
Abstract
Background:
Qualitative fluorescence angiography (FA) provides insights into intestinal tissue perfusion, but today it is not yet accurate in predicting anastomotic leakage. To improve peroperative detection of impaired perfusion, quantified parameters should be investigated using a standardized method. The aim of this study was to develop a (semi)automated algorithm for comprehensive and convenient analysis of FA parameters.
Materials and Methods:
An analysis tool was developed for the extraction of quantified FA parameters. The start- and endpoint of intensity increase (T0 and
Results:
Automated detection of T0 and
Conclusions:
The presented method provided convenient data analysis in the search for effective FA quantification. Future research should expand the data to find adequate threshold values for peroperatively identifying insufficient perfusion and investigate the influence of physiological conditions.
Introduction
Inadequate local or systemic perfusion is regarded as a substantial factor in complications after gastrointestinal surgery. The most feared and frequent example is anastomotic leakage (AL), associated with strongly increased morbidity and mortality and incidence rates varying from 3% to 19%.1–4 In current practice, blood supply is evaluated peroperatively by means of clinical observations such as mucosal color, palpable pulsations, and bleeding from the marginal artery. However, these methods lack accuracy and objectivity, irrespective of a surgeon's experience. 5 Alternative approaches including the use of Doppler, laser speckle contrast imaging, and hyperspectral imaging have yet failed to reach clinical implementation, since no recommendation can be made regarding their applicability due to technical difficulties and low reproducibility.6–10 There is a need for objective and reliable peroperative detection of insufficient intestinal perfusion.
In recent years, fluorescence angiography (FA) has emerged as a promising tool for yielding intraoperative insight into local perfusion dynamics. FA involves the intravenous injection of contrast agent indocyanine green (ICG) and subsequent monitoring of its fluorescent appearance in bowel tissue. The role of FA in peroperative decision making during colorectal surgery has already been demonstrated.6,11–13 Furthermore, superiority of FA over judgment on clinical signs alone in the detection of perfusion impairment has been shown in experimental models.14,15 However, the acquired images are evaluated in a qualitative manner, making them sensitive to misinterpretation. In addition, multicenter randomized controlled trials failed to show a significant reduction in AL after peroperative implementation of FA.12,13,16 It becomes apparent that the current qualitative interpretation of FA is unreliable, creating the need for more objective quantification.16,17
Animal studies showed a great ability of quantified parameters to indicate blood flow and tissue ischemia.14,18 Quantification should be based on reproducible signal properties, meaning that circumstances other than tissue perfusion should not be influential. For this reason, the use of intensity-based parameters such as maximal intensity is not advised, since these depend on factors such as ICG dosing and the distance between tissue and camera. Time-based dynamics of the signal are more consistent. Parameter
This study presents a convenient and objective semiautomated method for the acquisition of peroperative quantitative parameters in FA. Moreover, as a first step toward a differentiating threshold value, the characteristics of the parameter
Materials and Methods
Data acquisition
A total of 33 patients who underwent robotic laparoscopic abdominal surgery were prospectively included in this study. No ethical approval was needed under the Dutch law on medical research on human subjects, and the need for informed consent was, therefore, waived. All procedures were performed by 1 surgeon in Medisch Spectrum Twente (MST) Hospital (Enschede). No patient presented clinical signs suggesting impaired intestinal perfusion. Patient characteristics including laparoscopy indication are presented in Table 1. In each patient, FA was performed on the small intestine as a minor extension to standard peroperative FA application. No clinical decisions were made based on the intestinal FA analysis. All FA recordings were obtained using the Firefly module in the Da Vinci X system (Intuitive Surgical, Sunnyvale, CA, USA) after manual intravenous injection of 5 mg ICG (5 mg/mL) and subsequent saline flushing.
Characteristics of Patients Who Underwent Fluorescence Angiography During Robotic Laparoscopic Surgery (n = 32)
Includes intraductal papillary mucinous neoplasms.
ASA, American Society of Anaesthesia; BMI, body mass index; SD, standard deviation.
Parameter extraction
A software tool for the quantitative analysis of FA recordings was developed in MATLAB R2019a (MathWorks, Natick, MA, USA). The main purpose of this tool was convenient quantification of FA with automated but user-supervised parameter extraction. The algorithm employed several steps. First, an intensity–time curve was determined by calculating the mean value of the green channel in a specific region of interest (ROI) for each timeframe. Signal noise was subsequently removed using a lowpass Butterworth filter (second order, cutoff frequency = 0.18 Hz). The following step was detection of the start- and endpoint of the intensity increase (T0 and

Filtered intensity–time curve of FA.
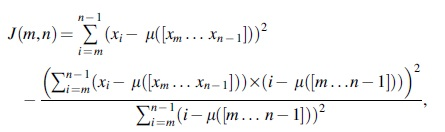
where
It is expected that the start- and endpoint of intensity increase are identified as one of these change points. Definitive designation of T0 and
The performance of the algorithm in the detection of T0 and
Patient analysis
The characteristics of
Results
FA was performed on a total of 33 patients, who all had a prosperous postoperative recovery. The recording of 1 patient was excluded from the analysis of
Algorithm performance
Among the 9 observers, ICC varied between 0.93 and 0.99 (95% confidence interval [CI]: 0.89–0.99) for T0. For
Patient analysis
A total of 32 patients were analyzed using the developed algorithm. In Figure 2, box plots are displayed that indicate the characteristics of

Box plots representing the measurements of
Figure 3 shows two examples of a cartogram automatically generated based on the value of

Discussion
This pilot study demonstrated that an automated approach in the quantification of FA for peroperative intestinal perfusion assessment including the characteristics of FA parameter
The ability of the change point detection algorithm was examined. Since there is no common consensus on the exact definition of
Automated analysis of
It should be considered that the single parameter
To clarify the correct interpretation of quantified FA and be able to identify inadequate perfusion, this study has to be expanded with more data. The presented approach is a substantial step toward an objective standardized method of analysis. When this is established, large scale data acquisition should be relatively straightforward. Naturally, the succeeding step would be to include patients with a known form of perfusion impairment. For instance, patients suffering from acute mesenteric ischemia (AMI) or chronic mesenteric ischemia (CMI) are certainly relevant. Indeed, one of the most important applications of FA is in the advanced stages of AMI or CMI.22,23 In case of transmural ischemia, bowel tissue is often surgically removed. It is very likely that the surrounding non-necrotic tissue is not properly perfused in this situation, increasing the risk of AL. A predictive threshold value in combination with the presented cartograms could be of great assistance in these circumstances.
A limitation in the current method is the lack of standardized admission of ICG. The rate and anatomical site at which the agent is injected influence the dilution in blood. This consequently affects intensity levels and fluorescence dynamics. It is, therefore, advised to investigate the use of an automated contrast injection system. Another presumably influential factor in the dynamics of ICG is cardiac output. In case of high cardiac output, it can be expected that time-based perfusion parameters improve. Future study should investigate the effect of cardiac output on quantified FA parameters and consider a possible correction. Finally, it is advised to examine the effects of temperature on FA parameters. Owing to consistent carbon dioxide insufflation, the temperatures during laparoscopy are expected to be similar. However, these conditions change when FA is applied in open procedures.
Conclusion
In conclusion, the presented semiautomated approach allows convenient analysis of FA recordings and can be of great assistance in the pursuit of threshold values to distinguish peroperative sufficient and impaired bowel wall perfusion. Clinical validation studies should be undertaken to underline that semiautomated FA analysis could reliably identify nonviable bowel tissue in gastrointestinal surgery.
Footnotes
Authors' Contributions
H.G.M.V., B.W., R.H.G., and D.J.L. designed the study. D.J.L. acquired data. H.G.M.V., B.W., R.H.G., and D.J.L. analyzed the data. All authors participated in data interpretation and article preparation.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.