
Abstract
Background/Aims:
Both endoscopic nasobiliary drainage (ENBD) and a plastic stent placement have some limitations in biliary decompression of elderly patients with acute cholangitis of severe type (ACST) due to choledocholithiasis. Dual stent placement may improve bile drainage without obvious discomfort. Here, we evaluated its advantages in the biliary decompression of elderly patients with ACST.
Materials and Methods:
A total of 257 elderly patients (≥65 years) with ACST had undergone urgent endoscopic decompression by nasobiliary catheter (ENBD group), single plastic stent (single-stent group), or dual plastic stents (dual-stent group). The data of the three groups was compared retrospectively.
Results:
The demographic data of the patients in the three groups were comparable. After endoscopic decompression, the serum total bilirubin and γ-glutamyl transferase levels in the dual-stent group were decreased faster than that in the single-stent group (P < .05). The abdominal pain in the dual-stent group was dramatically slighter than that in the ENBD group (P < .05). Compared with two other groups, the acute physiology and chronic health evaluation II scores were decreased dramatically quicker (P < .05) and the length of intensive care unit stay was significantly shorter (P < .05) in the dual-stent group. In the second endoscopic retrograde cholangiopancreatography, the rate of complete stone clearance in the dual-stent group was significantly higher than that in the ENBD group (P < .05).
Conclusions:
Dual-stent placement might be a better choice for elderly patients with ACST due to choledocholithiasis in comparison with ENBD or a single-stent placement.
Introduction
Acute cholangitis of severe type (ACST) is cholangitis with sepsis-induced organ damage. 1 Pus accumulates in the bile duct and causes a severe infection. ACST is a life-threatening disease that should be treated urgently. The International Tokyo Guidelines 2018 (TG18), based on expert opinions, recommend that treatment for the underlying etiology should be provided after the patient's general status has improved. 1 Biliary decompression, but not stone removal, is essential for disease control. 2 Endoscopic biliary decompression has been suggested to be the preferred choice in the urgent treatment of acute suppurative cholangitis (ASC).1,3–5
Both endoscopic nasobiliary drainage (ENBD) and endoscopic retrograde biliary drainage (ERBD) using a plastic stent are effective treatments for patients with ASC. 6 However, both methods have some limitations. Nasobiliary catheters can cause obvious discomfort in patients as well as the loss of electrolytes and fluid. Therefore, they are not suitable for long-term drainage. ERBD using a plastic stent is inefficient in biliary decompression compared with ENBD. 7 The stent can easily block and migrate, and the blockage and migration of the stent cannot be known in real time. 8 The plastic stent cannot be irrigated when it is obstructed.
For some elderly patients with ACST due to choledocholithiasis, after biliary decompression, stone removal is performed after a long waiting period due to poor physical condition and slow recovery. Therefore, compared with young patients, elderly patients with ACST require long-term biliary drainage. In addition, the preferred method for endoscopic biliary decompression has not been clearly defined for elderly patients with ACST in the TG18. Therefore, we attempted to define a preferable method of endoscopic biliary drainage for elderly patients with ACST due to choledocholithiasis.
Since dual-stent placement can improve bile drainage and is an internal indwelling procedure without obvious discomfort, we hypothesized that dual plastic stent placement might be a better choice for elderly patients with ACST. Although dual-stent placement has been used for acute cholangitis, its advantages have not been well defined. We, therefore, compared the effectiveness and safety of dual plastic stent placement with nasobiliary drainage and single plastic stent placement in elderly patients with ACST due to choledocholithiasis.
Patients and Methods
This study was approved by the institutional ethics review committee (NO2020-437).
Patients
From January 2013 to May 2020, a total of 257 elderly patients (≥65 years old) were diagnosed with ACST due to choledocholithiasis at admission and underwent urgent endoscopic biliary decompression in our hospital. The diagnosis of ACST was defined as acute cholangitis with the presence of organ dysfunction. 9 The data of patients with ACST who had successfully undergone the endoscopic retrograde cholangiopancreatography (ERCP) procedure were collected. Patients with biliary malignancies and coexisting intrahepatic stones were excluded. Patients who could not finish the ERCP procedure were also excluded. Imaging methods were used to show evidence of obstruction of the bile duct secondary to choledocholithiasis. These patients were divided into the ENBD group (n = 105), the single-stent group (n = 78), and the dual-stent group (n = 74) according to biliary decompression. The data of these patients in the three groups were collected and compared retrospectively.
ERCP procedures and medical treatments
All of the ERCP procedures were performed by professional endoscopists (annual ERCP volume of more than 400 cases). Endoscopic biliary drainage was performed after an initial treatment to maintain homeostasis and respiratory/circulatory management. Before the procedure, the patients were introduced to the advantages and disadvantages of the three types of biliary decompression. Patients who were irritable and could not cooperate with the procedure were not recommended for ENBD in consideration of a high rate of unplanned extubation. Every patient could choose a type of biliary decompression and provided written informed consent for the procedures and treatments.
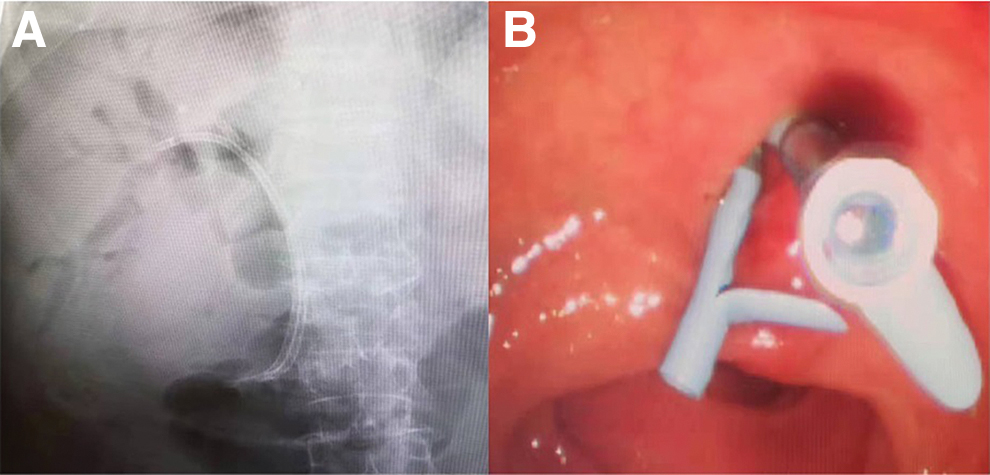
Patients received an injection of diazepam and meperidine for conscious sedation and analgesia and oral intake of lidocaine hydrochloride mucilage for local anesthesia. The ERCP procedures were performed by using a conventional therapeutic duodenoscope (ED34-i10T; PENTAX, Tokyo, Japan). Endoscopic sphincterotomy (EST) was routinely performed except for patients who underwent anticoagulant treatment and patients with coagulopathy (international normalized ratio >1.5, partial thromboplastin time greater than twice that of the control) or a platelet count <50,000 × 103/μL. After successful cannulation of the common bile duct, the bile was sucked out first, and then low-osmolar nonionic contrast medium was carefully injected to confirm the etiology of cholangitis, the diameter and the number of stones, and the internal diameter of the common bile duct. The stones were not removed at the initial procedure due to the poor physical condition of the patients. The patients were implanted with nasobiliary catheters (7.5F; Boston Scientific, USA) in the ENBD group or biliary stents (8.5F; Boston Scientific) in the single-stent group and the dual-stent group. The method of endoscopy decompression was mainly dependent on the patient's decision. For endoscopic biliary decompression with dual plastic stents, plastic stents were implanted into different hepatic lobe bile ducts. Pictures of dual stent placement are shown in Figure 1. Pancreatic stenting (5F; ENDO-FLEX, Germany) was used to prevent post-ERCP pancreatitis (PEP) in patients with high-risk factors.10,11
The X-ray perspective film
All of the patients were admitted to the surgical intensive care unit (ICU) for postoperative treatments, including antibiotics and somatostatin. The output of the nasobiliary catheter in the ENBD group was monitored, and the nasobiliary catheter was irrigated when it was obstructed.
The clinical data of each patient in the first week after the procedure were collected. The time to ERCP was defined as the time from admission to the commencement of the ERCP. Complications, including bleeding, displacement, and PEP, were recorded and compared among the three groups. The displacement of the nasobiliary catheter and stent in this study was defined as the catheter or the stent migrating from the bile duct completely. PEP was defined as abdominal pain, with at least a threefold elevation of serum amylase more than 24 hours after the procedure that required treatment for more than 2 days. 5 Serum total bilirubin (TBIL), serum γ-glutamyl transferase (GGT), and total leukocyte counts were assessed. The face pain ranking scale was used for the assessment of abdominal pain, and the acute physiology and chronic health evaluation II scoring system (APACHE II score) was used to assess the severity of disease. 12 The length of ICU stay was also recorded for each patient.
All of the patients were followed up after the procedures. They were recommended to undergo a second ERCP for the removal of stones on schedule. Usually, the time for stone removal in the ENBD group was 7–14 days after the previous ERCP, whereas that in the single- or dual-stent placement group was 3 months after the previous ERCP. The success rate of stone removal at the second ERCP was compared among the three groups. Further treatments and long-term complications, including blockage, displacement, and unplanned extubation, were also recorded. The blockage of dual stents was defined as the blockage of both stents.
Statistical analysis
All of the statistical analyses were performed with SPSS statistics software, version 21 (IBM, USA), or GraphPad Prism software, version 5.0 (La Jolla, CA, USA). Quantitative data are expressed as the mean ± standard deviation. The significant differences between two groups were assessed by the independent-sample t-test, and the significant differences among three groups were assessed by one-way analysis of variance. Categorical data were analyzed with the χ 2 test or Fisher's exact test. P < .05 was considered statistically significant.
Results
Clinical characteristics of the patients
The patients were divided into three groups: the ENBD group (n = 105), the single-stent group (n = 78), and the dual-stent group (n = 74). The clinical characteristics of the enrolled patients in each group are shown in Table 1. There were no significant differences in the clinical characteristics of the patients in the three groups.
Clinical Characteristics of the Enrolled Patients Undergoing Endoscopic Biliary Drainage
APACHE II score, acute physiology and chronic health evaluation II scoring system; CBD, common bile duct; ENBD, endoscopic nasobiliary drainage; ERCP, endoscopic retrograde cholangiopancreatography; GGT, γ-glutamyl transferase; PT-INR, prothrombin time-international normalized ratio; SD, standard deviation.
Endoscopic findings
The endoscopic findings are shown in Table 2. The operation time was similar in the three groups (ENBD group versus single-stent group versus dual-stent group: 20.21 ± 5.38 minutes versus 19.07 ± 4.86 minutes versus 20.72 ± 4.75 minutes; P > .05). EST was not performed in 56 patients: 27 in the ENBD group, 15 in the single-stent group, and 14 in the dual-stent group. Pancreatic stenting was performed in 27 patients: 11 in the ENBD group, 7 in the single-stent group, and 9 in the dual-stent group. Overall, no significant differences were found in endoscopic findings among the three groups (P > .05).
Endoscopic Finding in Endoscopic Retrograde Cholangiopancreatography Procedures
ENBD, endoscopic nasobiliary drainage; EST, endoscopic sphincterotomy; SD, standard deviation.
The effectiveness of endoscopic decompression in the three groups
To compare the effectiveness of the three endoscopic drainage methods, TBIL, GGT, total leukocyte count, pain rating index, APACHE II scores, and length of ICU stay were compared among the three groups (Fig. 2). The TBIL level was lower in both the ENBD group and the dual-stent group than in the single-stent group at 3 and 5 days after the procedure (P < .05). The GGT level was lower in the ENBD group at 5 and 7 days after the procedure and in the dual-stent group at 3, 5, and 7 days after the procedure compared with the single-stent group (P < .05). No significant difference was found between the ENBD group and the dual-stent group in the decrease in TBIL and GGT (P > .05). The total leukocyte count was decreased in each group after the procedure, and no significant difference was found among the three groups (P > .05). The abdominal pain of the patients in the single-stent group and the dual-stent group was much less severe than that in the ENBD group after the procedure (P < .05), and no significant difference was found in abdominal pain between the single-stent group and the dual-stent group (P > .05). The APACHE II scores of the patients in the dual-stent group decreased much more rapidly than those in the other two groups at 1 day after the procedure (P < .05). The mean length of ICU stay was 3.02 ± 0.35 days for the ENBD group, 3.41 ± 0.66 days for the single-stent group, and 1.98 ± 0.23 days for the dual-stent group. A significantly shorter ICU stay was found in the dual-stent group (P < .05).

Comparison of serum total bilirubin level
Adverse events of endoscopic decompression
To compare the safety of the three endoscopic drainage methods, complications and mortality were compared among the three groups (Table 3). The occurrence rate of adverse events was 10.12% in all of the patients. There was no significant difference in bleeding or catheter (or stent) displacement at 7 days after previous ERCP or PEP among the three groups (P > .05). Among the patients without EST, 2 patients (7.41%) in the ENBD group, 1 patient (6.67%) in the single-stent group, and 2 patients (14.29%) in the dual-stent group suffered from PEP (P > .05). The total mortality was 2.33%, and no significant differences were found in fatalities among the three groups (P > .05). Among these deaths, 5 died of multiorgan dysfunction due to ACST, and 1 died of ventilator-associated pulmonary infection.
Complications and Fatalities in the Three Groups
ENBD, endoscopic nasobiliary drainage; PEP, post-endoscopic retrograde cholangiopancreatography pancreatitis.
Follow-up of the patients
A total of 101 patients in the ENBD group, 75 in the single-stent group, and 72 in the dual-stent group underwent a second ERCP to remove stones on schedule. Four patients in the ENBD group, 3 patients in the single-stent group, and 2 patients in the dual-stent group died after the initial ERCP without a second ERCP for stone removal. Two patients in the ENBD group had unplanned extubation before the removal of stones on schedule. One patient was found to have displacement of the catheter, and 1 patient was found to have blockage of the catheter in the ENBD group at the time of the second ERCP. The rate of complete stone clearance in the second ERCP was 85.15% (87/101) in the ENBD group—much lower than 93.33% (70/75) in the single-stent group, and 95.83% (69/72) in the dual-stent group (P < .05). Three patients in the ENBD group with difficult stones and incomplete stone removal at the second ERCP underwent stent placement. The other patients with incomplete stone removal underwent a third ERCP, and the stones were completely removed.
The long-term complications between the single-stent group and the dual-stent group were also compared. At 3 months after previous ERCP, the occurrence rate of stent displacement was 3.85% (3/78) for the single-stent group and none for the dual-stent group (P > .05). The blockage of these removal stents was checked. The occurrence rate of stent blockage in the single-stent group was 18.67% (14/75), which was significantly higher than the 2.70% (2/74) rate in the dual-stent group (P < .05). Three patients in the single-stent group had a recurrence of cholangitis caused by obstruction or displacement of the stent.
Discussion
Acute cholangitis occurs in approximately one-third of patients with bile duct stones. 13 ACST is a severe form of acute cholangitis and results in high mortality, especially in elderly patients. Endoscopic decompression has been suggested to be the first choice in the urgent treatment of patients with ACST. 14 Both ENBD and ERBD using a plastic stent are effective in the management of biliary sepsis.6–8,15 Compared with plastic stent placement, ENBD is easier to irrigate when it is obstructed and does not block easily. In our study, ENBD was more effective in bile drainage and caused more rapid control of the disease. However, it was uncomfortable with long-term drainage and even led to unplanned extubation. Plastic stent placement was comfortable, but it had a high incidence of blockage and caused a slower decrease in liver enzyme levels. These findings were similar to those of some previous studies.7,8 Urgent biliary decompression and stone removal should be finished in two steps in ill, elderly patients. 16 Here, there might be a long waiting time before the second ERCP, or because someone could not undergo the second ERCP due to the poor physical condition and slow recovery of elderly patients. Therefore, both ENBD and single-stent placement have some shortcomings in the treatment of elderly patients with ACST.
Our study suggested dual-stent placement as a better choice for elderly patients with ACST, especially patients with difficult stones. Dual-stent placement had some advantages compared with ENBD and single-stent placement. (1) Placement of dual stents was more comfortable than ENBD. Previous studies have suggested that internal indwelling is a better choice for long-term biliary drainage, especially for confused or elderly patients who cannot tolerate ENBD.6,16,17 Therefore, dual-stent placement as an internal indwelling was suitable for long-term bile drainage. (2) The placement of dual stents was very effective for bile drainage and disease control. In this study, although no significant difference was found between the dual-stent group and the ENBD group, the placement of dual stents showed the fastest clearance of serum bilirubin and the fastest decrease in serum GGT among the three groups. The dual-stent group had a faster decrease in APACHE II scores at 1 day after the procedure and a shorter ICU stay than the other two groups. These effects might be the results of an enlarged drainage area and enlarged channel of dual-stent placement. (3) Compared with ENBD, plastic stent placement was much more helpful for stone removal at the second ERCP, which could contribute to an indwelling endoprosthesis reducing the volume and number of stones.18–20 (4) Dual-stent placement is generally operational and safe. Our study showed that the procedure time and the rates of pancreatic stenting and ERCP-related complications were similar in the three groups. One concern of our study was whether the placement of dual stents would increase the incidence of PEP. Although no significant differences in the rates of PEP were found among the three groups, the incidence of PEP in the patients with dual-stent placement without EST was as high as 14.29%, whereas that in the ENBD group was 7.41%, and that in the single-stent group was 6.67%. These outcomes might be the results of the limited number of patients in this study, and we should emphasize that dual-stent placement without the performance of EST in patients should be considered carefully. Regardless of this, the complications of dual-stent placement require further study.
The limitations of the present study were as follows: (1) It was only a retrospective study in a single center; (2) there were a limited number of patients in this study; and (3) the calibers of the plastic stent (8.5F) and the nasobiliary catheter (7.5F) were different.
In conclusion, our study suggested that the placement of dual stents had some advantages in the treatment of elderly patients with ACST compared with ENBD or the placement of a single stent. Dual plastic stent placement might be a better treatment for elderly patients with ACST due to choledocholithiasis. However, the incidence of PEP in patients with dual-stent placement deserves further study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for these works.