
Abstract
After surgical resection for Crohn's disease (CD) endoscopic recurrence is noted within few weeks and almost 80% of patients will have evidence of endoscopic recurrence at the anastomosis after ileocolic resection at 1 year. With time and if left untreated surgical recurrence will be detected at the preanastomotic segment or at the anastomosis in the vast majority of cases. It has become progressively apparent also based on these historical data that anastomotic configuration plays a major role in the subsequent recurrence of CD in surgically induced remission. In this article, we will review the evidence in the literature to support the different anastomotic configurations and we will discuss the principles of surgical prophylaxis of CD recurrence.
Background
Despite the remarkable advancements in the medical management of Crohn's disease (CD), it is estimated that about half of the patients will require a surgical intervention during their lifetime, with up to 30% eventually requiring a second procedure.1,2 Although several bowel sparing approaches have been developed, most index operations will involve a segmental bowel resection with anastomosis. 2 For many decades, surgeons have attempted to identify the ideal anastomotic technique, namely the one reliably associated with the lowest immediate postoperative complications and long-term recurrence rates. There are multiple technical aspects involved in the construction of a bowel anastomosis, including anastomotic technique and intestinal configuration.
Handsewn Anastomoses
There are no high-quality data suggesting the superiority of any sewing technique. A recent retrospective study looking at the outcomes of 347 handsewn colonic anastomoses found a lower risk of anastomotic leak (2.5% versus 16%, respectively; P = .001) and shorter hospital stay (16 ± 11 versus 23 ± 15 days, respectively; P < .001) with continuous versus interrupted sutures. However, <10% of the patients included had inflammatory bowel disease. 3
Regarding suture material, data from experimental studies suggest that nonabsorbable or slowly absorbable monofilament materials are better suited for intestinal anastomoses as they create more tissue reaction and dissolve slowly, thus improving anastomotic strength. However, there is no good quality clinical data to support the superiority of any type of suture.4–9 Based on the results from one randomized controlled trial, placing the stitches 5–10 mm from the cut edge seems adequate to achieve optimal results and, despite the scarce level of evidence, seromuscular and full-thickness bites are equivalent in ensuring the lowest rates of anastomotic leaks.10–15 According to evidence present in the literature, single-layer anastomosis are noninferior to double-layer, are faster and cheaper to perform, and, in colorectal anastomoses, may be less prone to leakage.16–18 Finally, no high-quality study has been published documenting any difference in outcomes between interrupted versus continuous sutures, hence the choice is mostly dictated by surgeon's preference. 19
Stapled Anastomoses
Since the introduction of intestinal stapling devices more than six decades ago, many studies have been published comparing the outcomes of stapled versus handsewn anastomoses in colorectal surgery, with somewhat conflicting results.20–25 Over the course of the years, the large amount of data accumulated on this topic was pooled into several meta-analyses, mostly showing comparable results between the two techniques in terms of short-term morbidity and mortality.26–28 In a Cochrane review by Choy et al. 29 examining anastomotic outcomes after right-sided resections, handsewn anastomoses were associated with significantly overall higher leak rates; when symptomatic leaks only were considered, this difference did not persist. In addition, no differences were noted in anastomotic leak rate in patients with nonmalignant disease, including CD. 29 An intriguing finding was reported by Friend et al. who documented that handsewn anastomoses led to higher leak rates compared with stapling when the anastomoses were performed by trainees, suggesting that in less experienced hands, stapled techniques may be more reliable. 30 This is an important point when looking at large population-based studies, taking into consideration that hand-sewing is not as extensively applied or taught.
When looking specifically at outcomes in CD patients, there is conflicting data regarding whether stapled side-to-side functional end-to-end anastomoses might be associated with less postoperative complications as well as lower rates of clinically significant recurrences compared with handsewn anastomoses.31,32 In an Italian retrospective review, leak rate after ileocolic resection for CD was 2.0% in the side-to-side stapled group versus 14.1% in the end-to-end handsewn group (P = .02), although the overall leak rate was high compared with the reported literature. 33 Conversely, in a Canadian randomized controlled study comparing the same two anastomotic techniques for ileocolic CD, equivalent rates were found regarding perioperative complications (including leaks) as well endoscopic and symptomatic recurrences. 31 In a meta-analysis of two randomized controlled trials and a total of eight studies, including 661 patients and 712 anastomoses for CD, end-to-end anastomoses were associated with significantly higher leak rates (odds ratio [OR], 4.37; P = .02), overall postoperative complications (OR, 2.64; P < .001), and increased length of stay (weighted mean difference, 2.81; P = .007) when compared with any other anastomotic configuration. There were no significant differences in anastomotic recurrences and reoperation rates. 34 Finally, a meta-analysis published in 2013 including eight studies, of which three were randomized controlled trials, concluded that when compared with handsewn end-to-end anastomoses, stapled side-to-side anastomoses for ileocolic CD results in fewer overall short-term complications and anastomotic leaks, as well as less anastomotic recurrences, including those requiring reoperation. 35
Anastomotic Configurations
In a retrospective study comparing different anastomotic configurations (side-to-side, side-to-end, and end-to-end), either stapled or handsewn based on surgeon's preference, no difference among groups was noted with regard to complications and reoperation for recurrence; however, when grouping the patients by anastomotic technique, the handsewn anastomoses were associated with a lower reoperation rate than the stapled ones (P = .04). 36 The advantage provided by the side-to-side configuration appears to be, at least in part, attributable to the actual size of the anastomotic lumen, as observed in a study by Muñoz-Juárez et al. 37 The wide-lumen side-to-side, functional end-to-end, stapled anastomoses provided a statistically significant reduction in the overall reoperation rate for anastomotic recurrence at 5 years compared with handsewn end-to-end anastomoses. 37
Interestingly, in a recent observational study on 128 patients with CD undergoing bowel resection, the end-to-end reconstruction was associated with significantly less emergency room visits (14.7% versus 33.3%; P = .01), hospital admissions (11.8% versus 30%; P = .01), overall higher quality of life (mean short inflammatory bowel disease questionnaire score 53.4 versus 47.9; P = .007), despite no significant differences in surgical complication and disease recurrence rates when compared with a side-to-side configuration. The side-to-side anastomosis were performed in an antiperistaltic orientation using a stapling device, whereas the end-to-end were handsewn either in a single or double layer. 38
One of the latest developments in surgery for CD is the antimesenteric functional end-to-end handsewn (Kono-S) anastomosis. Initially described by Kono et al., 39 this technique has shown very promising results in dramatically reducing anastomotic recurrence rates in CD patients. Four factors are hypothesized to be responsible for the significant reduction in endoscopic and surgical recurrence rates. The wide lumen of the anastomosis reduces reducing local fecal stasis that has an impact on local proinflammatory microbiota alterations. The added stabilization of the anastomosis provided by the “supportive column” limits luminal distortion. The isolation of the mesentery from the anastomotic lumen; the mesentery is known to be the site of early evidence of primary and recurrent disease. Finally, preservation of innervation and vascularization due to the limited mesenteric resection.39–41 The specific technical details of this technique will be discussed as follows. The recently published SuPReMe-CD randomized controlled trial confirmed the favorable outcomes observed in several previously published international retrospective series. The Kono-S reconstruction was associated with less endoscopic recurrences at 6 months (22.2% versus 62.8%, P < .001), fewer clinical recurrences at 24 months (18% versus 30.2%, P = .04), and longer interval until recurrence (P = .037) compared with stapled side-to-side anastomosis. The Kono-S anastomosis was the only independent predictor of decreased endoscopic recurrence rates. 42
The principles of mesenteric preservation of the Kono-S anastomosis seem to be in contrast with the concept of wide mesenteric excision recently popularized by Coffey et al. 43 In their study, they observed a remarkable reduction in reoperation rates in patients undergoing wide mesenteric excision when compared with those where the mesentery was divided close to the bowel wall (2.9 versus 40, respectively; P = .003). These results have yet to be reproduced by other investigators. Although this approach seems in striking opposition to the more validated Kono-S technique, they do share an important aspect, which is “protecting” the anastomosis from the mesentery, in one case by removing the adjacent segment, in the other by interposing the “supporting column.”
Relevant Factors in Choosing an Anastomotic Configuration and Technique
In CD, given the heterogeneity of the clinical presentations, the choice of the anastomotic technique and configuration is left to the surgeons' judgment, skills, and expertise given the paucity of disease-specific high-quality evidence. The authors utilize the following experience-based principles when assessing a patient in the operating room for an anastomosis:
CD should always be considered a pan-intestinal disease. The bowel wall even in normal appearing segments is not comparable with the bowel wall of patients with malignant and non-inflammatory bowel disease benign conditions in terms of ability to hold sutures or staples and to heal an anastomosis. As an example, a segment of bowel proximal to a chronic stricture will be dilated and often thickened, whereas distal to it will be decompressed. In addition, these patients are often malnourished and immunocompromised. Finally, the effects of several classes of drugs, including corticosteroids on postoperative septic complications have been extensively studied. All these factors demand meticulous technique and attention to details. Despite the mixed evidence in the literature, we do believe that a wide lumen anastomosis with limited impediment of the enteric flow will have long-term benefits on endoscopic and surgical recurrence rates.37,44 The anastomosis has been shown to be the most likely site of postoperative recurrence.
45
We believe that impairment of fecal flow at the anastomotic site results in local host-microbiota imbalance.
46
Preservation of innervation and vascularization at the anastomotic site will result in maintained peristaltic wave progression and lower incidence of anastomotic stenosis in the early postoperative period.
47
The mesentery is the early site of primary and recurrent disease demonstrated both clinically and from a cytokine production perspective.
48
Exclusion of the mesentery from the anastomosis intuitively will have a beneficial effect on endoscopic and surgical recurrence rates. In our opinion the anastomotic configuration and technique that more closely follows these principles (wide lumen, handsewn, exclusion of the mesentery, and preservation of vascularity and innervation) is the Kono-S anastomosis.
Technical Steps of the Kono-S Anastomosis
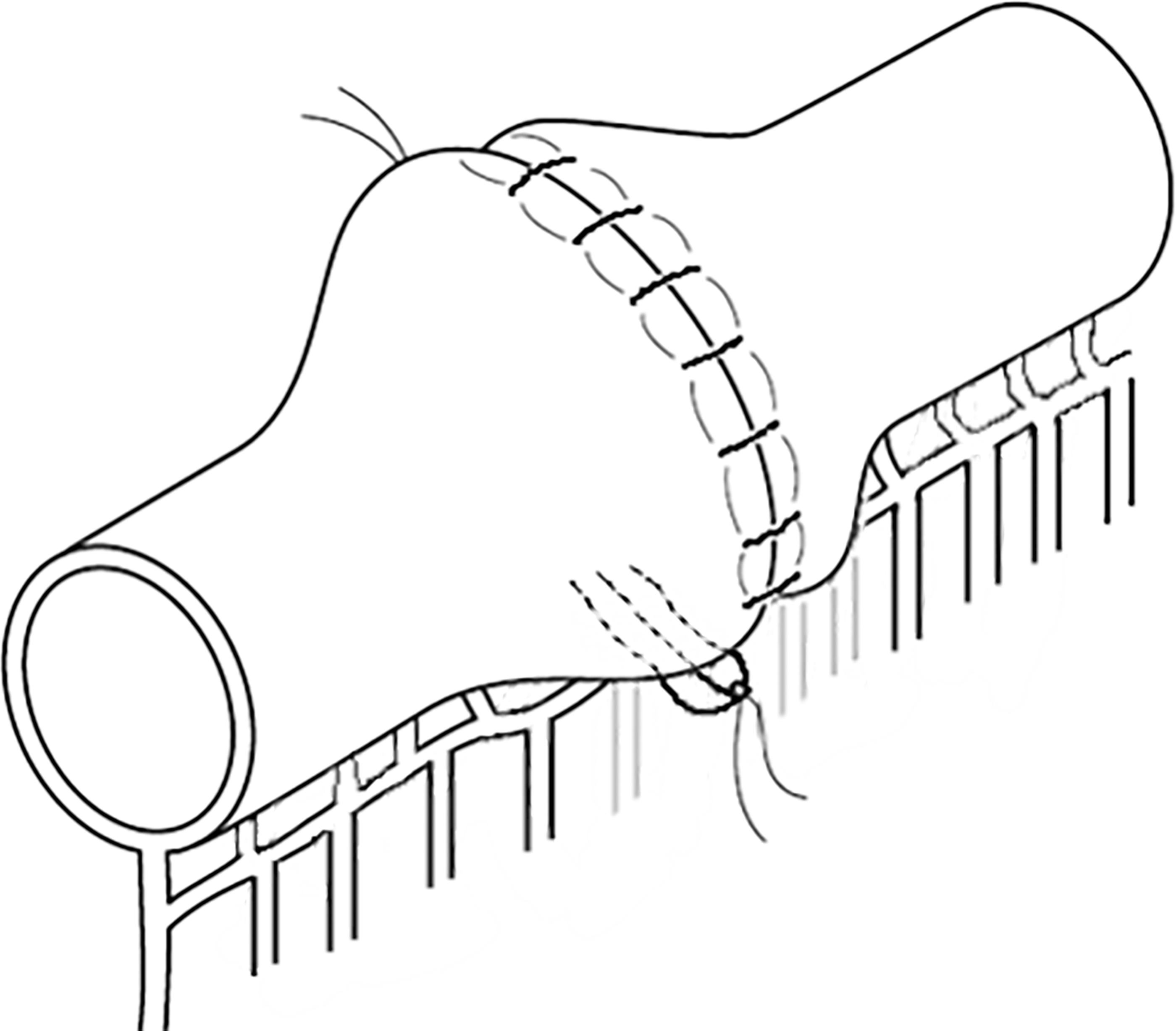
After identification of the involved segment, the bowel is divided with a stapling device with the mesentery perpendicular to the staple line. The intervening mesentery is transected close to the bowel wall to preserve innervation and vascularity. The two staple lines are sewn together with nonabsorbable sutures to construct the supporting posterior column (Fig. 1). In the event of size discrepancy between the two loops the difference is distributed along the staple lines. Longitudinal enterotomies are performed starting at 1 cm from the staple line and extending proximally and distally to allow a 7 cm transverse lumen (Fig. 2). The enterotomy should start <1 cm from the staple to avoid ischemia of a shorter segment and it may extend for up to 8 cm especially on the colon. The enterotomies are then sewn together in two layers in a transverse manner using 3-0 Vicryl running Connell sutures and 4-0 silk Lembert sutures (Fig. 3).

Creation of the supporting column. Longitudinal enterotomies starting at 1 cm from the staple line.

The enterotomies should result in a transverse lumen of 7 cm.
Completed two layers anastomosis.
Conclusions
In CD, given the variability of clinical scenarios, clinical judgment, experience, and skills play a major role at the time of critical intraoperative decisions. It is safe to say that we should approach every CD patient as a unique case. The authors have elucidated their thought process and algorithmic decision making based on the limited high-quality scientific evidence and their personal experience.
Footnotes
Disclosure Statement
The authors have no disclosures.
Funding Information
No funds, grants, or support received to complete the study.