pressures (5%).
Finally, De Simone et al. studied 33 rectal cancer patients before and after TaTME and found a significant decrease in the mean resting pressures 12 months after surgery. Interestingly, a slight, nonsignificative increase in the postoperative maximum squeeze pressures was also observed. 15 This manometric squeeze pressure pattern is somewhat different from that observed in our study, which can be partially explained by disparities in the manometric study protocol that can make comparisons between centers difficult. Anyhow, the inclusion in our study of a control group with the same manometric procedure allows us to assert that both surgical approaches share a similar pattern of manometric alterations (Table 3).
Studies Evaluating Manometric Outcomes After Transanal Total Mesorectal Excision
Results presented as median (range) or mean ± standard deviation, unless stated otherwise.
Distance to the anorectal junction.
Results expressed as maximum squeeze pressure instead of mean pressure.
LaTME, laparoscopic total mesorectal excision; RT, radiotherapy; TaTME, transanal total mesorectal excision.
LARS is a frequent and relevant complication after surgery on rectal cancer. Different questionnaires have been used for its assessment, the most widespread one being the LARS score. 16 In our study, both treatment groups presented high scores in the LARS questionnaire, with an improvement in both groups with time elapsed from surgery. These outcomes were similar to those described in a recent meta-analysis, including five observational studies that compared bowel functional outcomes after LaTME and TaTME using the LARS questionnaire. 12 Besides, some studies have found manometry to be related to the severity of functional symptoms after rectal cancer surgery.22,23
Specifically focused on TaTME, Bjoern et al. analyzed the correlation between LARS score and manometry parameters, finding a not statistically significant decrease in both main resting and squeeze pressures with the increase of the severity of LARS symptoms. 14 In the present study, better LARS scores were found in patients with a lower decrease between pre- and postoperative mean squeeze pressure. Although it is not mandatory for LARS diagnosis, anorectal manometry can help to monitor LARS progression and treatment response.28,29
This study has some limitations, including its observational nature, the small sample size, the inclusion of the TaTME learning curve, and the absence of preoperative bowel function and QoL assessment. On the contrary, matched-pair analysis and the inclusion of pre- and postoperative manometric measurements provide greater validity and usefulness to our results.
Conclusion
Manometric findings after TME for rectal cancer are comparable between the laparoscopic and the transanal approach. Although larger studies on this topic are needed, these results suggest that the use of a transanal device during TaTME does not increase the risk of sphincter apparatus and anorectal function worsening. Deterioration of both anal sphincter function and LARS improves with time after middle and low rectal cancer surgery.
Footnotes
Acknowledgment
The authors thank José Manuel Zarco Murcia for English language editing.
Authorship Confirmation Statement
All the authors meet the International Committee of Medical Journal Editors (ICMJE) authorship criteria.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.