
Abstract
Background:
The face mask has been used to protect against airborne diseases throughout history. We conducted a historical review of the literature on the origin of the face mask, the scientific evidence of its benefits, and its implications for domestic and international politics.
Material and Methods:
We performed a comprehensive search for peer- and nonpeer- reviewed literature published between 1905 and 2020.
Results:
Face mask wearing in hospital settings to prevent disease transmission from health care workers to their patients originates with the first use of the mask in surgery in 1897 by German surgeon Johann von Mikulicz. During the first half of the 20th century, various scientific investigators focused on determining the most effective type of medical mask. The role of the face mask in the general population as a preventive intervention during public health emergencies is supported by historical reports spanning from the European Bubonic Plague in 1619, to the Great Manchurian Plague of 1910–1911, the influenza pandemic of 1918, and the current coronavirus disease in 2019 (COVID-19) pandemic. Although the face mask has helped against airborne disease transmission, its benefits during pandemics have been filtered through the prism of political leanings and geopolitical interests.
Conclusions:
Our review suggests that while face mask alone cannot stop pandemics, in conjunction with other nonpharmacologic interventions it can be useful in mitigating them. When cooperation rather than division becomes the norm in the global response to pandemics, the face mask can then unite rather than divide us.
Introduction
The face mask has become the most visible symbol of the fight against the ongoing worldwide coronavirus pandemic. The purpose of this review was to provide a historical perspective of the face mask's fascinating scientific and political history.
Material and Methods
A diverse team of authors, including general surgery resident and attending surgeons conducted a historical review of the literature on the origin of the face mask, the scientific evidence of its benefits, and its implications for domestic and international politics.
We conducted a nonsystematic search for peer- and nonpeer-reviewed literature published between 1905 and 2020. Reference lists of articles were reviewed to identify additional studies.
The entire team of authors identified key findings in the literature related to the face mask, and the final results are the key points presented in this review. According to the VA Boston Healthcare System policy, our study was exempt from Institutional Board Review.
Results/Discussions
The origin of the face mask use in surgery and hospital setting
The face mask was first used in surgery in 1897 by Dr. Johann von Mikulicz, head of the surgery department of the University of Breslau (now Wroclaw, Poland), and consisted of a single layer of gauze tied to the cap with two cords which covered the nose, mouth, and beard. 1 His decision to use the mask was based on the work of his bacteriologist colleague, Carl Flügge, who had demonstrated that tuberculosis was spread by airborne respiratory droplets as observed by bacterial growth on agar plates placed in the operating room. 2
In 1898 Mikulicz’ assistant Hübner demonstrated that a double layer of narrow-meshed hydrophilic gauze would increase the efficiency of the mask. 3 In addition, he realized that given the close contact between the gauze and the mouth, the mask collected moisture and became contaminated with saliva. To keep a distance between the mask and the mouth, Hübner then created a new, sterilizable mask consisting of double layer of hydrophilic gauze stretched over a wire frame extending from the nose to the chin. 3
Over the next several decades, various investigators focused on confirming the value of face masks in protecting against contagious diseases and determining the most effective type of gauze mask.4–7 Their work is summarized in a chronological order in Table 1.
Studies Conducted Between 1905 and 1961 on the Benefits of Face Masks in Protecting Against Contagious Diseases and the Effectiveness of Gauze Mask
Although historical commentaries suggest that the use of face masks during operative procedures became general practice by the late 1920s,4–7 there are no clear data to identify when the face masks achieved widespread acceptance in surgery.
An analysis of >1000 historical operating room photographs from 1863 to 1969 by Adams et al. 26 showed that the probability that a surgeon would be wearing a mask was 50% between 1913 and 1919 and increased to 99% by 1964.
Beginning in the early 1960s, disposable masks made of nonwoven synthetic fibers were first introduced in the United States and subsequently disseminated worldwide. After the transition to single-use masks, the production of reusable masks halted because they were considered inferior to industrially produced disposable masks. 27 Single-use masks were made of different fiber materials such as polypropylene, polyester-rayon, and cellulose. 28 Subsequent investigations and developments focused on improving the efficiency of different types of materials used in disposable masks.
The use of the face mask in the general population
The use of face masks to protect against contagious diseases has a long history. Although it remains unclear when the first masks were used in the general population, we are presenting a historical timeline of documented reports of face masks being used for protection against airborne diseases.
European bubonic plague
Bubonic plague is an infectious disease caused by Yersinia pestis, a zoonotic bacterium that is transmitted between animals by fleas and can also spread from animals to humans. The bubonic plague has a long history in the European continent and most historians think that the bubonic plague killed 50 million people, ∼60% of Europe's entire population between 1347 and 1351. 29 The bubonic plague continued to cause recurring outbreaks throughout Europe in medieval times. 30
It was during one of these outbreaks in 1619 in France that Charles de Lorme, the chief physician to King Louis XIII, developed a protective leather outfit that included boots, breeches, a long coat, hat, gloves, and a long (15 cm) beak mask complete with crystal eyepieces. 31 At that time it was considered that the bubonic plague spread through “pestilential miasma,” a contagious bad odor created by decay and coming directly from the patient. As such, the long beak of the mask was filled with perfume, dried flowers, or aromatic herbs to prevent the inhalation of the “miasma.”
Historically, this is considered the first report of a mask intended to prevent an airborne disease. The first documented illustration of this mask (Fig. 1) was created during a deadly plague outbreak in Italy in 1956 by the German engraver Gerhart Altzenbach, who depicted a Roman plague doctor in full outfit, with text describing how the clothing protected against the plague. 32

The Bubonic Plague doctor costume as engraved by Gerhart Altzenbach. Credits: Wikimedia Commons.
Although the miasma theory proved to be incorrect, the use of the face mask and protective clothes suggests that efforts were being made to better understand transmission of contagious diseases and protect public health during pandemics.
The Great Manchurian Plague (1910–1911)
In the fall of 1910, a deadly disease broke among tarbagan marmot hunters in Northern Manchuria, modern day northeast China. The devastating disease caused fever, hemoptysis, and a purplish skin discoloration, and had a fatality rate nearing 100% in 1–2 days. Given the rapid spread of the disease, the Chinese emperor assigned Dr. Wu Lien Teh to intervene. After performing an autopsy on one of the victims, Dr. Wu found Y. pestis in the lungs, concluding that pneumonic plague was the cause of the epidemic. 33 He realized that hunters contracted the disease from infected tarbagan marmots and then spread it through airborne droplets. To prevent transmission of the disease he urged people to wear his “anti-plague mask” 34 made of cotton and gauze (Fig. 2).
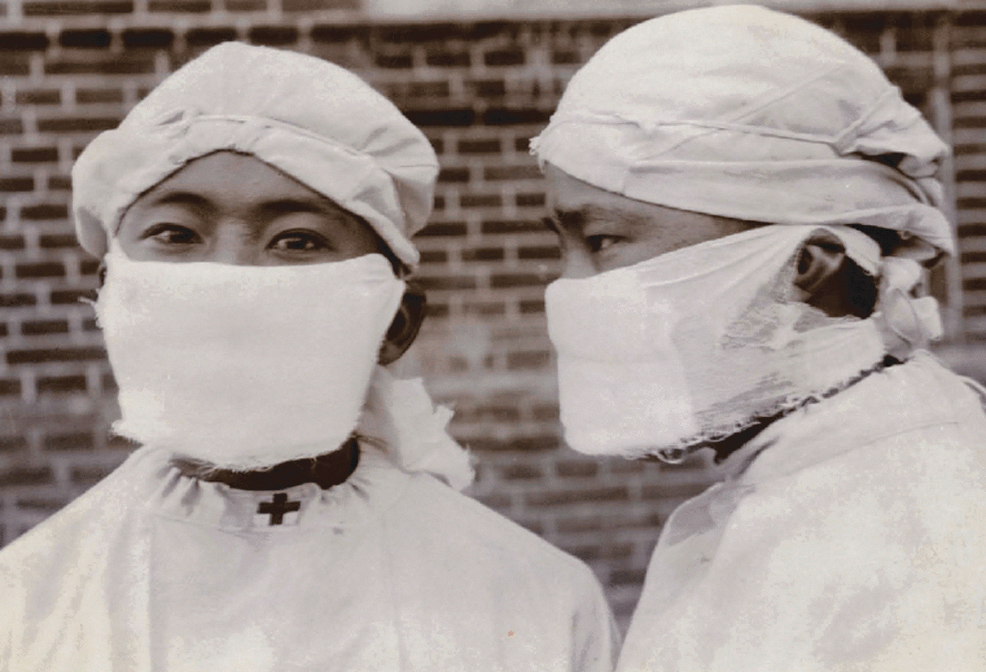
Front and side views of the Manchurian anti-plague mask. Credits: The University of Hong Kong Libraries.
However, Dr. Wu's conclusions were initially contested because until then, the only form of plague known to affect humans was the bubonic plague, carried by fleas from rodents to humans, without spreading from person to person. 35 As such, on January 11, 1910, a well-known plague expert from France, Dr. Gérald Mesny, was sent to the area to replace Dr. Wu as the person managing the epidemic. Because Dr. Mesny ignored Dr. Wu's strong recommendations for wearing a mask when treating patients, he died from the plague in a few days. His death caused panic and convinced the Chinese government to institute Dr. Wu's plan for controlling the epidemic that consisted in lockdowns, quarantines, mask wearing, travel restrictions, cremation of victims, and border controls. 35 Soon thereafter, almost everyone on the streets was wearing a mask. 36 The outbreak killed ∼63,000 people by the time it concluded in March of 1911, making it one of the world's largest epidemics at the time.
Mask wearing was the most visible measure in controlling the spread of the pneumonic plague and is considered to be the first use of a mask as a public health measure against airborne disease transmission. Dr. Wu was widely praised for his efforts in controlling the outbreak, and in 1935, he became the first Chinese physician to be nominated for a Nobel Prize. 35
The Great Manchurian Plague had also significant geopolitical implications. 37 When the pneumonic plague broke out in Manchuria in 1910, the Qing Dynasty (1644–1912) was weak and on the verge of collapse. While most of the sparsely populated Manchuria's territory was Chinese-governed, Japan controlled the port area around Dalian and Russia was running Manchuria's railways. Furthermore, European powers and the United States had treaty ports throughout the country.
Russia and Japan were interested in controlling the disease outbreak because they feared that the plague would affect their residents living in Manchuria, spread to their contiguous territories, and damage their commercial interests. 38 Furthermore, taking control of the epidemic was a strategic opportunity for Russia and Japan to expand their colonial possessions in Manchuria.37,38 By taking charge of the epidemic response and successfully ending the outbreak, Dr. Wu's interventions allowed China to protect its sovereignty.
China's role in preventing the pneumonic plague from spreading across Asia and the world was also recognized in the 1911 Mukden (modern-day Shenyang) Conference—the first international scientific conference held in China and dedicated to the understanding the pneumonic plague and its prevention.
The conference had two critical outcomes. First, it created the North Manchurian Plague Prevention Service in 1912, which aspired to develop a public health system for the entire China. 39 Second, the conference brought together resources, knowledge, and scientists from around the world and facilitated collaboration between Chinese and foreign governments and doctors. This collaboration highlighted the need for transnational coordination of governmental responses for responding to epidemics.
The influenza pandemic (1918)
The influenza pandemic of 1918 was the deadliest flu outbreak in history. Over the course of 2 years, it killed 675,000 people in the United States and 50 million people worldwide, 40 far exceeding deaths from the First World War (1914–1918). Although titled the “Spanish Flu” the pandemic did not start in Spain and its origin remains unknown. Whereas countries fighting in the First World War censored news that could affect morale and war efforts, Spain was a neutral country and the first country to publicly report the influenza outbreak, 41 creating a misperception that it originated in Spain; hence the nickname “Spanish Flu.”
As the influenza started to spread rapidly across the United States in the fall of 1918, local governments instituted policies to contain the outbreak. These interventions varied by region, and included closing schools and businesses, prohibiting public gatherings, quarantining infected people, using disposable tissues, enforcing “no-spitting” ordinances, and requiring people to wear masks in public. 41
Initially the U.S. public health authorities recommended the use of medical gauze masks only for health care providers taking care of influenza patients. However, as the influenza cases rose rapidly, in mid-October of 1918 the U.S. Public Health Service recommended that all citizens wear a mask. These recommendations were coupled with efforts by the public health authorities and the media encouraging mask wearing and providing instructions on making masks at home using gauze and cotton string (Fig. 3). Furthermore, authorities and media framed mask wearing as a wartime patriotic duty to help protect U.S. troops from the deadly outbreak. 42

Gauze and cotton string mask used during the Influenza Pandemic of 1918. Credits: The Oakland Museum of California.
Several Western U.S. states went further and imposed mandatory ordinances requiring masks in public. Violators were ticketed, fined, and even imprisoned.
However, the mask recommendations and ordinances were eliminated in November 1918 after the First World War armistice as the number of cases and deaths decreased. The relaxation of the mask wearing requirements led to a surge in the cases of influenza and a second mask mandate in some states.
Although most people initially complied with mask use, opposition to mask wearing increased following the institution of the second mask mandate. In a notable example, after the city of San Francisco instituted a second mask ordinance on January 17, 1919, the Anti-Mask League was created with members including physicians, lawyers, civil rights activists, and other citizens. 43 They asserted that there was no scientific evidence that masks were effective and that mask mandates were unconstitutional and infringed on civil liberties. 44 Given the growing opposition to the mask ordinance and the lack of measurable benefits, San Francisco ended the mask mandate on February 1, 1919.
Whether the mask use during the influenza pandemic of 1918 was effective in reducing casesa and deaths remains open to historical debate. Studies performed by public health organizations during the pandemic found no significant differences in influenza infections and deaths between cities that mandated the mask wearing in public and cities that did not, suggesting that mask mandates were not effective.45,46
Subsequent studies on mask wearing in the first years after the pandemic suggested that the reason for the perceived lack effectiveness was the lack of real-life compliance and improper mask use.47,48 Some examples included improperly constructed masks at home (using cheesecloth and other materials instead of the recommended medical gauze with tighter weave); masks used until they were soiled; masks worn incorrectly; and even the creation of holes in the mask to allow for smoking.
A more recent analysis demonstrated that the consequences of the 1918 influenza pandemic in the United States were mitigated in places that in addition to mandating mask wearing, instituted early, sustained, and multilayered public health interventions that included closing schools and businesses, prohibiting public gatherings, quarantining of infected people, transportation restrictions, public risk communications, and hygiene education. 49 These findings suggest that mask wearing alone was not enough to prevent the spread of the influenza pandemic.
The influenza pandemic of 1918 had several important geopolitical consequences throughout the world. Because all nations fighting in the First World War lost a devastating number of soldiers to the disease in the final months of the war, historians agree that the 1918 pandemic accelerated the end of the war, with the armistice being signed on November 11, 1918 amid the worst surge of the pandemic. 50
The pandemic also interfered with the peace process as it affected many of the participants to the Paris Peace Conference in April 1919. This was particularly important for the U.S. President Thomas Woodrow Wilson, as the president of the most powerful country at the end of the First World War. Before the Conference Woodrow Wilson had outlined The Fourteen Points, a statement of principles to be used for the peace negotiations. 51 The principles consisted in free trade, open diplomacy, a new balance of European power, and institution of the League of Nations—an international body to prevent future conflicts. Woodrow Wilson also advocated for a nonpunitive approach for Germany, to ensure a fair and lasting agreement. However, President Wilson contracted the influenza and became physically ill on April 3, 1919 while attending the conference. He was confined in bed for 5 days with a 103° fever and cough while the press was told that it was just a bad cold. 52 Historians believe that the lingering mental and physical weakness caused by the flu may have hindered Wilson's ability to effectively advocate for his Fourteen Points after he rejoined the conference. 53 This allowed French Prime Minister Georges Clemenceau to advance measures that were very different from Wilson's Fourteen Points. As a result, the Treaty of Versailles that was signed in June 1919 included measures against Germany that were so punitive and restrictive that caused economic devastation for German people after the First World War.
Historians agree that the humiliation and economic desperation inflicted on the German people by the Treaty of Versailles revived German nationalism and contributed to the rise of Adolf Hitler. 54
The 1918 influenza pandemic also played a crucial role in India's struggle for independence. In British-occupied India, the influenza pandemic of the 1918 caused more than 18 million deaths, the greatest loss of any country in the world. 55 Mahatma Gandhi, the leader of India's independence movement, was one of the millions who contracted the flu.
The British government officials protected themselves but did not take sufficient measures to prevent the spread the disease among the Indian population. This negligence increased anti-colonial sentiments and caused widespread resentment among the Indian people and gave an opportunity to the Indian nationalist movement to fill the void by distributing supplies to the infected people and managing the crisis. These events brought Indian people together and accelerated their fight for independence. 55
The 1918 influenza pandemic was an important turning point for public health in the United States and the world. Before the pandemic, health care was very fragmented, and it was widely considered that people who caught infectious diseases lacked personal responsibility and were at fault for getting sick. The pandemic revealed that the poor, immigrants, and racial and ethnic minorities were more affected by the pandemic owing to crowded living conditions, comorbidities, and poor access to health care. 55 This led to a new understanding of the importance of managing the contagious diseases at the population level and a rethinking of public health strategies. As a result, in the 1920s, many countries expanded access to health care for the general population either by adopting centralized health care systems (such as in Russia and Western Europe) or employer-based insurance plans (such as in the United States).55,56
Countries also recognized the need to coordinate their public health policies at the international level to prevent the spread of contagious diseases in an increasingly interconnected world. 55 This new cooperation started with the creation of an international bureau for fighting epidemics in Austria in 1919 and continued with the establishment of the League of Nations Health Committee and Health Section in 1922. With the outbreak of the Second World War, international health cooperation came to a standstill until the foundation of the World Health Organization (WHO) on April 7, 1948.
The coronavirus disease 2019 pandemic (2019)
The rapid global outbreak of coronavirus disease in 2019 (COVID-19) has created an unprecedented public health crisis. COVID-19 is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is a highly transmissible respiratory virus causing upper and lower respiratory tract infection leading to a high viral load in respiratory secretions and saliva. The primary route of transmission of SARS-CoV-2 is airborne, likely through small droplets that are ejected when speaking, coughing, sneezing, and even singing. As such, the use of face masks has taken a central role in the efforts to reducing transmission of infected droplets.
Early in the pandemic, it was believed that only infected patients who are symptomatic could transmit the SARS-CoV-2. Given the initially limited data on asymptomatic transmission and concern about mask shortages for health care workers, both the WHO and the Centers for Disease Control and Prevention (CDC) recommended that only patients symptomatic for suspected COVID-19 should wear a face covering.
However, after substantial evidence of transmission of SARS-CoV-2 in the community from persons without symptoms, both the WHO (in July 2020) and the CDC (in April 2020) started to recommend the voluntary use of face masks by the general public, while at the same time emphasizing the use of cloth masks to preserve the supply of medical masks and N95 respirators for health care workers. 57 These conflicting guidelines about public wearing face masks during the COVID-19 pandemic created confusion about the value of widespread masking in mitigating the transmission of SARS-CoV-2.
Universal masking during the COVID-19 pandemic has become one of the most contentious issues throughout the world. 58 Among mask-related controversies, the effectiveness of different types of masks both in the laboratory setting and at a population level remains the most strongly debated.
Effectiveness of mask in the laboratory
Like many other respiratory viruses, the SARS-CoV-2 is thought to be transmitted through infected expiratory particles in the 1- to 10-μm range. There are several laboratory studies that have evaluated the ability of face masks to filter particles around that size range. Some of their findings are summarized in a chronological order in Table 2.
Studies Conducted Between 1983 and 2020 on the Filtration Effectiveness of Different Face Masks Against Expiratory Particles
Overall, these laboratory studies suggest that the filtration effectiveness of cloth masks is generally lower than that of surgical masks and N95 respirators. However, when used correctly cloth masks can provide an important tool for reasonable protection in the community when medical masks are unavailable. The performance of cloth masks may be improved by using water-resistant material with a high number of threads and finer weave and increasing the number of mask layers.
Effectiveness of face mask at the population level
The fast-spreading nature and the immense scale of COVID-19 pandemic represent an enormous challenge for generating rapid epidemiologic data to inform evidence-based and timely decision making about the widespread use of the mask.
Furthermore, it is ethically challenging and methodologically difficult to develop and conduct adequate randomized clinical trials during pandemics given the urgency of the situation.
In such circumstances, to obtain information for mask benefits in the general population, scientists have focused on observational studies from natural experiments during the current pandemic, as well as past outbreaks of other respiratory viral diseases.
A natural experiment describes an event or intervention not under the control of researchers, who then can analyze the outcomes to infer causality. 69 Hence, natural experiments can play a crucial role in evaluating large-scale population health interventions in the setting of pandemics. In one example of such a natural experiment, Lyu and Wehby 70 evaluated the effects of state government mandates for face mask use in public issued by 15 U.S. states plus Washington, D.C., between April 8 and May 15, 2020. The study found that mandating face mask use in public was associated with a decline in the daily COVID-19 growth rate by 0.9, 1.1, 1.4, 1.7, and 2.0% points in 1–5, 6–10, 11–15, 16–20, and 21 or more days after state face mask orders were signed, respectively. 70 These results are significant as they represent between 16% and 19% of the effects of other social-distancing measures such as school closures; bans on large gatherings; shelter-in-place orders; and closures of restaurants, bars, and entertainment venues.
Another study from Germany reported that face masks reduced the number of newly registered SARS-CoV-2 infections between 15% and 75% over a 20-day period after their mandatory introduction. 71 Overall, the authors estimate that face masks reduce the daily growth rate of reported infections by ∼47%.
On a global scale, Leffler et al. 72 analyzed the public wearing of masks from 196 countries and found that in countries not recommending masks, the per capita mortality tended to increase each week by 62.1%. In contrast, in countries recommending masks, the per capita mortality tended to increase each week by just 15.8%.
Despite substantial indirect evidence supporting an important role of widespread face masks in reducing the transmission of SARS-CoV-2, absolute scientific certainty about the benefits of the face mask it not easy to achieve in the context of a novel contagious disease with dramatic consequences and no standard treatment. This raises an important ethical question with significant implications: Should researchers, physicians, and decision makers expect absolute scientific proof before making public health decisions about mask wearing at a time when the COVID-19 is spreading quickly, causing a staggering number of deaths, overwhelming health care systems, and ravaging economies all over the world?
The answer to this question lies with the precautionary principle that guides decision-making when consequences of an activity are difficult to predict. 73 The precautionary principle emerged in the 1970s as an anticipatory approach to protect the environment against potentially irreversible and unknown long-term effects of climate change. 73 Since then, the precautionary principle has spread to other nonenvironmental areas, including health protection, and is supported by the proponents of widespread face mask use during COVID-19.74,75 They are increasingly advocating for policy makers to not use the lack of full scientific certainty as a reason for postponing widespread faced mask use as a preventive intervention during such a severe pandemic. Based on the best scientific evidence available, there is good reason to believe that not wearing mask in the public might be harmful by increasing the transmission of SARS-CoV-2. Furthermore, the anticipated benefits of the face mask use in the community outweigh any potential downsides of wearing the mask. 76
Concerns that the use of precautionary principle during the COVID-19 pandemic could serve as a blanket justification for curbing civil liberties are unfounded. Messerschmidt 77 has demonstrated that the precautionary principle during COVID-19 does not exceed the limits of what is appropriate and necessary to prevent the spread of SARS-CoV-2.
Politicization of the face mask
Since the beginning of the COVID-19 pandemic, the face mask became the most powerful political symbol throughout the world. As a result, the debate on the benefits of mask wearing remains a deep partisan issue causing significant political polarization.
In the Unites States, while most other protective measures against COVID-19 get broad bipartisan political support, mask wearing is seen through the prism of party politics. Adolph et al. 78 demonstrated that state governor's political affiliation was the most significant driver for the timing of a state's mask-wearing mandate. This political messaging along party lines has caused a partisan divide in the general public's likelihood of wearing masks. 79 Of importance, partisan differences in the COVID-19 response are associated with higher COVID-19 infection and mortality rates. 80
Comparative political studies have also shown that federalism and presidentialism have further exacerbated the political influence over the COVID-19 response.81,82
Coordinating and balancing federal and state power is crucial for adequately responding to emergency public health crises. However, opposing political affiliations of federal and state leaders has hindered the mask wearing mandates and the overall response to COVID-19 in some federalist countries such as Italy, Spain, Brazil, Russia, and the United States. 81 The lack of an absolute hierarchy and a loose federal-state coordination in these countries forced subnational governments into leading roles and produced state-level responses that likely saved lives. 81
Along similar lines of inadequate central–local coordination, at the beginning of the COVID-19 pandemic, European Union (EU) suffered from a lack of coordination and solidarity among its member countries. Several EU countries implemented national controls to restrict the export of face masks and protective clothing, including other member countries. Although later the EU Commission discouraged member countries on such limitations of intra-EU trade, 83 it has proven challenging to maintain a comprehensive pan-EU response to COVID-19 when national governments are left facing the pandemic without support. 84
Presidentialist countries have a propensity to authoritarian actions and stalemates. 85 For example, in the United States and Brazil, the relationship of the president with state leaders during the COVID-19 has been fraught with tensions and antagonism, 81 which can undermine an effective country-wide response.
Significant attention is also being brought to the relationship between the type of regime and the COVID-19 response, as well as answering a very consequential question: Do authoritarian or democratic systems respond better to pandemics?
In autocracies, centralization of power has allowed governments to take more forceful actions by introducing harsher lockdowns regardless of social costs and human rights, curtailing civil liberties, using more privacy-intrusive contact tracing, and suppressing critical information.81,86,87 Whereas decentralization of power in democracies can potentially slow the initial response to public health emergencies, democracies have been shown to be more resilient and better at promoting transparent information, reducing geographic mobility in their countries to curb the spread of the virus, building high level of public trust, and increasing the capacity for innovation and adaptation.81,86,87 Although democracy is the best form of government for surviving pandemics, there is room for improvement, and lessons from the COVID-19 pandemic should stimulate democratic political systems to become more accountable, efficient, and responsive. 88
International “mask diplomacy” and geopolitical consequences
By early March 2020 China was able to largely contain their SARS-CoV-2 outbreak, and the epicenter of the COVID-19 pandemic shifted from China to Western Europe and subsequently to the United States and the rest of the world. The rapid global spread of the outbreak caused a significant shortage of face masks and other medical equipment, with the demand far exceeding their global supply, at a time when China was the largest producer of face masks, with 44% of the world's exports of face masks originating from China in 2018. 89
To boost its image and regain international trust after being criticized about the initial handling of the COVID-19 outbreak, the Chinese government started shipping face masks and medical supplies to countries in Asia, Europe, Africa, Latin America, the Caribbean, and even in some United States communities—an effort known as “mask diplomacy.”
Political scientists believe that in addition to representing itself as a responsible global leader, the Chinese government is also using mask diplomacy to pursue geopolitical goals.
In Southeast Asia, Beijing's mask diplomacy has focused on highlighting its positive image and promoting the notion of a generous Beijing to increase its influence in the region. Beijing's emphasis on public gratitude and expected reciprocity is intended to convince Southeast Asian countries to support China's growing influence in the region. 90
Following China's example, other Asian countries have used mask diplomacy to further their geopolitical goals. Thus, Taiwan has donated face masks and medical supplies to Europe, the United States, Japan, and diplomatic allies to increase international recognition and counter the Chinese government's campaign to block Taiwan from participating in international organizations such as the WHO. 91 Vietnam has also shipped face masks to Europe and neighboring countries to boost its profile and counter China's growing influence in the South China Sea region. 92
In Europe, by providing face masks and medical supplies to those European countries that are friendly to the Chinese government, Beijing is hoping to achieve political and popular credibility that would then translate in support for more Chinese investment and for the Belt and Road Initiative (sometimes referred to as the New Silk Road)—a massive infrastructure project that would stretch from East Asia to Europe and increase its political influence.93,94 Increased political and economic influence in Europe could weaken its relationship with the United States and create a geopolitical buffer zone between transatlantic alliance and Russia. 90 To counteract the Chinese government's mask diplomacy and defend against political fragmentation, the EU has increased efforts to coordinate the COVID-19 response among its member countries, as well as provide pan-European financial solidarity during the pandemic.
Through delivery of face masks and medical assistance, the Chinese government is also seeking to expand and cement its economic and political interests in Africa and counter the traditional U.S. influence in Latin America and the Caribbean.
In such a difficult time for the global health, one of the unfortunate casualties of the geopolitical competition among great world powers is the WHO. The WHO faced significant criticism over its slow response to the pandemic, its perceived deference to the Chinese government, and withholding important health information from Taiwan. 95 This led to the United States deciding to withhold U.S. funding for the WHO while reviewing its COVID-19 response. In a competition for global health leadership, the Chinese government has voiced increased support for constructing a Health Silk Road that would aim to create a public health network between the countries along China's Belt and Road Initiative. 96 On the contrary, in the United States there have been calls to establish an alternative global health institution free from the Chinese government's influence. 95
Conclusions
This historical review illustrates the long journey of the face mask from scientific validation of its utility against airborne disease transmission, to becoming a scapegoat for domestic politics, and just another tool for geopolitical competition. Mask use alone cannot stop pandemics, but in conjunction with other nonpharmacologic interventions can be useful in mitigating them. When cooperation rather than division becomes the norm in the global response to pandemics, the face mask can then unite rather than divide us.
Footnotes
Acknowledgment
The authors thank Eliora M. Kristo and Elis A. Kristo for their assistance with the literature search for this review.
Authors' Contributions
Conception and design of study: G.K., P.M.F.; Acquisition of data: G.K., K.H.; Analysis and/or interpretation of data: G.K., K.H, E.W., P.M.F.; Drafting the article: G.K., P.M.F.; Revising the article critically for important intellectual content: G.K., K.H., E.W., P.M.F.; Approval of the version of the article to be submitted: G.K., K.H., E.W., P.M.F.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.