
Abstract
Objectives:
To prove the hypothesis that modifying the endoscopic correction of vesicoureteral reflux (VUR) technique (STING procedure) and sharpening its contraindications, lead to increased success rate and decline in the complication rate.
Materials and Methods:
All patients that underwent endoscopic correction of VUR utilizing Vantris were divided into two groups according to procedure date; before 2015 and 2015–2019. Indication for treatment included persistent high-grade VUR or breakthrough infections. Contraindications included voiding dysfunction, active infection and since 2015 suspicion for obstructive/refluxing ureterovesical junction (UVJ) presented by “beak” sign on voiding cystourethrography (VCUG). Follow-up regiment included ultrasound and VCUG at predetermined intervals.
Results:
The first group included 215 (158 girls and 57 boys) children with mean age of 4.8 ± 2.8 years who underwent endoscopic correction between 2009 and 2015 and the second group included 42 children (28 girls and 14 boys) with mean age of 3.9 ± 2.1 years who underwent surgery between 2015 and 2019. In the first group, VUR was unilateral in 74 patients and bilateral in 132 comprising 338 renal refluxing units. In the second group, VUR was unilateral in 14 patients and bilateral in 30 comprising 74 RRUs. In the first group reflux was corrected in 317 (94.9%) RRUs after a single injection, after the second in 7 (2.1%) RRUs. In seven (2.1%) RRUs, reflux downgraded to Grade I–II. Three RRUs (0.9%) failed endoscopic correction and required ureteral reimplantation. Nine (2.7%) RRUs developed UVJ obstruction. In the second group reflux was corrected in 61 (82.4%) RRUs after a single injection, after the second in 12 (16.2%) RRUs. In one (1.4%) RRU, endoscopic correction failed and required ureteral reimplantation. None of the patients developed UVJ obstruction. Reflux correction has led to the significant decrease of febrile urinary tract infection (UTI) in both groups.
Conclusions:
Our data indicate that endoscopic injection utilizing Vantris is safe and long durable procedure. Although utilizing the proper technique and contraindication criteria, the rates of post procedural VUJ obstruction is null.
Introduction
Since the introduction of STING (“Subureteral Transurethral Injection”-correction of vesicoureteral reflux [VUR] by injecting bulking agent to the ureteral orifice) 30 years ago, and since the approval of “Dextranomer/Hyaluronic-Acid copolymer” (Deflux; Q-Med Scandinavia, Uppsala, Sweden) by the FDA (Food and Drug Administration) for the treatment of VUR, the endoscopic approach for the correction of VUR became a first-line treatment for all grades of reflux in some pediatric urology centers.1–6 The overall success rates were published by several groups and range between 68% and 92%, affected mainly by the VUR grade.1–5 The complication rates after this procedure relates mainly to the obstruction of ureterovesical junction (UVJ) and the development of a new contralateral vesicoureteral reflux after treatment of unilateral VUR. 6
Since the endoscopic treatment for the correction of VUR had remarkable success in decreasing the rates of urinary tract infection (UTI) in the short-term follow-up, it is eminent to examine the long-term efficacy by observing the incidence of UTI after endoscopic correction of VUR over the long run. Decade ago concerning data regarding the recurrence rate after successful treatment of VUR utilizing Deflux was presented. 7 Some pediatric urologists speculated that the biodegradable nature of Deflux is responsible for its elimination and subsequent VUR recurrence.6,7 These results, and the published overall recurrence rate of up to 21%, are remarkably sobering and implies that another bulking agent is needed to reach long-term efficacy by the endoscopic correction of VUR. Polyacrylate-polyalcohol-copolymer (Vantris, Promedon, Cordoba, Argentina) is a nonbiodegradable substance that can be used as a bulking agent, and shown to present short-term efficacy, but also potentially avoid reflux recurrence due to nonbiodegradable nature. 8
Over the past 10 years, we have conducted a prospective evaluation of Vantris in our practice. Over this period we have published our short- and long-term results.9–11
During those years we witnessed an evolution of our technique and gained better understanding of when the endoscopic correction of VUR should be avoided and open/robotic ureteral reimplantation surgery should be performed instead.
Since the majority of changes occurred in 2015 we have hypothesized that by comparing two groups of patients, the first includes all patients who underwent endoscopic correction of VUR with Vantris before 2015 and the second includes the cases between 2015 and 2019, we would be able to show the better results with less complications in the second group.
Moreover, the number of patients in the study who underwent endoscopic correction of VUR with the bulking agent Vantris is the largest to be reported so far; therefore, we would like to share the experience we have gained with special emphasis on the lessons and recommendations that we have learned and developed over this period.
Materials and Methods
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study. After permission from the Institutional Review Board, we have retrospectively evaluated our prospectively collected clinical database.
Owing to the evolution of our surgical technique and changing of the indications for surgery during the study period, all patients were divided into two groups. The first group included all the children who underwent endoscopic treatment for the correction of VUR using Vantris between 2009 and 2015, and the second group included the children from 2015 to 2019.
We published before our indications for the endoscopic correction of VUR and our follow-up schedule. In brief, the VUR grade is estimated by voiding cystourethrography (VCUG) preceding and after surgery or during conservative treatment, in accordance to the International Classification System (International Reflux Study Committee). 12 The indications for endoscopic correction of VUR in most of the cases were persistent high-grade VUR or breakthrough infections while on antibiotic prophylaxis. However, in some patients, VUR correction was performed according to guardian request. Children who suffered from symptoms of dysfunctional voiding or constipation were allocated to conservative treatment before endoscopic treatment until full resolution of the voiding symptoms was achieved and preoperative reassessment, including repeated VCUG, was performed. As we have already mentioned, we have adopted in our practice a dysfunctional voiding symptoms survey for the evaluation of dysfunctional voiding.9–11 None of the children in this series had voiding dysfunction at the time of endoscopic treatment.
Since 2015 following increased number of UVJ obstructions in our studied population we have started to perform routinely postvoiding images in all patients undergoing VCUG seeking for the presence of “beak” sign in the refluxing ureter. 13 The beak sign suggests the presence of obstructive/refluxing UVJ. All patients with the presence of “beak” sign were denied endoscopic correction and underwent open (Cohen or Politano-Leadbetter) or recently robotic-assisted laparoscopic reimplantation. 14
99mTc dimercaptosuccinic acid scan (DMSA) renal scans were taken to assess relative renal function (RRF) using background corrected regions of interest of each kidney in the posterior view and calculating the resultant percentage uptake. The scan was performed at least 6 months after the last febrile UTI. Renal scintigraphy was taken 2 hours after injection of DMSA. The fractional left and right renal activity was calculated for each kidney. RRF of 40%–50% of total renal activity was considered as normal, 30%–40% was considered as moderate, and renal function <30% was considered as poor.
All injections were performed by a single surgeon (B.C.) as part of the study protocol. The technique of endoscopic correction has undergone an evolution during the study period. In the beginning, in patients with grade I–III VUR, we utilized the usual technique of STING, with the needle introduced submucosally under the ureteral orifice at the 6 o'clock position. In patients with grade IV and V VUR or in those with a widely open orifice, the injection was performed inside the orifice. Since November 2015 we have adopted previously published technique of ureteral lifting and implant reposition. 15 The needle is introduced submucosally under the ureteral orifice at the 6 o'clock position while only needle tip is positioning under mucosa during the commencement of the injection the surgeon lifts a needle with the mucosa allowing a proper placement of the implant under the mucosa (Supplementary Video S1) (Figs. 1 and 2).
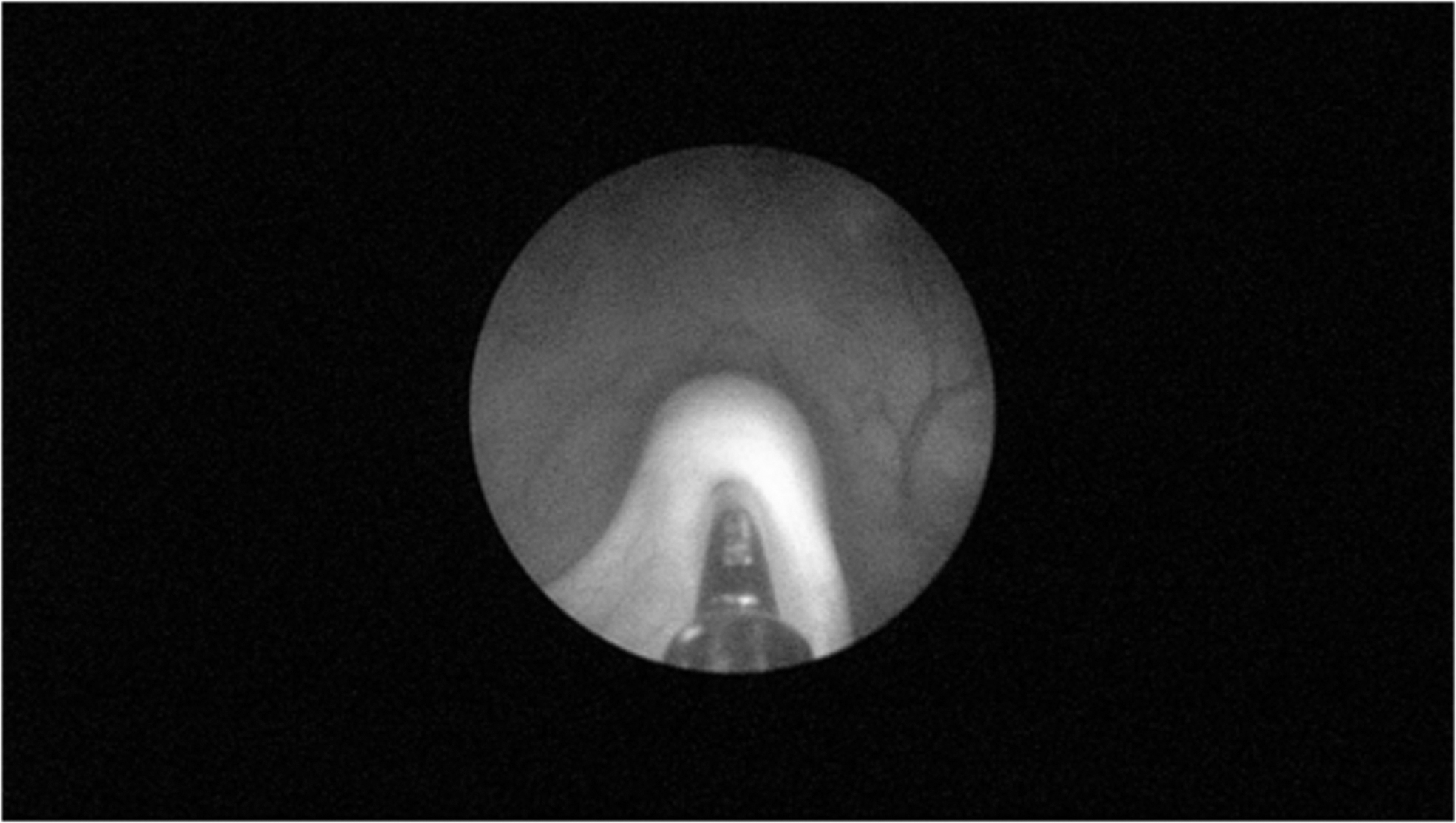
Ureteral orifice during the ureteral lifting technique.

Ureteral orifice after Vantris injection.
We have also started to utilize about the same time metallic needle in our practice supplies by Promedon (Cordoba, Argentina) along the injectable material. Having more than two decades of experience with flexible needles we feel that the use of metallic needle is easier to manipulate during injection, independence from the assistant, possibility to lift and rotate a needle during injection, and finally allowing to put an implant at the proper place.
Grade I reflux was treated only in children with contralateral high-grade VUR. Overall, 97 (24%) of ureters have had Grade I–II upon correction. Bladder mucosa considered to be inflamed if on cystoscopy examination upon injection mucosal erythematous swelling with or without ulceration was seen. In those cases, the surgery was postponed.
The follow-up protocol included ultrasound scan performed 1 month after endoscopic correction of VUR to evaluate for the presence of hydronephrosis, obligatory VCUG was performed 3 months after the endoscopic treatment, and if VCUG demonstrated no reflux prophylactic antibiotic treatment was stopped (all patients received prophylactic antibiotic treatment until VCUG showed resolution of VUR). Reflux was determined to be cured if VCUG did not show any grade of VUR. Our ultrasound follow-up schedule was 1, 3, 5, and 10 years after treatment. Following the same prospective schedule we suggested to perform VCUG 1, 3, and 10 years after endoscopic treatment.
If follow-up ultrasound (US) demonstrated an appearance of new hydronephrosis or deterioration of previously existed hydronephrosis, repeat US or dynamic renal scan or magnetic resonance urography study were performed to rule out UVJ obstruction. After diagnosis of UVJ obstruction the patient underwent ureteral reimplantation utilizing one of the existing technique (Cohen or Politano-Leadbetter) or robotic-assisted laparoscopic reimplantation according to the surgeon preferences.
Median follow-up was 7 years (range 4–11 years) in the first and 3 years (range 8 months to 5 years) in the second group.
Commercially available software GraphPad Prism version 6.02 for Windows, (GraphPad Software, San Diego, CA, USA) was used. Mann–Whitney U test and Fisher's exact test were utilized for statistical evaluation, of the factors, considering P value of <.05 as significant.
Results
The demographic and clinical data presented in Table 1. The first group included 215 (158 girls and 57 boys) children with mean age of 4.8 ± 2.8 years (mean ± standard deviation) who underwent surgery between 2009 and 2015 and the second group included 42 children (28 girls and 14 boys) with mean age of 3.9 ± 2.1 years who underwent endoscopic correction between 2015 and 2019. In the first group, VUR was unilateral in 74 patients and bilateral in 132 comprising 338 renal reflux units (RRUs) Grade I was in 19 (5.7%) RRUs, Grade II in 48 (14.4%), Grade III in 168 (50.3%), Grade IV in 71 (21.3%), and Grade V in 28 (8.3%) RRUs consequently. Initial RRF revealed 160 (48%) children with RRF >40%, 80 (24%) with RRF between 30% and 40%, and 94 (28%) patients with RRF <30%. The mean RRF was 32.9 ± 6.9 (mean ± standard error of the mean [SEM]) in all reviewed children before the surgery.
Demographic Characteristics of Studied Patients
RRU, renal refluxing units; SD, standard deviation.
In the second group, VUR was unilateral in 14 patients and bilateral in 30 comprising 74 RRUs. Grade I was in 9 (12.2%), Grade II in 19 (25.6%), Grade III in 35 (47.3%), Grade IV in 9 (12.2%), and Grade V in 2 (2.7%) RRUs consequently.
Initial RRF revealed 50 (68%) children with RRF >40%, 16 (21%) with RRF between 30% and 40%, and 8 (11%) patients with RRF <30%. The mean RRF was 38.9 ± 6.5 (mean ± SEM) in all reviewed children before the surgery.
In the first group reflux was corrected in 317 (94.9%) RRUs after a single injection, after the second injection in 7 (2.1%) RRUs. In seven (2.1%) RRUs, reflux downgraded to Grade I and II, and they were taken off antibiotic prophylaxis. Three RRUs (0.9%) failed endoscopic correction and required ureteral reimplantation. Nine (2.7%) RRUs developed UVJ obstruction and required ureteral reimplantation. In these patients, reflux was Grade III in one RRU, Grade IV in three and V in five RRUs, respectively. All patients developed obstruction between 1 and 2 years after injection.
Whereas in the second group reflux was corrected in 61 (82.4%) RRUs after a single injection, after the second injection in 12 (16.2%) RRUs. In one (1.4%) RRU, endoscopic correction failed and required UR. None of the patients developed UVJ obstruction. The patients from the second group have had significantly lower numbers of GR V VUR (P < .0001) and required significantly less volume of Vantris to cure the reflux 1.1 ± 0.4 versus 0.4 ± 0.1 (P = .012). However, there were no difference in the overall success rate between two groups (Fig. 3) Moreover, we also did not find a difference in the success rate after single injection in both groups (P = .058). Reflux correction has led to the significant decrease of febrile UTI in both groups (Fig. 4).
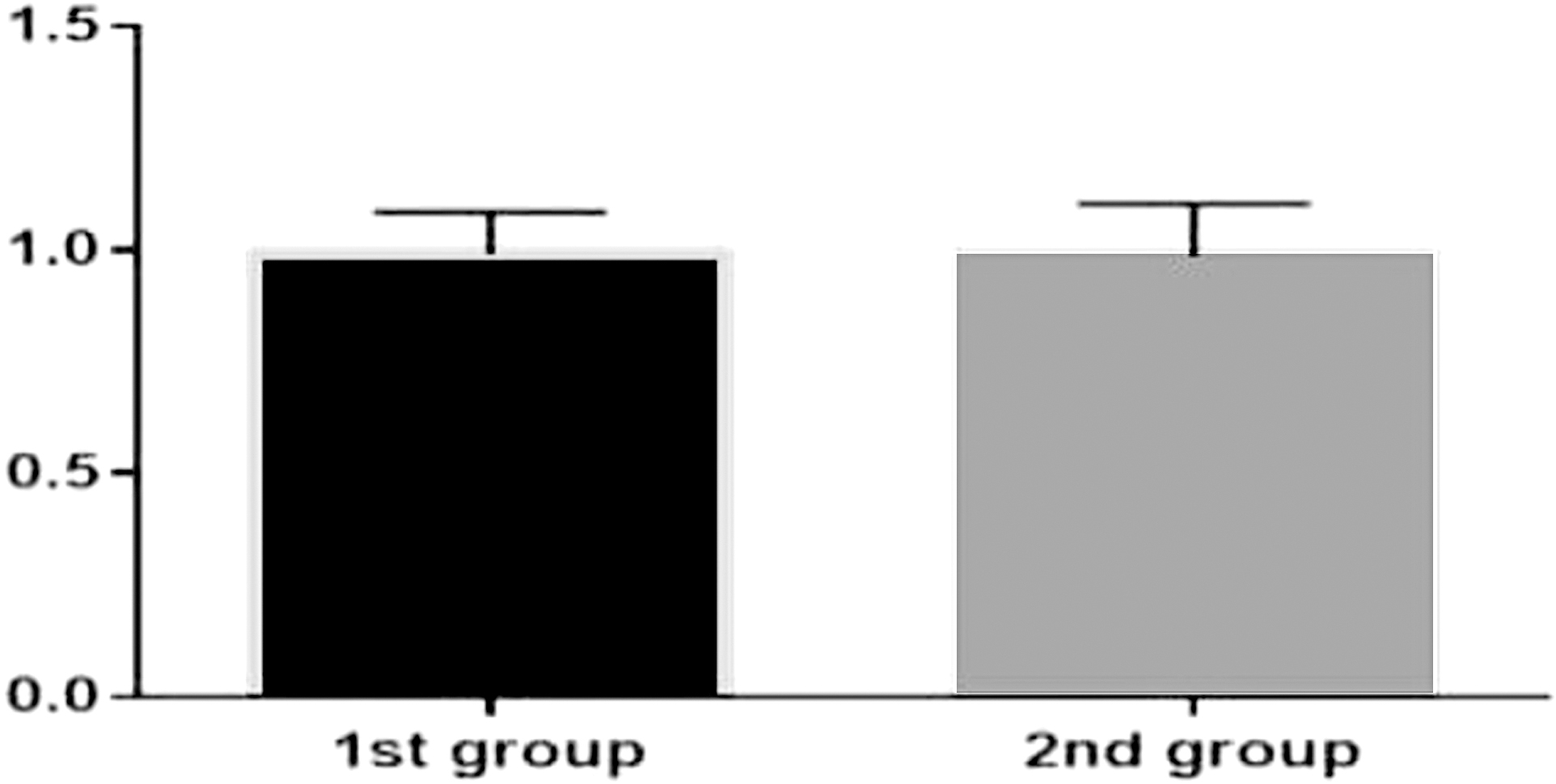
Outcome of treatment in both groups.
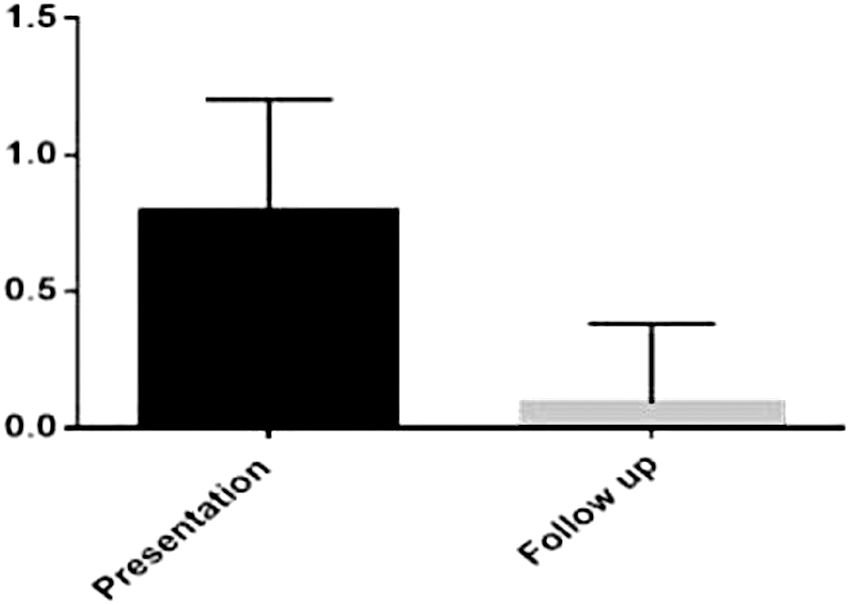
Incidence of UTI over the study period. UTI, urinary tract infection.
Thirty-eight percent of our patients have had VCUG 1 year and 40% 3 years after surgery as a part of our protocol. None demonstrated reflux recurrence. Moreover, all patients who have had developed febrile and afebrile UTI underwent obligatory VCUG as a part of our protocol, none of these patients showed reflux recurrence. Furthermore, 11 patients who developed reflux recurrence after Deflux injection and underwent successful endoscopic correction with Vantris have had VCUG as a part of prospective Vantris evaluation, also did not demonstrate reflux recurrence.
Nine children from the first and two from the second group underwent follow-up DMSA due to suspected renal development arrest on the postoperative US. None demonstrated significant deterioration of the renal function.
Discussion
The high reflux recurrence after reflux correction using Deflux has led us to look for an alternative bulking agent without biodegradable features.6,7 Although our own data on the reflux recurrence demonstrated only 9% recurrence rate after Deflux injection (unpublished data) we have thought that we have to find a better alternative. Vantris is a nonbiodegradable substance of synthetic origin belongs to the acryl family.6,8–11 The particles of Vantris have an average diameter of 300 μm, compared with Deflux with average diameter of 130 μm, therefore reducing the risk of local and distant migration. Once injected the implant is also stable through time.
In this study in accordance to the previous studies we have not observed reflux recurrence after successful correction utilizing Vantris as bulking agent.10,11 Although not all of our patients in this group underwent obligatory VCUG in the long term, however those who have had repeated VCUG after 1 and 3 years demonstrated no reflux recurrence. Furthermore, we have also repeated VCUG in the patients after febrile and afebrile UTIs as a part of the protocol in this specific group of patients and none of these patients demonstrated reflux recurrence. Of course, it could be that some of our patients have had “silent” reflux recurrence; however, since they all have been under strict follow-up and did not develop febrile UTI, we assume that they are not at risk of renal damage development. Moreover, the incidence of febrile UTI decreased significantly after successful endoscopic correction in all patients further proving a durability of Vantris as a bulking agent.
We have not performed routine DMSA scan in the postoperative period. However, these patients who have risen suspicion on the arrest of the renal development and have had a new DMSA scan did not show new renal scarring or further renal deterioration.
We could not brush aside the higher incidence of UVJ obstruction in the beginning of our learning curve. The 2.7% of patients in the first group who reflect our initial experience went on and developed UVJ obstruction required ureteral reimplantation. Others also raised concern regarding UVJ obstruction related to Vantris injection.16–19 This incidence led us to reconsider our contraindications for surgery and to re-evaluate our experience to define which patients are more prone to develop obstruction and must be excluded from endoscopic correction.
We have published our data concerning indications/contraindications for endoscopic correction and right patient selection. 13 Our long-term data further prove our previously published conclusions. For all patients from the second group new contraindications for endoscopic reflux correction were applied. All postvoiding images on VCUG were meticulously evaluated and all patients with even mild suspicion on the presence of “beak” sign of ureter were referred for ureteral reimplantation. Furthermore, all patients with high-grade ureteral reflux who could develop UVJ obstruction due to possible dysfunctional features of the intramural part of the ureters were closely followed after the procedure and their parents informed.20–23 It should be ironed out that even if the patient developed UVJ obstruction after Vantris injection it usually occurs during the first 2 years after correction, as Kocherov et al. just polished out his expertise in multicenter study proving overall safety of Vantris and further shedding out the fear of silent obstruction and loss of renal function in the long-term period. 24
Another important observation that we have learned over the period is the technique of injection. All patients from the second study period underwent so-called ureteral lifting technique. 15 We do believe that utilization of this technique allows proper implant placement with minimal amount of Vantris required to correct reflux and avoid complications, while maintaining high rate of overall success (Fig. 5). Of course, one could speculate that our overall success with new technique is due to increased experience with endoscopic correction rather than a new technique. However, the senior author has had sufficient level of expertise with endoscopic correction upon study commencement and just polished out his expertise during this evaluation.
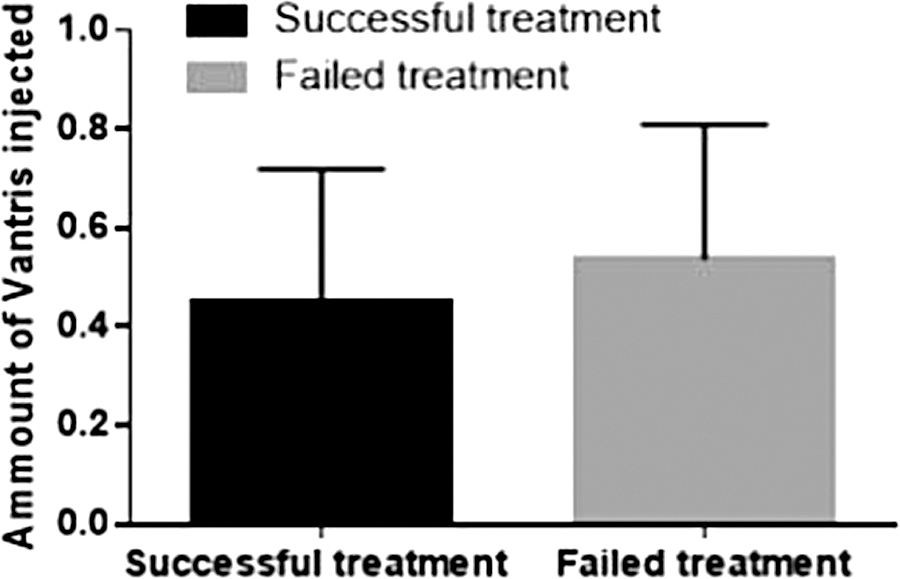
Outcome of endoscopic correction regarding the amount of Vantris.
Finally, we have developed recommendations regarding ureteral reimplantation after UVJ obstruction in patients after endoscopic correction with Vantris. We have encountered technical problems in some patients concerning the transvesical dissection of the intramural part of the obstructive ureter that could be technically demanding due to fibrotic reaction around obstructive orifice. However, not all 9 obstructed patients in this study demonstrated such reaction; furthermore, we have encountered similar issues in our practice with other patients who were injected different tissue augmenting substance and further required ureteral reimplantation. Therefore, we do recommend performing extravesical reimplantation or approaching ureter extravesically to avoid transvesical dissection and to perform reimplantation with extravesical or extra-/intravesival manner according the surgeon preference. Recently, we have utilized robotic approach for reimplantation with good functional results and today it is our preference to deal with obstructive ureter after endoscopic correction. 14
Some study limitations should be mentioned. The group's population is different as well as the numbers of the patients in the studied groups. The overall drop in the number of children who underwent endoscopic correction might be explained by different reasons. Length of the study period was different in two groups. Our indications for reflux treatment and particularly patient selection for endoscopic correction has evolved over the past 10 years and led us to refer some candidates for open surgery from the beginning. Correct patient selection from our point of view has resulted in the negligible complications rate in the patients from the second group as aforementioned and, therefore, proving our hypothesis to be correct.
We did not obtain VCUG in all patients who completed 10 years of the follow-up. However, we have pointed out that we have maintained prospectively our clinical database and were able to register all incidences of UTIs or other adverse reactions. We do not have data on the characteristic appearance of Vantris on computed tomography (CT), but we do know that it is barely seen on US examination and do hope that in the future we will gather enough experience to describe the visibility of Vantris on CT. In this specific group of patients all injections were performed by a single surgeon with previous experience in endoscopic correction of VUR. That could explain our high overall success rate in this series and might not reflect the general practice. However, in our department we have several pediatric Urologists who utilize Vantris. And we will continue to prospectively evaluate its efficacy and safety, And report more recommendations in the future.
Conclusions
Our data indicate that endoscopic injection utilizing Vantris is safe and durable procedure that significantly reduces the risk of acute pyelonephritis after successful repair. Right patient selection and use of the ureteral lifting technique allow to achieve a high success rate of reflux correction with negligible complications rate. In case of UVJ obstruction, we do recommend avoiding transvesical approach, while performing ureteral reimplantation and deal with the ureter extravesically leaving behind the obstructive intramural part. Robotic assisted surgery, when available, appears to be the method of choice in these patients.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.