
Abstract
Background:
Given the importance of operative documentation, we reviewed operative notes for surgeries that required splenic flexure mobilization (SFM) to determine their accuracy.
Materials and Methods:
We performed a retrospective review of 51 operative notes for complete SFMs performed at a single institution from January 2015 to June 2020.
Results:
None of the operative notes reported a rationale for performing SFM, use of preoperative imaging to guide technical approach, reasoning for the operative method and mobilization approach used, or specific steps taken to ensure that SFM was done safely. Most reports did not include technical details, with one-third of the notes merely reporting that “the splenic flexure was mobilized.”
Conclusions:
Increased awareness about the lack of operative documentation of the critical aspects of the SFM could stimulate initiatives to standardize the SFM method and improve the quality of operative notes for SFM.
Introduction
The splenic flexure mobilization (SFM) is considered one of the most technically challenging procedures in colorectal surgery.1,2 The difficulty in mobilizing the splenic flexure is related to its high location in the left upper quadrant near the spleen and proximal to the costal margin. Furthermore, the embryological development of the splenic flexure results in its fixation to several surrounding structures, making its mobilization challenging.
Because of the anatomic complexity of the splenic flexure, its mobilization is not without risks. SFM is associated with iatrogenic injuries to the spleen as well as to adjacent structures such as mesentery, bowel, and pancreas.3,4 Furthermore, complications related to the SFM are associated with prolonged operating time, worse postoperative outcomes, increased length of hospital stay, and higher mortality.5,6
Although multiple approaches for SFM are used, a standardized SFM method has yet to be developed, reflecting the challenges that exist in understanding the embryology of the splenic flexure and performing its mobilization. Importantly, in the absence of a standardized SFM approach, explicit guidelines for the content of SFM in operative notes would be difficult to develop.
Operative notes are expected to accurately document the details of every operation and are essential for patient care. 7 Furthermore, they are important for quality assurance, medicolegal cases, research, and education.8–11 Despite their acknowledged importance, operative notes often lack critical aspects of the procedure.12–14
The purpose of this study was to review operative notes for surgeries that required SFM, to determine how frequently they contained a clear description of the key technical steps of the SFM. Additionally, based on a review of the SFM literature, we aim to propose guidelines on the important elements that operative notes describing SFM should contain to accomplish its goals.
Methods
After an institutional review board exemption was granted, we retrospectively reviewed the operative notes for all colorectal surgeries with complete SFM that were performed at our institution over a 5-year period (January 2015–June 2020).
The presence of the description of the following six elements of the SFM was analyzed:
Preoperative assessment of the anatomic location of the splenic flexure Operative method (open, laparoscopic, or combined) Reasoning for choice of operative method SFM approach (anterior, lateral, medial, or combined) Reasoning for choice of SFM approach Preventive measures to avoid injury to the spleen and the surrounding structures
We also conducted a retrospective chart review to identify patient demographics, indications for the surgery, and intraoperative and early postoperative complications.
All operative notes consisted of narrative reports. Patient information and the name of the surgeon were anonymized before data were analyzed. From the operative notes, the full text of SFM as described by surgeons were recorded verbatim and no attempt was made to read between the lines.
Nonparametric data were analyzed using Fisher's exact and Mann–Whitney U tests. Statistical significance was set at P < .05.
Results
Between January 2015 and June 2020, 51 patients underwent colorectal surgery with complete SFM at the Veterans Affairs Boston Healthcare System.
The median (range) age of patients at the time of the operation was 64 (33–91) years. Most patients were males (48 [94.1%]), with only 3 (5.9%) female patients. The median body mass index (BMI) of patients was 27.7 (range 19.2–40.1) kg/m2. Patient primary diagnoses, operations performed, and operative approaches are shown in Table 1.
Patient Primary Diagnoses, Operations Performed, and Operative Approaches
Intraoperative splenic injuries occurred in 5 (9.8%) patients, with all injuries consisting in capsular tear or avulsion. Four of the five splenic injuries occurred during open procedures, whereas one injury required conversion from laparoscopic to open surgery. All splenic capsule injuries were successfully managed with electrocoagulation, packing, and application of hemostatic agents.
Other intraoperative complications occurred in 10 (19.6%) patients and included colorectal anastomosis leak (2), bladder injuries (2), left diaphragmatic injury requiring primary repair (1), left pneumothorax (1), gastric perforation (1), proximal transverse colon perforation (1), ischemia of the colon splenic flexure requiring unplanned resection (1), and rectal injury (1).
Early postoperative complications occurred in 16 (31.4%) patients and included ileus (7), anastomotic breakdown requiring reoperation (3), superficial surgical-site infection (2), deep surgical-site infection (1), wound dehiscence requiring reoperation (1), myocardial infarction (1), and deep vein thrombosis (1).
The analysis of description of the key SFM procedural elements in operative notes is shown in Table 2. Although preoperative computer tomography imaging was obtained in all patients, no operative report describes an assessment of the anatomic location of the splenic flexure to estimate the level of SFM difficulty and make appropriate procedural plans.
Description of Splenic Flexure Mobilization Procedural Steps in Operative Notes
SFM, splenic flexure mobilization.
Reasoning for surgeon's choice of the operative method (open, laparoscopic-to-open conversion, or laparoscopic) is described only for the six laparoscopic-to-open conversions, and includes presence of significant intra-abdominal adhesions (3), inability to locate colonic mass laparoscopically (1), occurrence of a gastric perforation (1), and inability to control bleeding from splenic injury laparoscopically (1).
Description of both SFM approach (anterior, lateral, medial, or combined) and the reasoning for its choice is missing from all operative notes. Furthermore, no operative report describes any preventive measures taken to avoid injury to the spleen and the surrounding structures.
The range of SFM details contained in operative notes is illustrated by verbatim descriptions in Table 3. In one-third of operative notes, there was no SFM description and surgeons only reported that “the splenic flexure was mobilized.” Half of operative notes contained no specific details of the SFM technique, whereas seven notes had only minimal details and described the division of only one splenic attachment (splenocolic or pancreatocolic).
Verbatim Descriptions Illustrating the Range of Splenic Flexure Mobilization Details Contained in Operative Notes
SFM, splenic flexure mobilization.
Only one operative note contained moderate technical details by describing the division of two splenic attachments (gastrocolic and splenocolic) as well as delineating a combined (anterior + lateral) SFM approach, without specifically reporting the approach type.
Discussion
To the best of our knowledge, this is the first study to evaluate operative notes of SFM, which represents one of the most challenging steps of many colorectal surgeries. We found that none of the operative notes in our sample reported a rationale for performing SFM, use of preoperative imaging to guide technical approach, reasoning for the operative method and mobilization approach used, or specific steps taken to ensure that SFM was done safely. Furthermore, of the operative reports that state SFM was performed, most did not elaborate on the technical details, with one-third of the notes merely reporting that “the splenic flexure was mobilized.”
SFM is a complex procedural step used in several colorectal operations involving the transverse colon, descending colon, and sigmoid colon. Clinical and cadaveric studies show that SFM increases the colonic redundancy and achieves about 28 cm of additional colon length, as measured from the sacral promontory toward the pelvis.15–17 This increased colonic mobility afforded by SFM is very important not only for creating a well-perfused, tension-free anastomosis and performing a pouch reconstruction when necessary, but also for achieving adequate oncological resection. 18
However, this mobilization is not without risks, as the splenic flexure is embryologically and anatomically complex with attachments to the spleen, stomach, and other surrounding structures. The most frequently noted complication of SFM is splenic injury, with rates of iatrogenic splenic injury in transverse and left hemicolectomies (operations in which SFM is often performed) ranging from 1% to 8%.19–21 Some of the risk factors for iatrogenic splenic injuries during colorectal surgery are open surgery, male gender, peripheral vascular disease, malignant neoplasia, diverticulitis, emergency surgery, teaching hospital status, and type of the procedure (transverse colectomy has the highest risk, followed by left colectomy and total colectomy).4,22 In line with this evidence, in our study, we found a 9.8% rate of splenic injury, all of which were capsular tears or avulsions.
Due to the challenging technical nature of splenic mobilization and the risks associated with it, we propose that surgeons follow a systematic approach preoperatively and intraoperatively with clear documentation of that approach to ensure the most favorable outcomes:
Preoperative assessment
Preoperative assessment of the anatomic location of the splenic flexure is important for advanced preparation for the difficulty of the SFM. In our study, we found that all the patients had preoperative computer tomography imaging, but none of the operative reports mentions a preoperative evaluation of the splenic flexure. Meecham et al. 23 describe a system by which the splenic flexure can be reproducibly assessed, using the Shrewsbury Splenic Flexure Siting (SSFS) system. They propose that the difficulty of SFM correlates with the height and laterality of the flexure. The authors found that observers could consistently site the splenic flexure using computer tomography imaging. Surgeons could use and document a technique such as the SSFS to evaluate the splenic flexure and a specific plan for its mobilization.
Other studies have used computer tomography to analyze the location of the splenic flexure in relationship to the splenic hilum and the lower pole of the spleen.24,25 Taken together, this evidence supports the importance of preoperative understanding of the anatomical location of the splenic flexure for performing a safe SFM.
The operative method is another important factor to consider when planning the mobilization of the splenic flexure. Laparoscopy has been shown to have fewer splenic injuries than open surgery.5,19,21,22,26 We had similar results with four of five splenic injuries occurring in open operations. Furthermore, when compared with open surgery, the laparoscopic approach is associated with a lower need for splenectomy as most iatrogenic splenic injuries can be managed with spleen-preserving approaches. 27 The advantages of laparoscopy may be due to better exposure and visualization of the colon, spleen, and its attachments; tail of pancreas; and lesser sac. Furthermore, as the laparoscopic instruments can be easily moved in the left upper quadrant, the splenic attachments can be divided without applying excessive traction. On the other hand, the splenic flexure may be challenging to visualize with an open approach and may require significant traction to the splenic attachments, increasing the risk of splenic injury.
Hand-assisted or laparoscopic-assisted SFM are some other operative methods that can be used in a patient with high BMI, bulky disease, or a hostile abdomen. 28 These methods combine the advantages of both laparoscopic surgery and conventional open surgery.
They may shorten operative times, avoid a supraumbilical extension of the incision, and allow a greater proportion of patients to undergo a minimally invasive SFM.29–32
While the rationale for choosing between open and laparoscopic method for SMF varies depending on surgeon experience and patient factors, surgeons should comment on their decision in their operative notes as well as consider laparoscopic approaches whenever possible.
Operative technique
The different ligaments that are divided to achieve a complete SFM are phrenocolic, splenocolic, pancreaticocolic, and gastrocolic (Fig. 1).

The splenic flexure ligaments: phrenocolic, splenocolic, pancreaticocolic, and gastrocolic.
Based on the anatomic route used to enter the lesser omental sac, there are three approaches currently used to mobilize the splenic flexure: an anterior approach (through the gastrocolic ligament), lateral approach (through the lateral side of the lesser sac), and medial approach (between the transverse colon and the pancreas).33,34
For the lateral-to-medial approach, the colon is gently retracted medially, an incision is made along the lateral peritoneal reflection (the white line of Toldt), and the mesocolon mobilized off the retroperitoneum along the Gerota's fascia up to the splenic flexure. Separation of the splenic flexure and opening of the lesser sac is then performed from the lateral side (Fig. 2).
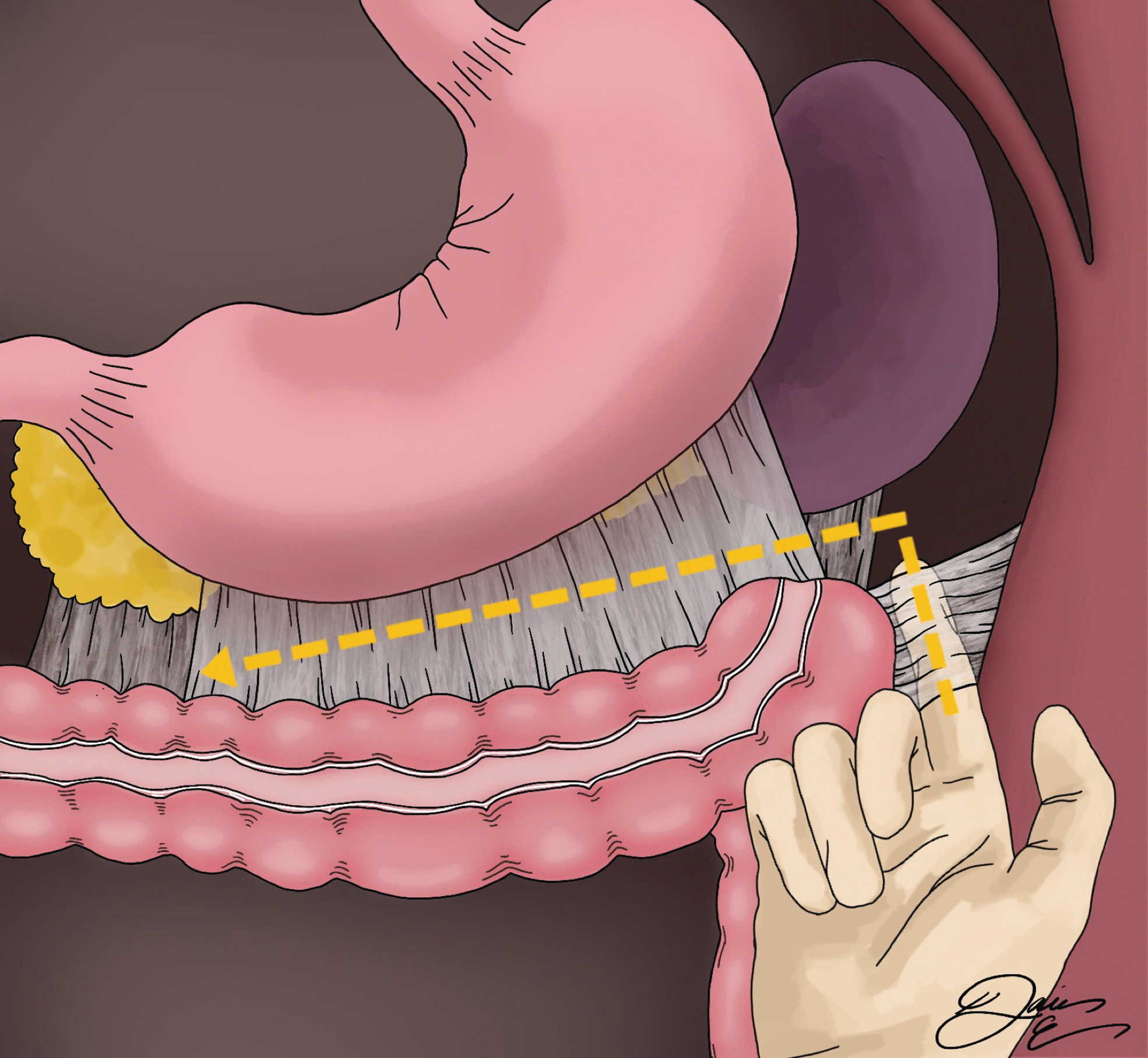
Lateral-to-medial approach for splenic flexure mobilization. The lesser sac is entered from the lateral side after phrenocolic (dotted line) and splenocolic ligaments are divided. The gastrocolic (dotted line + arrow) and the pancreaticocolic are then divided to complete the mobilization of the splenic flexure.
The medial approach begins with a peritoneal incision over the mesentery of the sigmoid colon beneath the trunk of the inferior mesenteric artery and toward the sacral promontory. After the inferior mesenteric artery is divided, the incision is extended to the ligament of Treitz and the anatomic planes above the retroperitoneum are followed cephalad until the inferior mesenteric vein is identified and divided (Fig. 3). After the base of the transverse mesocolon is divided at its origin along the pancreas, the lesser sac is entered followed by mobilization of the splenic flexure from this direction.
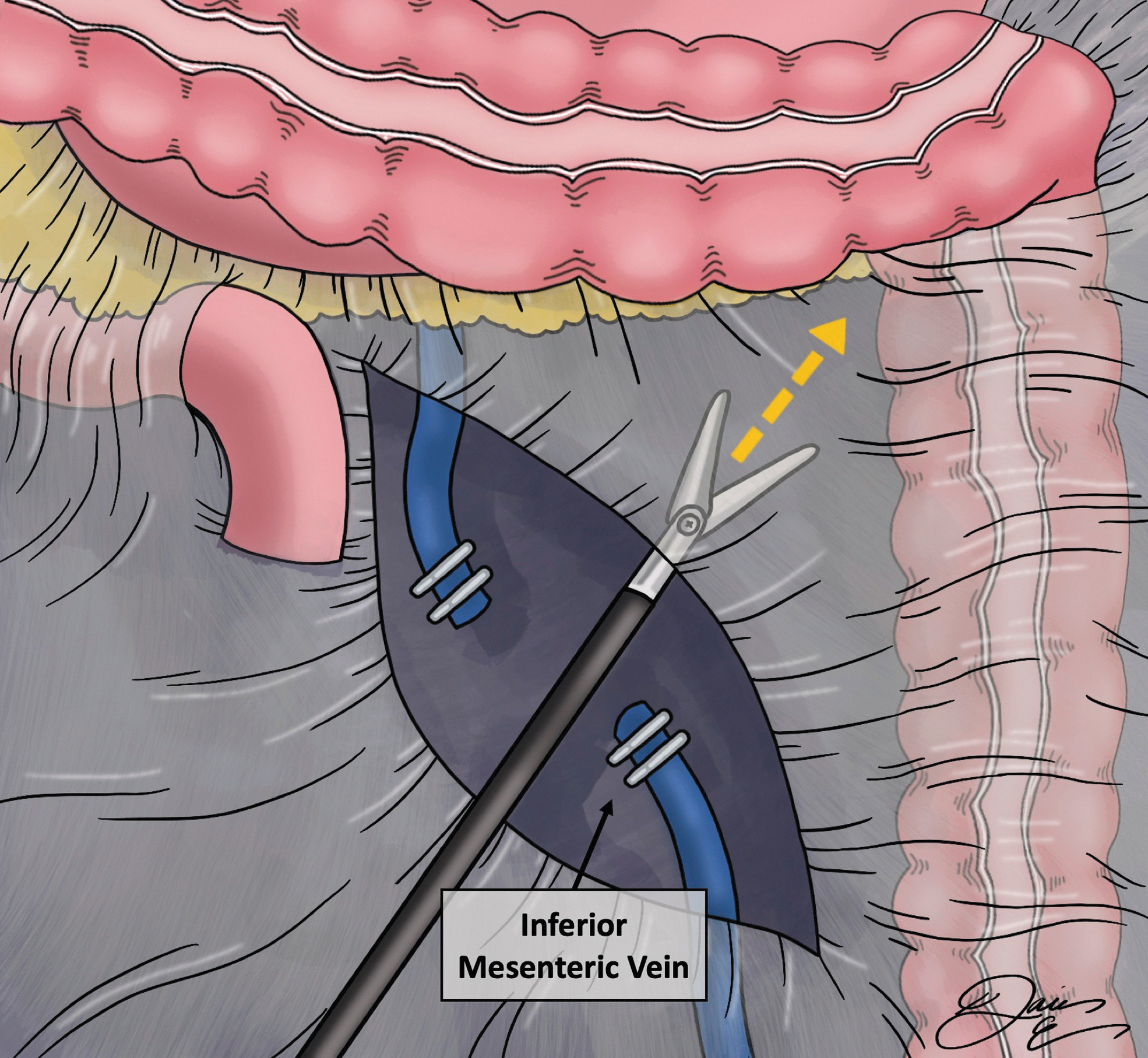
Medial approach for splenic flexure mobilization. After transection of the inferior mesenteric vein (as shown) the base of the transverse mesocolon is divided from this direction (dotted line + arrow).
For the anterior approach, the lesser sac is entered by transecting the midpoint of the gastrocolic ligament at the so-called Bouchet's area, a thin and transparent area on the distal side of the gastroepiploic vascular arch. 35 The lesser sac is then opened toward the splenic flexure and lateral abdominal wall (Fig. 4). After the origin of the transverse colon is incised along the inferior edge of pancreas down, the distal transverse mesocolon and left colon are then mobilized off the retroperitoneum in a caudal direction.
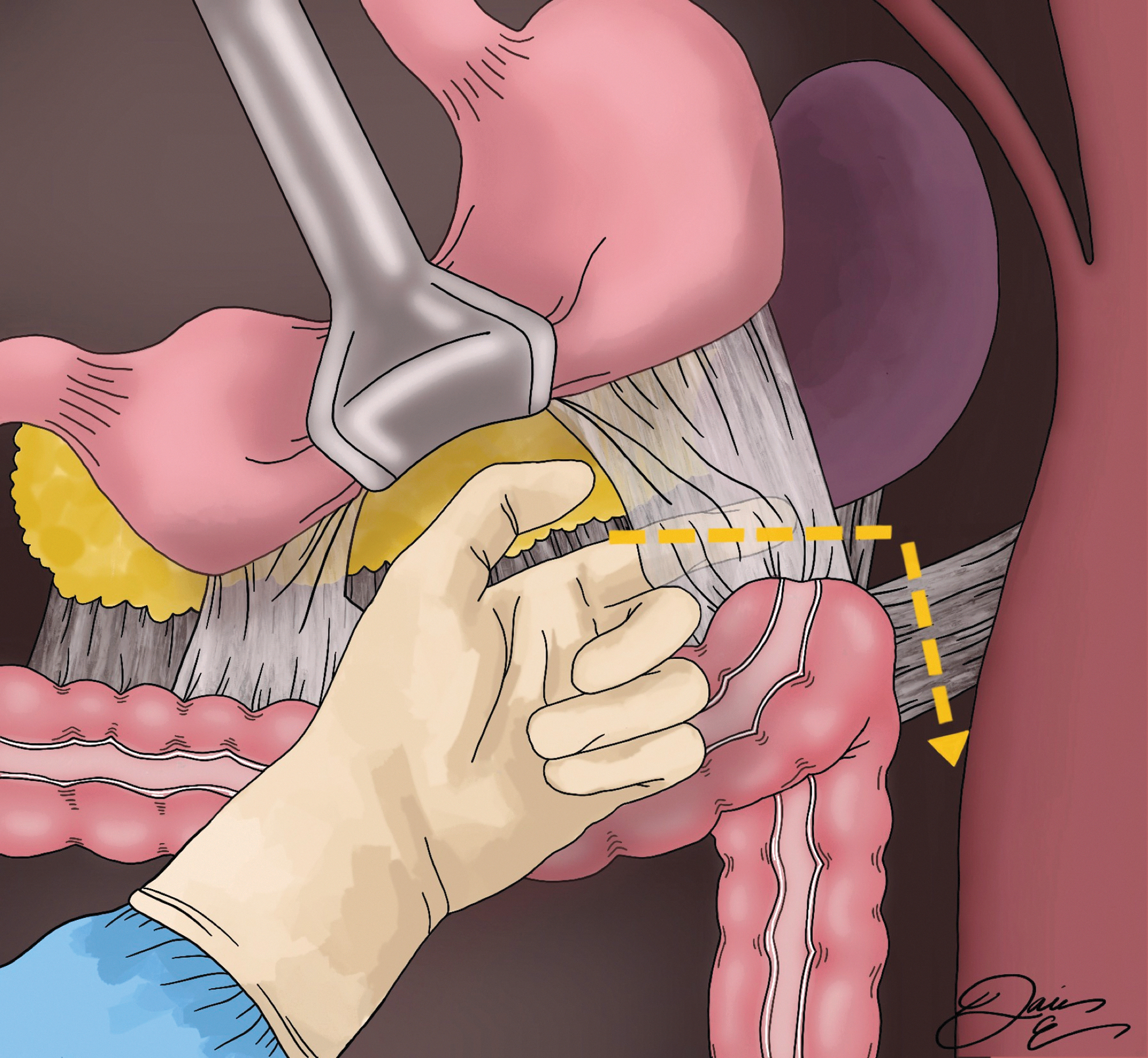
Anterior approach for splenic flexure mobilization. The lesser sac is entered by dividing of the gastrocolic ligament (dotted line) and then opened toward the splenic flexure and lateral abdominal wall until all splenic flexure ligaments are divided.
While each one of the three described approaches for SFM is feasible and safe in experienced hands, there are risk differences according to the approach. Benseler et al. 34 found a lower rate of intraoperative complications (including splenic bleeding), less postoperative complications, a shorter hospital stay, and the highest quality of the resected specimen when the anterior approach was used, likely due to a better visualization of the pancreas and spleen. The conversion rate from laparoscopic to open surgery was significantly higher when the lateral approach was used. 34
The mobilization of the splenic flexure may not be always possible by a single approach, and in some cases a combination of different approaches might become necessary.
Given the approach-associated risks and benefits, the rationale for choosing a specific approach and its technical steps should be clearly described in the operative report. We found, however, that only eight notes in our sample described any of the specific splenic attachments that were divided.
Excessive traction to the attachments of the spleen is the most common cause of iatrogenic splenic injury during SFM.27,36–39 Various techniques to prevent traction injuries to the spleen have been described in the past and they include placement of packs behind the spleen to reduce tension on the splenic attachments, 40 and preliminary division of the gastrohepatic ligament in upper abdominal operations to reduce the traction transmitted on the spleen from the stomach. 41 However, no special technique can substitute for technical accuracy, cautious dissection, adequate visualization, and optimal traction of the splenic attachments during SFM. Therefore, the highest vigilance must be taken to avoid iatrogenic splenic injuries during SFM regardless of the surgical method and approach.
While it is clear from our data that many key elements of the SFM are not included in operative reports, our study is not without limitations. This study was, by nature of reviewing operative notes, a retrospective review. This may have led to a selection bias, as we are only able to identify cases in which SFM was documented, which may not accurately reflect the true number of cases where SFM was performed. This study also only reflects one institution and perhaps institutional culture and precedent plays a role in the details documented in operative reports.
Despite these limitations, our findings raise awareness of the lack of thorough documentation of the key aspects of the SFM. We hope that our work will stimulate initiatives to improve the quality of operative notes for SFM, similarly to how laparoscopic cholecystectomy reporting has been standardized. 42
Conclusions
SFM is a complex procedure with a high risk of complications. Our findings show that the operative notes lack the key elements of the SFM. This has important implications because operative notes are crucial for patient care, quality assurance, medicolegal reasons, research, and education.
Footnotes
Authors' Contributions
Conception and design of study: P.C. and G.K. Acquisition of data: P.C. and G.K. Analysis and/or interpretation of data: P.C., K.H., D.E., A.M., E.W., and G.K. Drafting the article: P.C. and G.K. Revising the article critically for important intellectual content: P.C., K.H., D.E., A.M., E.W., and G.K. Approval of the version of the article to be submitted: P.C., K.H., D.E., A.M., E.W., and G.K.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.