
Abstract
Objectives:
The purpose of this article was to systematically evaluate the clinical efficacy of laparoscopy-assisted distal gastrectomy (LDG) and open distal gastrectomy (ODG) in the treatment of gastric carcinoma (GC).
Methods:
PubMed, Web of Science, Embase, CNKI, and Wanfang databases were systematically searched for relevant articles on surgical treatment of GC published from 2010 to 2020. GC patients in the treatment group received LDG, whereas those in the control group received ODG. The evaluation criteria of these two surgical methods included operation time, intraoperative blood loss, postoperative first exhaust time, number of dissected lymph nodes, postoperative hospital stay, and incidence of complications.
Results:
A total of 18 studies, with 2102 patients, which met the criteria were included in this meta-analysis. The analysis results showed that in comparison with the control group, both the incidence rate of complications (odds ratio = 0.31, 95% confidence interval, CI [0.23 to 0.41]) and intraoperative blood loss (standardized mean difference, SMD = −2.72, 95% CI [−3.43 to −2.00]) were lower in the treatment group. In addition, in comparison with the control group, LDG led to an increase in the number of dissected lymph nodes (SMD = 0.08, 95% CI [−1.10 to 0.25], P = .403) and associated with shorter hospital stay (SMD = −1.42, 95% CI [−1.90 to −0.94]) and earlier postoperative first exhaust time (SMD = −2.12, 95% CI [−2.86 to −1.38]).
Conclusion:
LDG can significantly reduce the incidence of complications of GC, intraoperative blood loss, postoperative exhaust time, and hospital stay, whereas increase the number of lymph node dissection. Therefore, LDG is worthy of clinical application.
Introduction
Gastric carcinoma (GC) is one of the most common digestive system tumors, and also the third leading cause of cancer death worldwide. 1 Its incidence is the highest in China, and its number of cases is larger that of esophageal cancer and liver cancer, second only to lung cancer. 2 With the advancement of diagnosis and treatment techniques, the annual mortality rate of GC in China has decreased from 3.8% to 2.3%. 3 The etiology of GC is a complex and is a process in which multiple factors and mechanisms are involved. 4 So there are a variety of surgical strategies for GC in clinical practice, and the surgical practice may vary in different continents, countries, and surgeons. According to the different severity and prognosis of GC, radical or nonradical surgery has been proposed clinically, as well as symptom-relieving surgery (also known as palliative surgery) and cytoreductive surgery for cases without hope of radical cure. 5 Currently, the choice of surgical techniques, open or minimally invasive gastrectomy, has become a controversial topic in GC surgery. Kitano et al. 6 performed the first laparoscopy-assisted distal gastrectomy (LDG) in 1991. With the continuous development of laparoscopic techniques, related studies have reported that LDG has a better short-term efficacy compared with traditional open distal gastrectomy (ODG). 7 ODG is still the preferred surgical method (68%) in most clinical practice, and 65% of surgeons prefer minimally invasive distal gastrectomy for early GC. Minimally invasive total gastrectomy is performed in 49% of early GC while 6% of advanced GC, whereas, laparotomy was performed. 8 From the aforementioned studies, no consensus on the optimal surgical approach for GC has reached. Therefore, the aim of this study was to comprehensively and quantitatively compare the clinical efficacy of LDG and ODG in the treatment of GC to obtain the optimal one.
Materials and Methods
Literature search method
English databases such as PubMed, Web of Science, and Embase as well as Chinese databases such as CNKI and Wanfang were searched for relevant studies with the search terms: (“gastric carcinoma”), (“radical laparoscopic surgery” or “peritoneoscope operation”), and (“ open distal gastrectomy” or “traditional open surgery” or “conventional surgery”). Subsequently, other potential studies were selected through searching the references of relevant studies, as well as conference articles and abstract articles. The search time was from 2010 to 2020 with no language restrictions. IRB approval is not required for this study.
Inclusion and exclusion criteria of literatures
The inclusion criteria were based on participants, interventions, comparisons, outcomes protocol: (1) Population: GC patients who underwent surgery. (2) Intervention and control: LDG was provided in the treatment group, whereas ODG in the control group. Both groups required the surgeons to be proficient and standard in operation. (3) Outcome measures: At least one of the efficacy indicators such as operation time, intraoperative blood loss, postoperative first exhaust time, number of dissected lymph nodes, postoperative hospital stay, and incidence rate of complications of the two surgical methods. (4) Study design: randomized controlled trials. If multiple studies were from the same research institution, the one with the best quality or the recently published one would be included.
Exclusion criteria were as follows: (1) not GC patients; (2) patients who received neoadjuvant chemotherapy and/or radiotherapy before operation; (3) studies without data required by this meta-analysis, and studies available for the original text; (4) literature with poor quality, missing data, and duplicate literature; (5) case reports, systematic reviews, and animal trials.
Literature quality evaluation and data extraction
Quality assessment and data extraction were independently performed by 2 investigators. According to the inclusion and exclusion criteria, the titles and abstracts and full text were carefully read to screen appropriate articles. The following data were extracted: basic characteristics of the literature, type of study method, sample size, and outcome measures. Disagreements in data extraction were resolved by discussion with a third researcher.
Statistical analysis
Heterogeneity in the study was assessed using the Q test (P < .10 indicating heterogeneity) and the I2 statistic. In case of heterogeneity (P < .10 and I2 > 50%), random-effects model (REM) was adopted; otherwise, fixed-effects model (FEM) was employed. Results of categorical variables were reported as odds ratio (OR) and 95% confidence interval (CI), whereas numerical variable results as standardized mean difference (SMD) and 95% CI. P < .05 suggested statistically significant differences. Sensitivity analysis was utilized in assessing whether the meta-analysis results were robust and credible while funnel plot (with a test of α = 0.10) in observing whether there was publication bias. All statistical analysis processes were performed using Sata16.0.
Results
Literature search results
The literature screening process is presented in Figure 1. Initially, 193 relevant articles were included, and then 148 of them were excluded by titles and abstracts. Finally, after the full text was read and quality evaluation, 18 articles were included in this meta-analysis.,9–26 with a total of 2102 patients (1006 in the treatment group and 1096 in the control group). Basic characteristics of included studies are shown in Table 1. The included studies were all retrospective observational studies with observation time ranging from 10 months to 10 years, and the age and gender of the both groups were comparable in these studies.
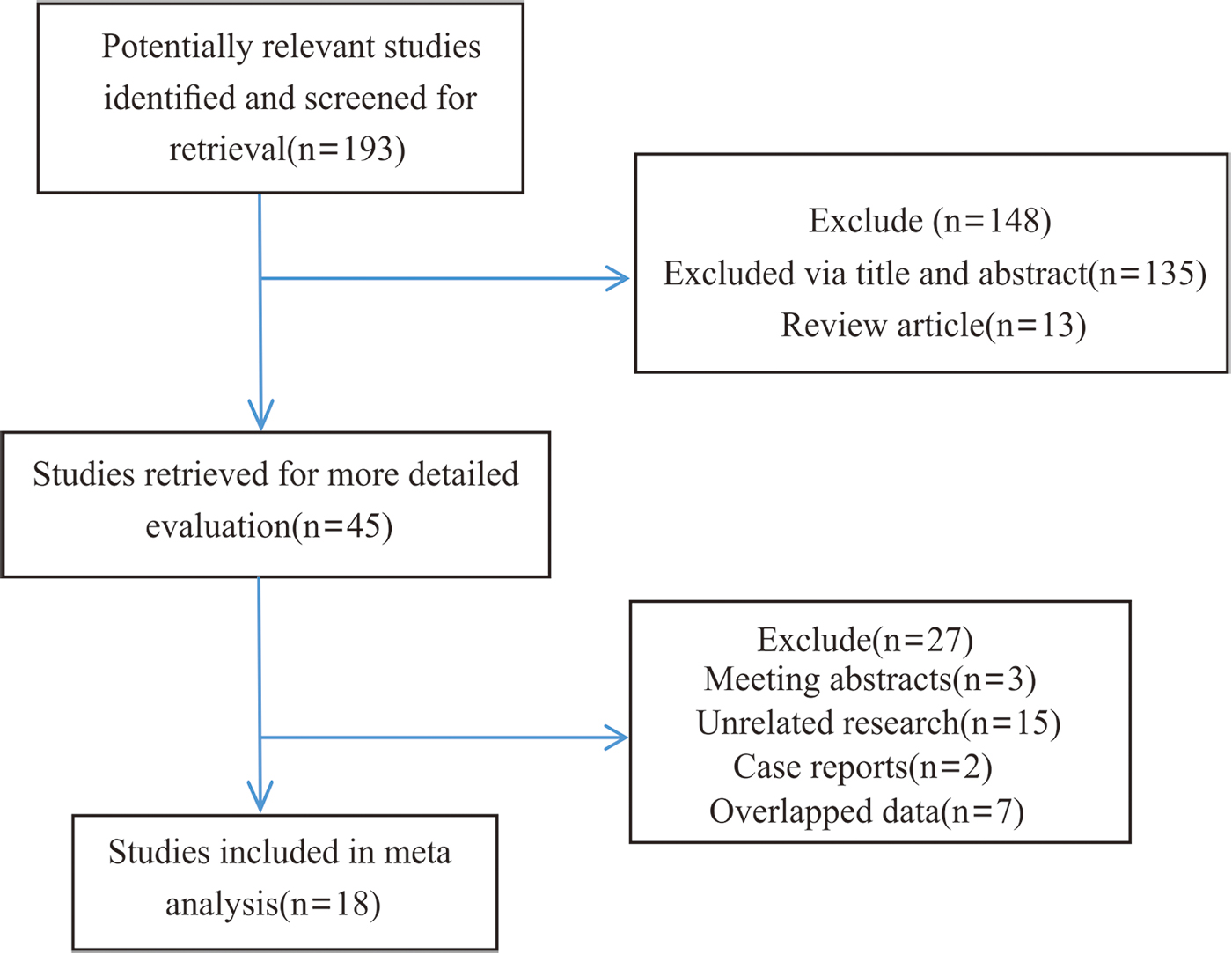
Literature screening flowchart. Color images are available online.
The Basic Characteristics of Inclusion in the Literature
①: Estimated blood loss; ②: operating time; ③: hospital stay; ④: time to first flatus; ⑤: complications; ⑥: number of retrieved lymph nodes.
NR, not reported.
Meta-analysis results
Incidence of complications
A total of 14 studies reported incidence of complications in both groups. No marked heterogeneity existed (I 2 = 6.10%, P = .385), so the FEM was employed for analysis. The results showed that the incidence rate of complications in the treatment group was significantly lower than that in the control group, which was 0.31 times that in the control group (OR = 0.31, 95% CI [0.23 to 0.41], P < .001) (Fig. 2).
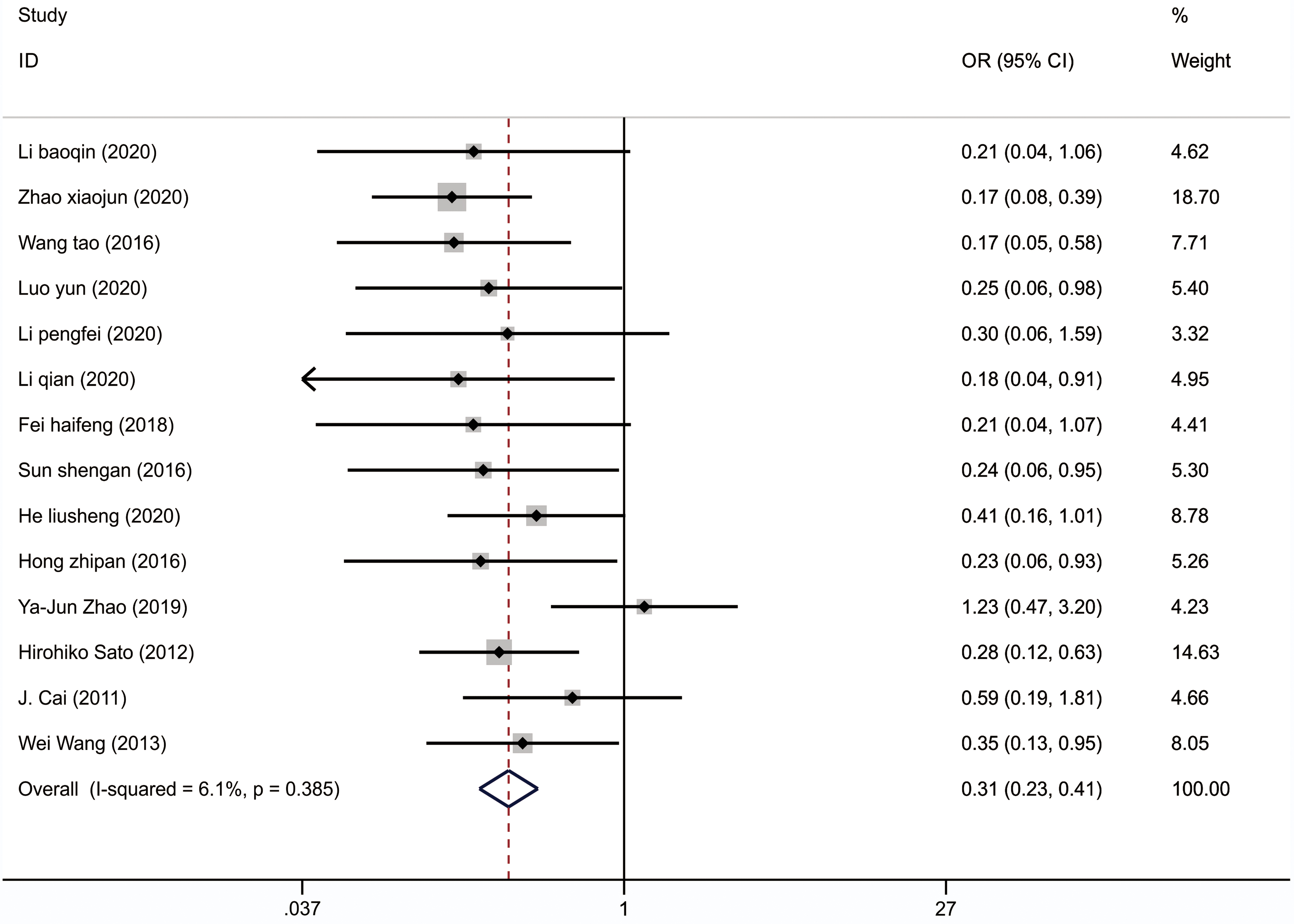
Forest map of the incidence rate of gastric cancer complications in the two groups. Color images are available online.
Number of dissected lymph nodes
A total of 11 studies provided the number of dissected lymph nodes in the two groups. Marked heterogeneity existed (I 2 = 63.50%, P = .002), so the REM was utilized. The results showed that the number of dissected lymph nodes in the treatment was significantly larger than that in the control group (SMD = 0.08, 95% CI [−1.10 to −0.25], P = .002) (Fig. 3).

Forest plot of number of dissected lymph nodes between the two groups. Color images are available online.
Other efficacy indicators
A total of 18 studies compared intraoperative blood loss between the two groups (Fig. 4A). The REM was used due to the significant heterogeneity (I 2 = 97.60%, P < .001). And the results showed that the intraoperative blood loss in treatment group was significantly lower than that in control group (SMD = −2.72, 95% CI [−3.43 to −2.00], P < .001).

Forest map of secondary efficacy indicators in the two groups.
A total of 17 articles compared the operation time (Fig. 4B). The REM was adopted due to the marked heterogeneity (I 2 = 97.20%, P < .001). The result showed no significant difference in operation time between the two groups (SMD = 0.468, 95% CI [−0.13 to 1.07], P = .127).
A total of 14 studies compared the hospital stay (Fig. 4C). The REM was utilized for analysis due to the marked heterogeneity (I 2 = 93.40%, P < .001). The results showed that the length of hospital stay in the treatment group was significantly shorter than that in the control group (SMD = −1.42, 95% CI [−1.90 to −0.94], P < .001).
A total of 14 studies compared the postoperative first exhaust time (Fig. 4D). The REM was employed for analysis due to the marked heterogeneity (I 2 = 93.40%, P < .001). The results showed that the postoperative, first exhaust time in the treatment group was earlier than that in the control group (SMD = −2.12, 95% CI [−2.86 to −1.38], P < .001).
Sensitivity analysis
From the results of sensitivity analysis of the incidence rate of complications (Fig. 5), the number of dissected lymph nodes (Fig. 6), as well as intraoperative blood loss (Fig. 7A), operation time (Fig. 7B), hospital stay (Fig. 7C), and postoperative first exhaust time (Fig. 7D), the aforementioned indicators did not change after being pooled. This indicated that the sensitivity of these indicators was low, and the results of this meta-analysis were robust and credible.

Sensitivity analysis chart of complication rate in two groups.

Sensitivity analysis plot for the number of dissected lymph nodes in the two groups.
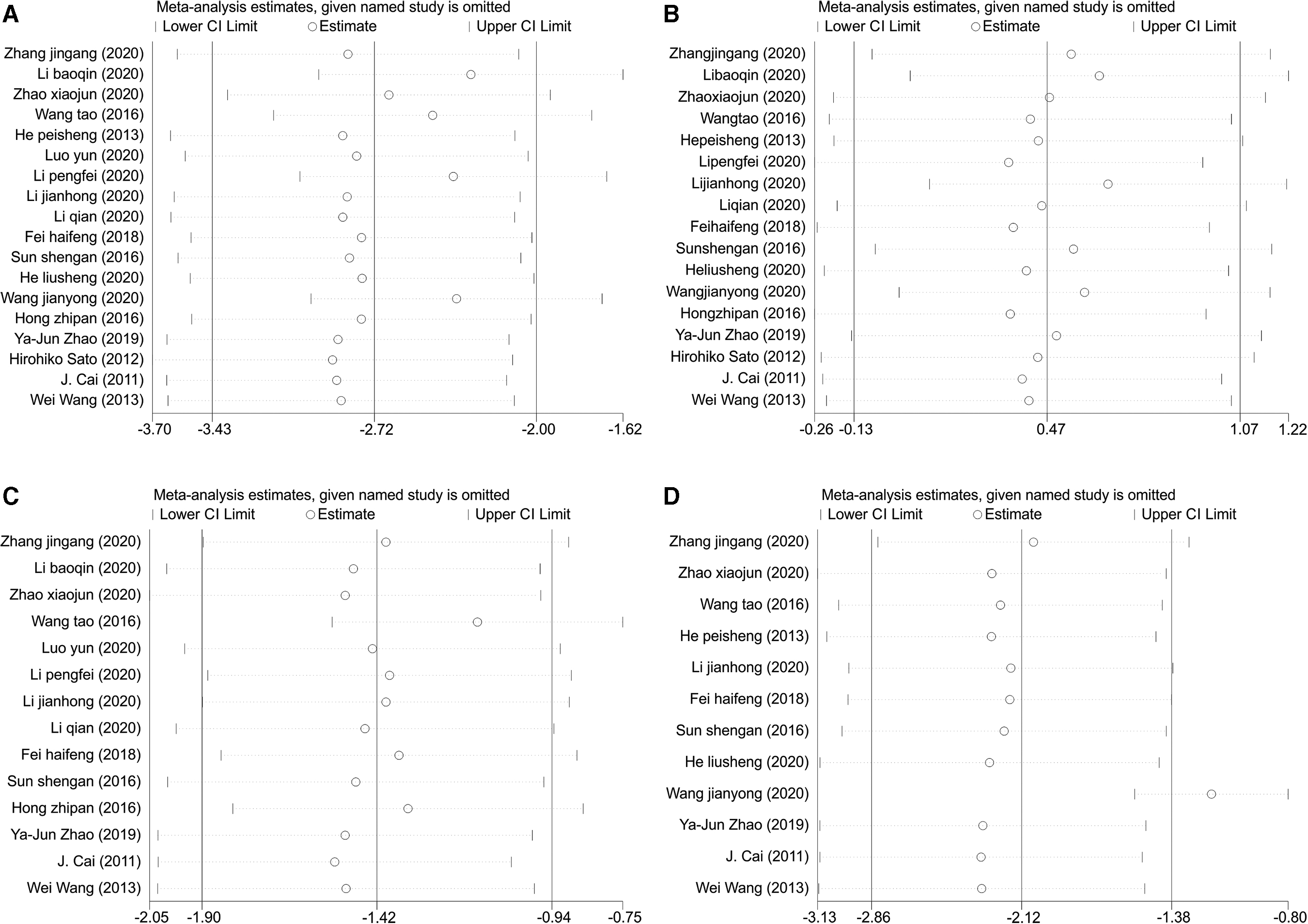
Sensitivity analysis of secondary efficacy indicators in the two groups.
Publication bias
Funnel plots were further used to detect publication bias in the included studies. As shown in Figures 8 and 9, the included studies scattered either side in symmetrical manner, confirming no significant publication bias in the incidence of complications and the number of dissected lymph nodes. In addition, the scatter distribution of the intraoperative blood loss (Fig. 10A), operation time (Fig. 10B), hospital stay (Fig. 10C), and postoperative scheduling time (Fig. 10D) was also basically symmetrical, indicating the possibility of low publication bias and robust meta-analysis result.

Funnel plot of complication rate in two groups. Color images are available online.

Funnel plot of number of dissected lymph nodes in two groups. Color images are available online.

Funnel plot of secondary efficacy indicators in the two groups.
Discussion
GC has a high incidence in clinical practice. Japanese gastric cancer treatment guidelines (5th edition) by Japanese Gastric Cancer Association (JGCA) has clarified LDG as a routine surgery for stage I GC, 5 whereas laparotomy as a potential choice for progressive GC patients. The rapid development of minimally invasive techniques has changed the traditional view of surgical treatment of advanced cancer, but some surgeons are reluctant to perform laparoscopic surgery for progressive GC due to its uncertainty of safety and oncological results. 27 In recent years, D2 LDG for progressive GC by an experienced team is safe and feasible, and there is no significant difference in 3-year disease-free survival rate and overall survival rate between laparotomy group and laparoscopy group. 28 In 2016, relevant medical institutions issued the recommended indications for laparoscopic surgery: GC exploration and staging; D2 radical resection for GC < T4a stage; GC at stage I, II, and IIIA before surgery; short-circuit surgery for advanced GC. 29 In view of the fact that the surgical treatment of GC is not uniform, this meta-analysis compared the clinical efficacy of LDG and ODG in the treatment of GC, thus providing a basis for selecting the optimal one.
A total of 14 studies reported the incidence rate of complications in the two groups, and the results of meta-analysis revealed lower incidence of complications in the treatment group compared with the control group. The possible reason is that open surgery reduces the patient's tolerance to prolonged surgery; in contrast, LDG for tumor resection and lymph node dissection has the advantages of clear surgical field, small wound, mild trauma, rapid postoperative recovery, and lower incidence of complications, reducing immune damage. 30
A total of 11 studies provided the number of dissected lymph nodes in the two groups, and the results showed that this number was larger in treatment group. At present, lymph node metastasis is considered to be an important factor affecting the long-term survival rate of GC patients. 31 The follow-up data obtained by Kim et al. 31 revealed that in 10,873 GC patients, the corresponding regional lymph node dissection can improve the survival rate, especially in advanced GC patients. Siewert et al. 32 found that lymph node metastasis is a critical prognostic factor, and extended lymph node dissection can prolong the survival time of GC patients after surgery. Laparotomy has limitations and some difficulty for lymph node dissection. In contrast, laparoscopic surgery with the aid of instruments can magnify the visual field, and surgeons can clearly observe the lesion and various anatomical sites and vascular directions, and subsequently remove and dissect the lymph nodes completely.33,34 Collectively, lymph node dissection can completely improve the long-term survival rate of patients, and laparoscopic surgery is superior to laparotomy in the effect of lymph node dissection.
A total of 18 studies compared the intraoperative blood loss between the groups, and the comprehensive result revealed lower intraoperative blood loss in the treatment group. In 17 studies, the operation time was compared and found no significant difference between the groups. Compared with ODG, LDG for GC reduce the blood loss during surgery. This may be due to the small wound of laparoscopic surgery and the magnified field by electron microscope, thus avoiding the damage to the surrounding vessels. 35 With the promotion of laparoscopic surgery and the continuous maturity of surgeons' techniques, LDG for GC gradually has no significant difference in operation time compared with laparotomy, 36 which is consistent with the conclusion of this article.
Fourteen studies compared the length of hospital stay, and found shorter hospital stay in the treatment group. Fourteen studies compared postoperative first exhaust time, and the result showed earlier exhaust time in the treatment group. Laparoscopic surgery reduces surgical trauma, promotes recovery of body function, and accelerates recovery time, leading to shorter hospital stay and earlier postoperative first exhaust time. 37 Collectively, compared with ODG, LDG for GC had the advantages in reducing intraoperative blood loss, shortening hospital stay, and making postoperative first exhaust time earlier.
This study also has some limitations. First, the sample size is small, and all included articles are retrospective observational studies without randomization. The aforementioned factors may lead to some selection bias and information bias. Second, due to the limited information provided in the literature, the effects of various confounding factors such as age, gender, and GC grade cannot be analyzed. Finally, laparoscopic surgery is closely related to the operating ability, but the technical difficulty is not discussed in the text, and it is not mentioned whether the surgeon is proficient and the number of surgeons who can perform laparoscopic surgery.
In summary, based on a comprehensive analysis of relevant clinical studies, we believe that LDG has significant overall advantages in improving overall therapeutic effect. Specifically, LDG can reduce the incidence of postoperative complications, intraoperative blood loss, and hospital stay and postoperative first exhaust time, whereas can increase the number of dissected lymph nodes. This method provides a crucial important reference for the treatment of GC patients, and is worth promoting and applying in clinical practice.
Footnotes
Disclosure Statement
No competing financial interests exit.
Funding Information
No funding was received.