
Abstract
Background:
Thoracoscopic diaphragmatic plication has gained popularity in the treatment of congenital diaphragmatic eventration (CDE), but the therapeutic effect and prognosis have rarely been compared with nonendoscopic surgery.
Materials and Methods:
The medical records of 77 children who had received treatment for CDE in our institution from September 2006 to January 2019 were retrospectively analyzed. According to the repair approach, the children were divided into a thoracoscopic plication group and a modified small incision plication group. The perioperative characteristics and follow-up details after diaphragm plication were compared between the two groups.
Results:
Among 77 children with CDE, 44 cases were in the thoracoscopic plication group and 33 cases were in the modified small incision plication group. All the cases of CDE were unilateral, with 13 cases on the left side and 64 cases on the right side. There were no differences in the preoperative characteristics between the two groups. The modified small incision plication group had a higher bleeding volume (P = .000) and a greater proportion of patients needing chest drainage (P = .000), whereas the differences in the total and postoperative hospital stays (P = .088, P = .247, respectively) did not significantly differ between the two groups. There were no differences in postoperative improvement in the location of the diaphragm between the two groups or between the right and left lesions (P = .438, P = .677, respectively). The total follow-up time was 2–11 years. No recurrence was reported during this period in either of the groups, but the incidence of postoperative thoracic deformities was higher in the modified small incision plication group (P = .013).
Conclusions:
Compared with the modified small incision plication, thoracoscopic plication has the advantages of smaller blood loss, a low percentage of intrathoracic drainage tube usage, and no occurrence of thoracic deformities.
Introduction
Congenital diaphragmatic eventration (CDE) is a rare entity characterized by a partial or complete elevation of the diaphragm caused by a congenital defect or acquired phrenic nerve injury during or after birth. Open transthoracic plication is the classical approach to treating patients with symptomatic diaphragm eventration or paralysis. 1 Recently, diaphragmatic plication through laparoscopy or thoracoscopy has become an acceptable alternative to the classical operative technique. 2 However, there have been no comparative studies of the thoracoscopic plication and modified small incision plication for the treatment of CDE. In this study, we focused on the comparison of the perioperative effects of the two approaches and tracked their long-term prognosis.
Materials and Methods
Study population
This study followed the Declaration of Helsinki and obtained informed consent from the children's families.
The clinical data of 77 children who had undergone diaphragmatic plication for CDE in our hospital from September 2006 to January 2019 were retrospectively reviewed and followed up until July 2020. There were 44 cases treated with thoracoscopic diaphragm plication (the thoracoscopic plication group) and 33 cases treated with modified small incision diaphragm plication (the modified small incision plication group).
The study population included 59 males and 18 females, with a median age of 6.75–21.60 months and a median weight of 8–12 kg at operation. There were 13 cases of left and 64 cases of right CDE. In all the patients, the diagnosis of CDE was confirmed by chest X-ray or computed tomography (CT), showing that the diaphragm on the affected side was raised by two to five intercostal spaces compared with the normal side. All the symptomatic children with CDE were operated after obtaining the informed consent from their families. There were no differences in gender, age, weight, lesion location, and degree of diaphragm elevation before operation between the two groups, indicating that the data of the two groups were comparable (Table 1).
Comparison of Clinical Characteristics Between the Thoracoscopy Group and the Modified Small Incision Group
Continuity-corrected chi-square test.
There were 69 cases with complete preoperative imaging data, including 42 cases in the thoracoscopy group and 27 cases in the modified small incision group.
IQR, interquartile range; M, median.
Operative technique
Surgical plication of the diaphragm was performed in symptomatic patients. The patients underwent diaphragmatic plication under general anesthesia in a lateral decubitus position. For modified small incision diaphragm plication, a 3–5 cm small incision was performed through posterolateral thoracotomy through the sixth or seventh intercostal space. The redundant diaphragm was gripped by forceps and interruptedly sutured along the forceps margin by #7 nonabsorbable suture with intracorporeal knots; then, the excessed diaphragm was covered and sutured to the normal diaphragm to complete diaphragmatic plication and reinforcement. Finally, a single intercostal drain was left in place, and the thoracotomy was closed in layers, especially including the closing of affected intercostal space.
For thoracoscopic diaphragm plication, after positioning the patient in the lateral position, CO2 was insufflated at 2–8 mm Hg pressure and 0.5 L/min flow to deflate the lung. Three ports were inserted: the camera port was placed in the fourth intercostal space in the midaxillary line, and working ports were placed in the fourth intercostal space on the anterior axillary line and in the fourth or fifth intercostal space on the posterior axillary line. Positions of the ports were adjusted for each patient. We explored the affected side of the diaphragm, lifted the diaphragm, and found the margin of the normal diaphragm. Both sides of the normal diaphragm edge were sutured with vertical mattress suture; then, as the modified small incision diaphragm plication, the excessed diaphragm was covered and sutured to the normal diaphragm.
Statistical analysis
All the analyses were performed using IBM SPSS Version 25 (SPSS, Inc., Chicago, IL). Continuous variables were presented as the median, 25th, and 75th percentiles and range, whereas categorical variables were shown as number and percentage. The Mann–Whitney U test was used to compare the non-normally distributed continuous variables between the two groups, and the chi-square test, continuity-corrected chi-square test, and Fisher's exact probability test were used to compare the categorical variables. A P value of <.05 was considered statistically significant.
Results
Perioperative outcomes
In Figure 1, representative chest X-rays demonstrate the location of the hemidiaphragm before and 1 week after plication. The elevated diaphragm returned to its normal position after plication in both groups. It is worth noting that after thoracoscopic diaphragm plication, the postoperative intercostal space was not affected; however, after modified small incision diaphragm plication, the intercostal space at the surgical site became narrow.

Representative chest X-rays in children with CDE.
As given in Tables 2 and 3, bleeding volume was higher (P = .000) and the proportion of patients needing chest tube was greater (P = .000) in the modified small incision group than in the thoracoscopy group. However, there were no intergroup differences either in the degree of diaphragm decline after surgery (P = .438) or in the length of total and postoperative hospital stays (P = .088 and .247, respectively). The postoperative improvement of the diaphragm did not differ between the left and right sides (P = .677).
Comparison of the Perioperative Outcomes Between the Thoracoscopy Group and the Modified Small Incision Group
The Degree of Diaphragm Decline After Surgery in Different Groups
IQR, interquartile range; M, median.
Postoperative follow-up and outcomes
Forty-seven children were followed up completely after the operation, including 26 in the thoracoscopy group and 21 in the modified small incision group. The duration of the follow-up was 2–11 years. We evaluated the chest X-ray 3 years after surgery; the position of the hemidiaphragm in both groups did not change significantly compared with the position at 1 week after surgery. There were three punctate scars and a linear scar left at the surgical site in the thoracoscopy group and the modified small incision group (Fig. 2). No thoracic deformities occurred in the thoracoscopy group. In contrast, in the modified small incision group, five cases (23.8%) had thoracic deformities at the surgical site 4–6 years after surgery, indicating that the incidence of thoracic deformities was higher in the modified small incision group than in the thoracoscopy group (P = .013). There was no relapse, rapid breathing, dyspnea, and repeated respiratory infections in either of the groups (Table 4).
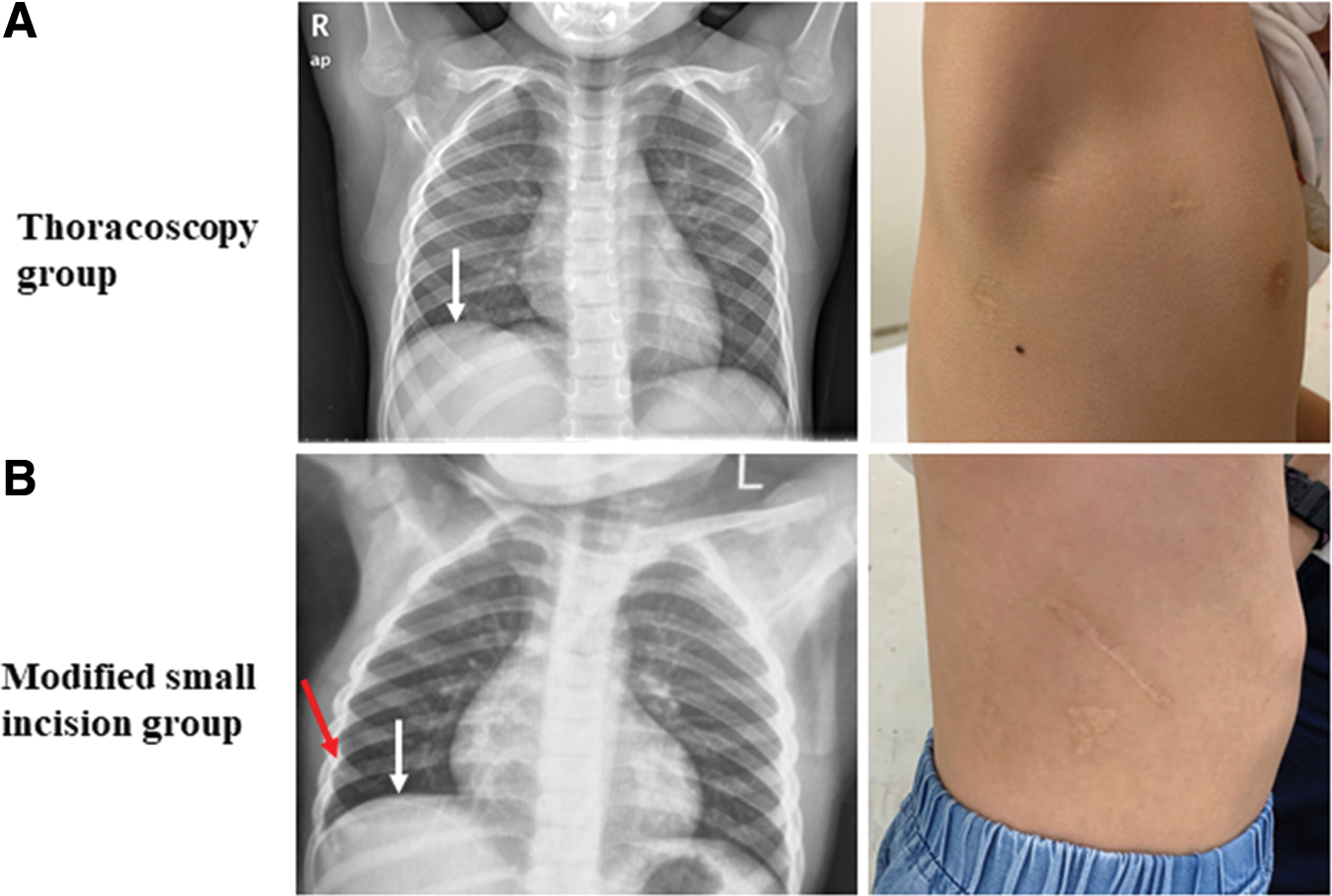
Representative chest X-rays and surgical scars 3 years after diaphragmatic plication.
Comparison of the Postoperative Outcomes and Follow-up Data Between the Thoracoscopy Group and the Modified Small Incision Group
Fisher's exact probability test.
Discussion
CDE is a rare developmental abnormality characterized by partial or complete muscular aplasia of the diaphragm. The normal diaphragm is replaced by a thin layer of fibrous tissue, which causes the bulging of the pathological diaphragm into the chest cavity, paradoxical movement of the hemidiaphragm, and reduction in homolateral lung volume. 3 Most children with CDE are asymptomatic and are accidentally discovered by chest X-ray examination. However, some children may have symptoms such as rapid breathing, dyspnea, vomiting, cough or expectoration, repeated respiratory infections, and even respiratory failure. There has always been a controversy as to whether asymptomatic children need surgery. Those who advocate surgery believe that the abnormally elevated diaphragm may hinder lung development; although the deviation of the mediastinum may not affect the lung dynamics in the short term, it causes serious damage to the lung function in the long term. 4 The current trend is that surgery is recommended for symptomatic patients but not for completely asymptomatic patients.
Diaphragm plication is a classic approach for the treatment of CDE; it can be performed as an open procedure or under endoscopy. 1 Open diaphragm plication includes transthoracic plication and transabdominal plication. Modified small incision diaphragm plication in our institution is performed through the transthoracic approach. In recent years, with the development and wide application of thoracoscopes, the thoracoscopic diaphragm plication has gradually matured. 2 A variety of minimally invasive transthoracic and transabdominal techniques have been described,5,6 and thoracoscopic diaphragm plication is used in our institution. It has been shown that surgical effects do not differ between transthoracic and transabdominal approaches. 5 Good therapeutic effects have been achieved both with open and with minimally invasive diaphragm plication.1,7 However, hitherto there have been no studies directly comparing the various diaphragm plication techniques. The main aim of our study was to compare the therapeutic effects between the modified small incision diaphragm plication and the thoracoscopic diaphragm plication.
Open transthoracic plication is the traditional approach to treat patients with symptomatic diaphragm eventration. Many reports have shown significant improvement in postoperative symptoms and the location of the diaphragm,7,8 and the improvement effect persists during long-term follow-up. 7 In the modified small incision diaphragm plication, only a small (3–5 cm) incision is used to complete the diaphragm plication; in this study, it was moderately modified while following the traditional thoracotomy method. An obvious improvement of clinical symptoms was observed, and there was no recurrence during the postoperative follow-up after this type of surgery. With the rapid development and wide application of minimally invasive surgery, its treatment effects have gradually achieved or even surpassed traditional open surgery in the treatment of many diseases, including tumors.9,10 Furthermore, minimally invasive surgery is characterized by small trauma, small surgical incision, less bleeding, and quick recovery.9–11 Thoracoscopic diaphragm plication is an excellent minimally invasive alternative to open transthoracic plication, and the long-term follow-up data suggest that it may be as effective as the open approach.2,12 In this study, we concluded that compared with modified small incision diaphragm plication, the thoracoscopy treatment had the advantages of smaller bleeding and less frequent need to place a thoracic drainage tube, but there was no significant intergroup difference in hospital stay.
An important difference between child surgery and adult surgery is that postoperative scars in children grow with increasing age. 13 Both the modified small incision and the traditional thoracotomy diaphragm plication use a longer surgical incision, and the ribs on both sides of the surgical incision are tied and fixed when the chest is closed. In the process of children's growth, the traction of scars and the restriction of rib growth and movement may cause thoracic deformities. Indeed, the thoracic deformity is known to occur after thoracotomy performed during childhood. 14 At present, there are no reports on CDE-related thoracic deformities. In this study, a follow-up of thoracic deformity of the two groups revealed that 5 children developed convex or concave deformities at the surgical site 4–6 years after surgery in the modified small incision diaphragm plication group, whereas no thoracic deformities occurred in the thoracoscopy group. This reminds us that in children, in addition to focusing on the improvement of CDE symptoms under different surgical procedures, we should also assess whether surgical scars and rib banding could negatively affect the growth and development.
Conclusions
In conclusion, our data on the treatment of CDE show that thoracoscopic diaphragm plication has the advantages of less bleeding and less frequent placement of thoracic drainage tube, but there is no significant effect on the hospital stay. The long-term follow-up results show that there is no postoperative recurrence in either of the two groups, and thoracoscopic treatment can avoid the occurrence of thoracic deformities. At present, thoracoscopic diaphragm plication is relatively mature and should be recommended first if conditions and technology are feasible.
Footnotes
Disclosure Statement
All authors have seen and approved the final version of this article. No competing financial interests exist.
Funding Information
No funding was received for this article.