
Abstract
Background:
Our study aims to evaluate the influence of potential determinants of glomerular filtration rate (GFR) decrease after partial nephrectomy (PN), including renal parenchymal loss and other clinical, tumoral, and surgical factors.
Materials and Methods:
Eighty-six patients who had undergone PN and for whom preoperative and postoperative computerized tomography scans were available were selected. We calculated the preoperative total kidney volumes, tumor volumes, and postoperative total kidney volumes 1 year after surgery using a three-dimensional (3D) volume segmentation method. Factors that may be potential determinants of percent GFR decrease were also evaluated, including patient age, type of procedure (laparoscopic vs. open), comorbidity index, preoperative GFR, tumor size and volume, RENAL nephrometry score, warm ischemia time, and 3D calculated renal parenchymal loss. Clinical, surgical, and tumor parameters potentially associated with renal parenchymal loss were evaluated.
Results:
The mean age of the patients was 58 years, the mean tumor diameter was 3.6 cm, and the mean tumor volume was 11.7 cc. The mean percent of renal parenchymal loss was 22.3%, and the mean percent of GFR loss was 17.3%. The renal parenchymal loss was strongly associated with age (r = 0.702, P = .02), Charlson comorbidities index (r = 0.768, P < .001), and RENAL nephrometry score (r = 0.812, P < .001). In multivariate logistic regression analysis, older age, higher Charlson comorbidities index, higher percent renal parenchymal loss, and higher RENAL nephrometry score were independently associated with higher percent of GFR loss.
Conclusion:
Of all the factors analyzed, RENAL score and Charlson comorbidities index were the most accurate predictors of postoperative parenchymal loss. Also, the percent decrease in GFR at late time points was associated with renal volume preservation and quality of the remnant parenchyma.
Introduction
Partial nephrectomy (PN) has become the standard of care for patients with T1a renal tumors. 1 Currently, the indications for elective PN have been enlarged to larger tumors such as clinical T1b and T2a in carefully selected patients. 2 The aim of PN is to preserve renal parenchyma as much as possible with paying attention to negative surgical margins and a low complication rate. The volume and the quality of the remaining renal tissue are the determinants of glomerular function rate (GFR) after PN.
Preoperative assessment of patient-related risk factors such as age, chronic diseases, and comorbidities are important in decision-making process. However, in addition to these clinical conditions, the prominent parameter for deciding the operation type is the tumor volume and location. Accordingly, the role of volumetric measurement of tumor burden and estimated parenchymal loss is becoming increasingly important in decision-making before PN. Recently, kidney parenchymal volume has been shown as a predictor of renal function in kidney transplants. 3 In addition, it has been shown that tumor volume provides more prognostic information than tumor size alone after PN. 4 Although it is of obvious importance, the volumetric calculation of tumor and parenchymal loss have not been extensively studied due to the challenges in measuring the functional volume change. There is no agreement in the literature with respect to the ideal method of volumetric calculation of soft tissue. Numerous techniques have been used for calculation of total kidney and tumor volume using computerized tomography (CT) or magnetic resonance imaging; yet, they have not been much adequate for actual kidney anatomy.5,6 Three-dimensional (3D) volume segmentation is a novel method providing detailed and individual anatomy of the soft tissue.
In this study, we retrospectively measured total kidney volume and tumor volume using commercially available 3D reconstruction volume software in patients undergoing open or laparoscopic PN and evaluated the risk factors potentially associated with the parenchymal loss.
Materials and Methods
Patient selection
The study was carried out with the University of Health Sciences Turkey, Okmeydanı Training and Research Hospital Ethics Committee's approval dated 14.08.2018 and numbered 814. Informed consent form was obtained from all patients. Cases were selected from an Institutional Review Board approved database of consecutive patients who underwent open and laparoscopic PN from January 2005 to August 2016. Selection of patients for analysis was based on the inclusion criteria of treatment for a single unilateral kidney tumor, normal preoperative serum creatinine (range 0.5 to 1.5 mg/dL), and the availability of postoperative surveillance CT and serum creatinine. We excluded patients with a solitary kidney and patients with incomplete data from this study. Of 126 patients identified in the database, 86 met the inclusion criteria.
Open PN was performed with a flank extraperitoneal approach. The entire renal surface except for the tumor area was dissected from the overlying fat tissue. The renal artery was temporarily occluded. The tumor was removed en bloc with the perinephric fat lying on the surface of the tumor providing a 10 mm margin of normal renal tissue around it. Laparoscopic PN was performed using an intraperitoneal approach for all patients. The renal artery was clamped with a bulldog clamp. After PN was performed, sutures were done intracorporeally using absorbable thread with a piece of felt that was fixed with a Hem-o-Lok.
Retrospectively clinical, tumor-related and surgical parameters, including patient age at surgery, gender, type of procedure, preoperative GFR, radiographic and tumor volume, and warm ischemia time, were evaluated as potential predictors of postoperative GFR. Three-dimensional volumetric assessment of parenchymal loss was calculated with using available preoperative and postoperative CT data. In addition, serum creatinine and GFR were studied 12 months after surgery. All serum creatinine measurements were made at a single clinical reference laboratory. GFR was estimated using the modification of diet in renal disease two equation. 7 The correlation of each factor to parenchymal and GFR loss after postoperative 1 year was calculated.
Volumetric analysis
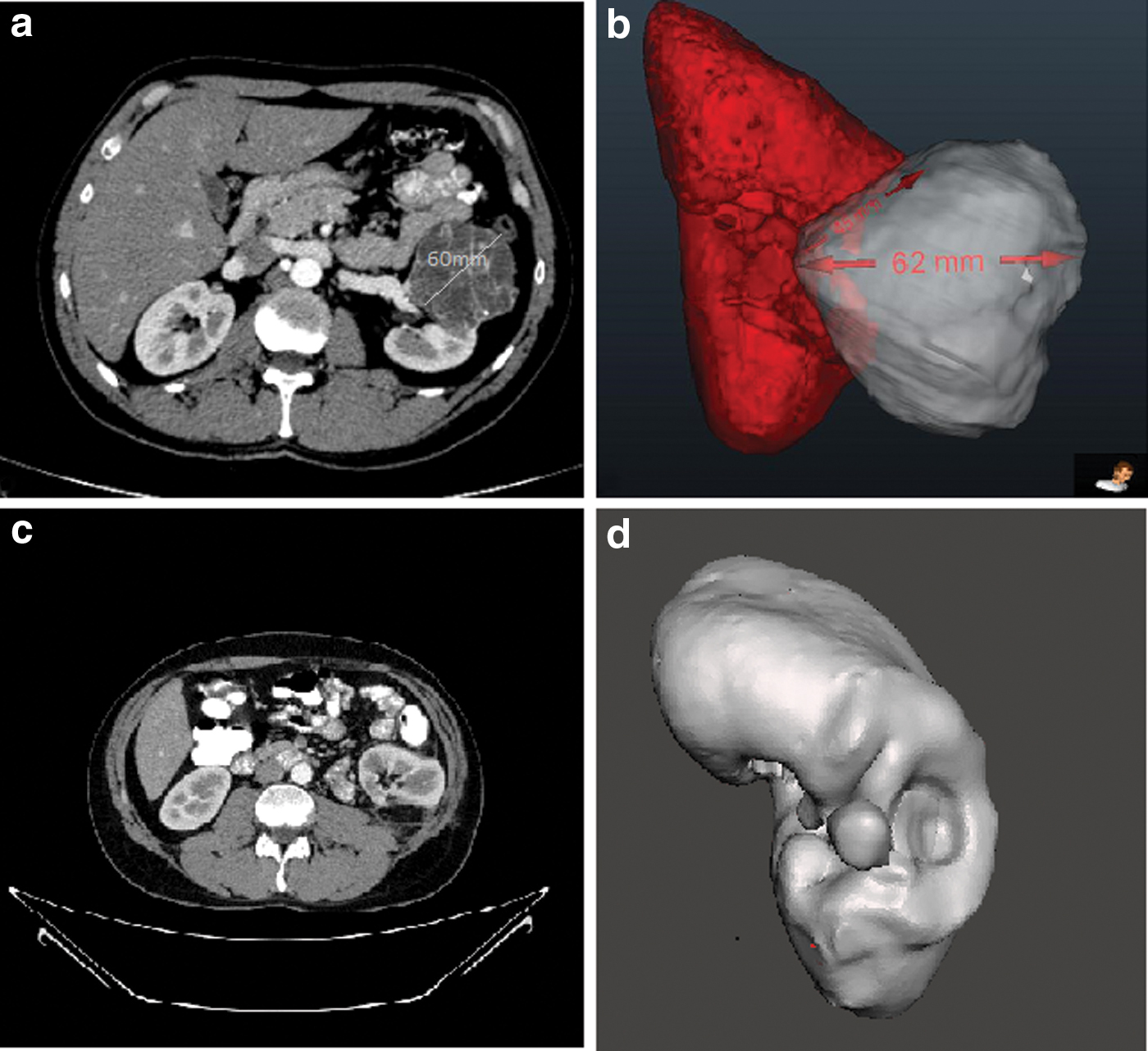
CT cross-sectional images data with 1 mm step-section and iodinated contrast medium were used for kidney and tumor volume segmentation. CT data (Digital Imaging and Communications in Medicine) were uploaded to special 3D segmentation software (Dornheim Segmenter, Magdeburg, Germany). Segmentation of kidney parenchyma and tumor was done by using semiautomatic tools of the segmentation software. First, threshold-based tool was used to define the soft tissue basis of Hounsfield unit attenuation; second, cutting tool was used to select the interested region; and third, the removal of artifacts from the desired region was done. Renal sinus fat, hilar vessels, and collecting system were excluded from volumetric segmentation to ensure that only parenchyma was included in the final volume. Each volume measurement was done three times in different scan planes and the results were averaged. Three volume segmentations were done with this method; (1) preoperative, the total volume of the functioning renal parenchyma and tumor, (2) the tumor alone, and (3) the volume of the functioning renal parenchyma 12 months after surgery. After the segmentation of kidney and tumor was finished, data were converted to three-dimension for calculation of total kidney volume and tumor volume with geometric analysis. The RENAL nephrometry score was calculated by the geometric analysis of 3D images, Figure 1.
Statistical analysis
Continuous variables with normal distribution were expressed as mean and range. Distribution of variables was assessed with the Kolmogorov–Smirnov test. The Mann–Whitney U test compared quantitative data, and the chi-square test was used for analysis of qualitative independent data.
Univariate and multivariate logistic regression analyses were done to identify the predictive factors for percent GFR loss (GFR <30% loss mL/minute/1.73 m2) 1 year after surgery. In both univariate and the multivariate analyses, we used odds ratio (OR) as the risk measure and its 95% confidence interval (95% CI). Associations between parenchymal loss (%) and GFR loss (%) with other variables were examined by Spearman's rank correlation analyses. A value P < .05 or an OR with 95% CI was considered statistically significant, and the software used was SPSS 22.0™ (IBM Corporation, San Ramon, CA).
Results
The baseline clinical and pathologic features of 86 patients are shown in Table 1. The mean age of the patients was 58. Mean radiographic tumor diameter was 3.6. The median RENAL score of the cases was 5 and the 50% clinical stage of the tumor was T1a. Overall, 33.7% of the PN cases were open, whereas the remainders were laparoscopic surgery. Final margins were negative in all cases. Warm ischemia was used in all surgeries with a mean duration of 26 minutes. No intraoperative major complications, including significant injury to an adjacent organ, major vessel, ureter, or hemorrhage, were reported. Perioperative complications were observed in 6 patients (6.9%), all of whom underwent open PN. Pneumonia (Clavien classification Grade II) and paralytic ileus (Grade II) occurred in 3 patients, and blood transfusion was required for 3 patients (Grade II).
Demographic, Pathological, and Operative Data of Patients
BMI, body mass index; CT, computerized tomography; PN, partial nephrectomy; SD, standard deviation.
Table 2 lists the 3D calculated volumetric analysis of operated kidney and renal function data. Median tumor volume was 11.7 cc (range 6.2 to 133 cc). The mean percent renal parenchymal loss per patient was 22.3% (range 11% to 49.4%) and the mean percent GFR loss per patient was 17.3% (range 6% to 53%). Figure 2 shows correlations of the factors found to be potentially significant in the prediction of percent renal parenchymal losses. Percent renal parenchymal loss was strongly associated with age (r = 0.702, P = .02), Charlson comorbidities index (r = 0.768, P < .001), and RENAL nephrometry score (r = 0.812, P < .001). Also, moderately associated with tumor diameter (r = 0.512, P = .022) and warm ischemia time (r = 0.301, P = .047). Figure 3 shows the relationship between percent glomerular filtration rate (GFR) losses with percent parenchymal loss, warm ischemia time, and Charlson comorbidities index.
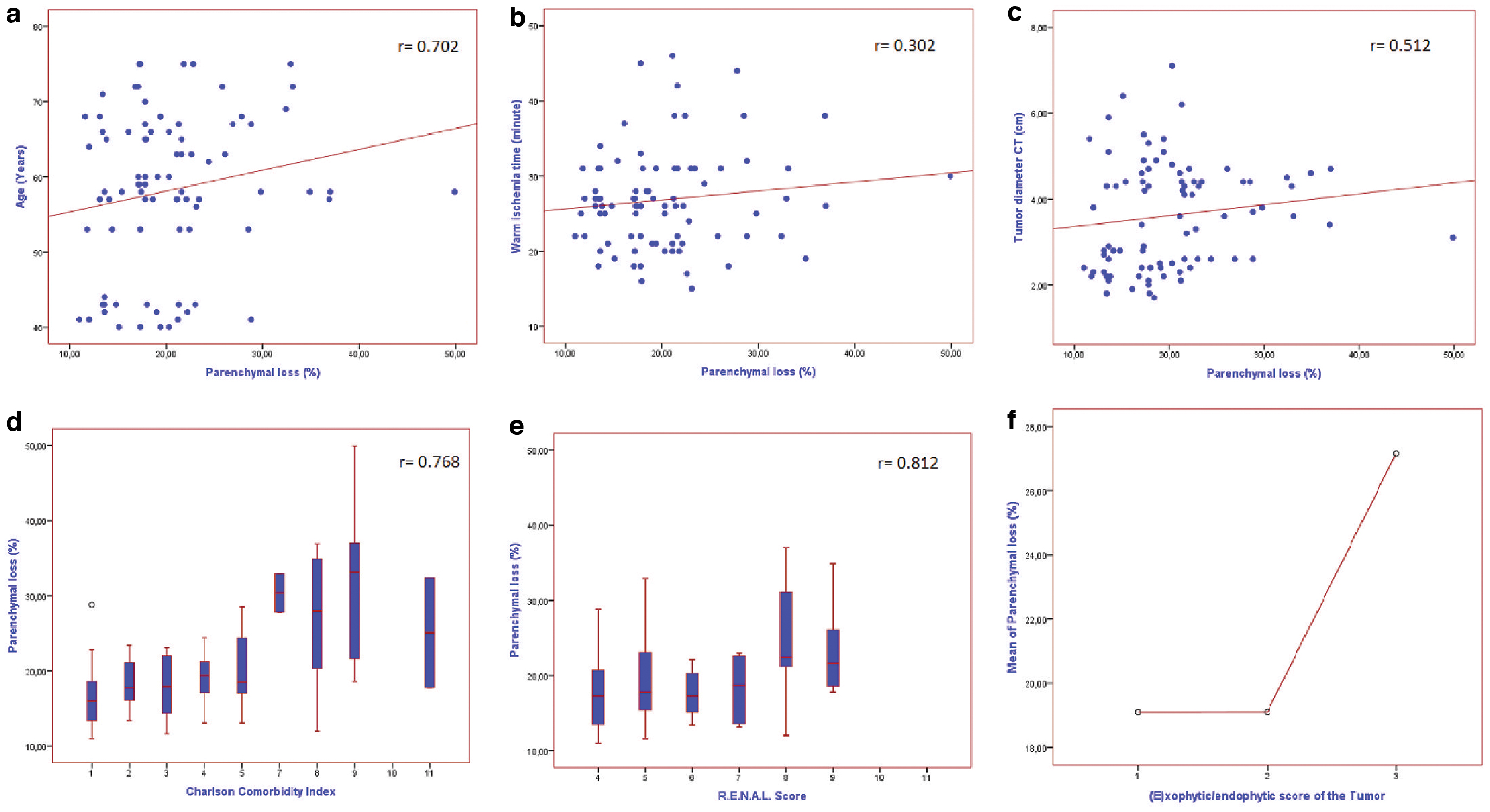
Correlations of the factors found to be potentially significant in the prediction of percent renal parenchymal losses.

Relationship between %GFR losses with percent parenchymal loss, warm ischemia time, and Charlson comorbidities index.
Volumetric and Functional Data Specifically Derived from the Operated Kidney
All GFR values were derived from the modification of diet in renal disease 2 equation.
3DKV, Three-dimensional kidney volume; 3DV, three-dimensional volume; GFR, glomerular filtration rate; SD, standard deviation.
On univariate analysis, age (P = .006), Charlson comorbidities index (P = .006), postoperative kidney volumes (P = .008), RENAL nephrometry score (P > .001), and percent renal parenchymal loss (P < .001) were associated with higher percent GFR loss. In contrast, higher percent GFR loss did not vary significantly with increased body mass index (P = .395) or warm ischemia time (P = .813). On multivariate logistic regression, age, Charlson comorbidities index, percent renal parenchymal loss, and RENAL nephrometry score remained independently associated with higher percent GFR loss, Table 3.
Analysis of Predictive Factors for Percent Glomerular Filtration Rate Loss 12 Months After Partial Nephrectomy
Bold values show statistically significant P value.
Italic values show statistically significant P value.
3DKV, Three-dimensional kidney volume; 3DV, three-dimensional volume; BMI, body mass index; CI, confidence interval; OR, odds ratio; PN, partial nephrectomy.
Discussion
We performed this study to identify the degree of relationship between the loss of parenchymal volume following PN and clinical, tumor, and surgical factors. Also, we investigated multiple factors as possible predictors for postoperative severe GFR loss. Some normal renal tissue is removed with the tumor to create a negative surgical margin or because vascular parenchyma is sacrificed for renography. Furthermore, quality of the residual renal parenchyma, which is associated with the age and comorbidities of the patient, could be other parameters effective on postoperative late GFR level. Therefore, we assessed these factors that could be attributable to the loss of normal parenchyma. We used the database of patients with a unilateral kidney tumor who underwent PN at our institution in the last 10 years who were known to have measured GFR data available. We studied patients preoperative and postoperative CT and converted them to 3D images for calculation of kidney and tumor volumes.
In this study, we found that the best predictors of parenchymal loss 1 year after PN were the RENAL nephrometry score, comorbidity index, and age of the patient. Tumor size, tumor volume, and warm ischemia time had weaker or borderline correlations with the parenchymal loss. Also, the most significant factors for severe GFR decrease were renal parenchymal loss and the comorbidity status of the patient. Overall, endophytic tumors were found to have a greater parenchymal loss than peripheral tumors. These findings may be partially explained by the need to excise additional renal parenchyma to adequately resect endophytic tumors than peripheral tumors because intrarenal tumor generally requires resection of the overlying but uninvolved renal parenchyma. Moreover, patients with higher comorbidity index may disturb the quality of residual renal parenchyma, resulting in greater GFR loss after surgery.
Numerous prior studies have shown that functional volume loss after PN directly associated with tumor burden and ischemia time.8,9 However, the result that we have found in this study is different from the others, that is, the parenchymal volume loss was moderately correlated with tumor volume or size. The correlation of parenchymal volume loss with the region of the tumor and the tumor depth was higher than tumor volume alone. Also, comorbidity index was another parameter that needs to be assessed for prediction of GFR loss before PN.
These data lead redefinition of determinants that contribute to the functional recovery of renal function after PN. The quantitative amount of parenchymal volume loss and the quality of the residual tissue are the predominant predictors of late GFR loss. Also, the quality of residual renal tissue is another parameter that could influence on late parenchymal loss due to increased vulnerability to ischemic injury. The recovery phase of the remaining functional volume, which is affected by trauma and ischemia during surgery, are primarily associated with the age and the medical comorbidities of the patient. Contemporary data support that warm ischemia time is not a major effecting factor on late GFR levels and functional volume loss. But as an exceptional subgroup, elderly population (older than 70 years of age) or patients with major medical comorbidities (Charlson score greater than 5) should be considered as the most likely population that may suffer from prolonged ischemia time.
Consequences of reduction in parenchymal volume after PN have been shown in experimental studies. Levine and colleagues had reported that there was a significant increase in the ratio of mesangial matrix surface to the glomerular surface, indicative of progressive diabetic nephropathy, in response to nephrectomy in diabetic rats. 10 Also, acceleration of renal injury was shown in obese Zucker rat models after nephrectomy. 11 While these experimental studies cannot be replicated in humans, it is reasonable to assume that similar consequences would occur after PN to subjects' with the kidney tumor, who are likely to be older and have high comorbidity scores.
Nephrectomy is associated with an acute and significant drop in the GFR, due to the immediate loss of renal parenchyma. In a retrospective analysis comparing 173 patients who underwent radical nephrectomy with 148 patients who underwent PN, Lau et al. 12 reported that after a median follow-up of 25 months postoperatively, the cumulative incidence of chronic renal deficiency (CKD) was 22.4% and 11.6% following radical and PN. In another study from a cohort of 662 patients who had normal preoperative creatinine, Huang et al. 13 compared the impact of partial or radical nephrectomy for T1a stage on the risk of postoperative CKD. Despite a normal serum creatinine level before surgery, CKD was present in 26% of the patients. Following the surgery, the 2-year probability of CKD was 35% for radical nephrectomy and 10% for PN. In our study, new onset CKD was found in 11 patients (18%) 1-year after surgery.
The patients that are diagnosed with kidney tumor are more prone to CKD due to older age, a long history of smoking and/or hypertension, and more likely to be obese. Especially in patients with moderate to severe renal insufficiency (CKD stage III/IV) cryoablation and radiofrequency ablation could be an alternative treatment for PN in selected subjects. Also, no differences were found between cryoablation and radiofrequency ablation in terms of complications rates and efficacy. 14 In a recent study, Woldu et al. 15 compared the renal parenchymal volume preservation between PN, cryoablation, and radiofrequency ablation using 3D volume measurements. They concluded that radiofrequency ablation or cryoablation was associated with less renal parenchymal loss than PN in the management of small renal masses.
Computer-based 3D volume segmentation of tomographic data allows the use of multiple tools that can be used to calculate and interpret 3D images at a level of understanding unachievable through the analysis of a series of two-dimensional serial sections. This digital approach facilitates the interactive visualization of anatomical structures and their relationships. Especially in kidney cancer, detailed examination of the tumor and its relationship with other structures are very important for surgeon before PN. Also, it could be used for prediction of surgery complexity with an accurate calculation of tumor diameter and RENAL nephrometry score. In 2014, Durso and colleagues 16 have used this method to determine kidney volumes and compared it with conventionally available methods. They concluded that 3D provided a highly reliable way of assessing kidney volumes and clinically useful tool for urologists looking to improve patient care using analysis related to volume.
Limitations of this study include its retrospective nature, reliance on GFR estimation from serum creatinine, and the presence of compensatory function from normal contralateral kidneys in most patients. Studies would ideally include only patients with a solitary kidney and/or direct GFR measurement of affected kidney using separate renal scintigraphy.
Conclusion
Of all the factors analyzed, RENAL score and Charlson comorbidities index were the most accurate predictor of postoperative parenchymal loss. Also, the percent decrease in GFR at late time points was associated with renal volume preservation, and quality of the remnant parenchyma. There was a negligible impact of limited warm ischemia on late percent GFR decrease, but patients with older age and renal insufficiency are subgroups that need attention. New techniques that optimize tissue preservation may be an option for patients with older age or high medical comorbidities.
Footnotes
Authors' Contributions
Conception and design: M.E., H.A.A., H.B., R.B.D., and L.C.; Acquisition of data: M.E., H.A.A., H.B., S.O., L.C., and O.C. Analysis and interpretation of data: M.E., H.A.A., R.B.D., and O.C.; Final approval of the completed article: M.E., H.A.A., S.O., L.C., and O.C.
Disclosure Statement
No competing financial interests exist.
Funding Information
No research support or funding was received in connection with this study. The authors have no significant affiliation or involvement, either direct or indirect, with any organization or entity with a direct financial interest in the subject matter or materials discussed.