
Abstract
Background:
Restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) is the procedure of choice for patients with ulcerative colitis and select patients with Crohn's disease. Minimally invasive techniques have been increasingly adopted including the transanal approach. However there remains a dearth of comparative data assessing the technical advantages and outcomes of a transanal approach to the IPAA against other minimally invasive techniques.
Methods:
In this review, we describe our learned approach with the transanal IPAA (ta-IPAA) and highlight key technical steps for a successful surgery in addition to evaluating the current literature on surgical and functional outcomes of this relatively novel procedure.
Results:
The ta-IPAA affords better visualization and access during a pelvic dissection translating to lower conversion rates. Lower odds of postoperative morbidity have been reported, but there was no difference in severity of complications when present. Though this technique has the advantages of a more accurate rectal transection obviating the need for multiple staple firings, the risk of anastomotic leak was similar between the two groups. Functional outcomes were found to be overall similar, though data is limited.
Conclusions:
The technical aspects of the IPAA have continued to evolve to mitigate the challenges posed by a deep pelvic dissection. While the ta-IPAA has been shown to be a safe and feasible procedure, the true advantages and functional benefits of this technique have yet to be elucidated with large-scale, quality data.
Introduction
The restorative proctocolectomy and ileal pouch-anal anastomosis (IPAA) procedure, described first by Parks and Nicholls in 19781 for use in patients with ulcerative colitis, has since been adopted for use in patients with indeterminate colitis, familial adenomatous polyposis and selectively in Crohn's disease patients. While IPAA offers good long-term functional outcomes for a large majority of patients who retain their pouch,2,3 technical aspects of the IPAA procedure continue to evolve to minimize pouch-related complications and optimize function and quality of life.
The use of minimally invasive surgery (MIS) for the IPAA procedure has become increasingly more common than the traditional open approach4,5 and provides a number of short-term advantages such as reduced pain, shorter hospital stay and post-operative recovery.4–6 Long-term benefits of laparoscopic IPAA also include improved cosmesis and body image, 7 lower risk of adhesive disease 8 and hernias, shorter operative time and faster recovery in subsequent ileostomy closure 9 and improved female fertility and fecundity.10,11 Though MIS has proven benefits over an open approach, the learning curve of laparoscopic pouch surgery is steep and conversion rates to an open approach are variable in the present literature, between 6% and 23.8%.6,12 The ideal MIS IPAA procedure is still under development as evidenced by the common use of a hand-assisted 13 or a hybrid combined open approach with a Pfannenstiel incision to facilitate the pelvic dissection.6,14
More recently, application of a transanal approach to the rectal dissection during an IPAA for ulcerative colitis or other benign pathologies has been proposed to mitigate the technical challenges inherent in operating deep in the pelvis and performing a precise low rectal transection and pouch anastomosis.15–17 Early results of the transanal IPAA (ta-IPAA) have demonstrated its safety and feasibility,18,19 irrespective of patient factors such as obesity or a narrow male pelvis, and even reduced morbidity in one European series. 20 Other technical advantages of the ta-IPAA may include a more precise distal rectal transection which obviates the use of multiple staple firings and risk of anastomotic leaks, 21 and direct visual evaluation of the level of the anastomosis. The use of a two-team approach has also been suggested to lower conversion rates and decrease operative times.22,23 Herein, we describe our operating room set-up and two-team coordination for a total proctocolectomy with ta-IPAA, while highlighting key technical aspects and intraoperative decision points of the procedure.
Technique
Operating theatre setup
A large operating theatre is ideal to accommodate the necessary equipment and facilitate the circulation of personnel. To accommodate two teams working simultaneously, two sets of instruments and two laparoscopic towers with monitors, cameras, and insufflation are needed (Table 1).
Equipment Suggested for Two-Team taTME Approach
Lone Star Retractor System (CooperSurgical, Inc., Trumbull, CT).
ENDOEYE II 10 mm, 30°, rigid video laparoscope (Olympus, Center Valley, PA).
ENDOEYE FLEX 10 mm articulating tip video laparoscope (Olympus).
Airseal (Conmed, Inc., Utica, NY).
Laparoscopic trocars rounded tip with balloon (Applied Medical, Inc., Rancho Santa Margarita, CA).
GelPOINT® Mini Advanced Access Platform (Applied Medical, Inc.).
GelPOINT Path Transanal Access Platform (4 × 5.5 cm) (Applied Medical, Inc.).
Ligasure™ (Medtronic, Inc., Minneapolis, MN).
Endopath® Probe Plus II (Ethicon, Inc., Somerville, NJ).
CDH29A 29 mm circular stapler (Ethicon, Inc.).
TaTME, transanal total mesorectal excision.
The patient is positioned on the operating room table in modified lithotomy with convoluted foam used to provide padding and prevent patient movement when placed in extreme Trendelenburg (Fig. 1). The abdominal team typically stands to the patient's right and their monitor is placed directly across on the patient's left. The back table for the abdominal team is usually placed beyond the patient's right leg (Figs. 2 and 3). The energy devices and suction are passed off the patient's right while the laparoscopic camera and insufflation tubing is passed off the patient's left.
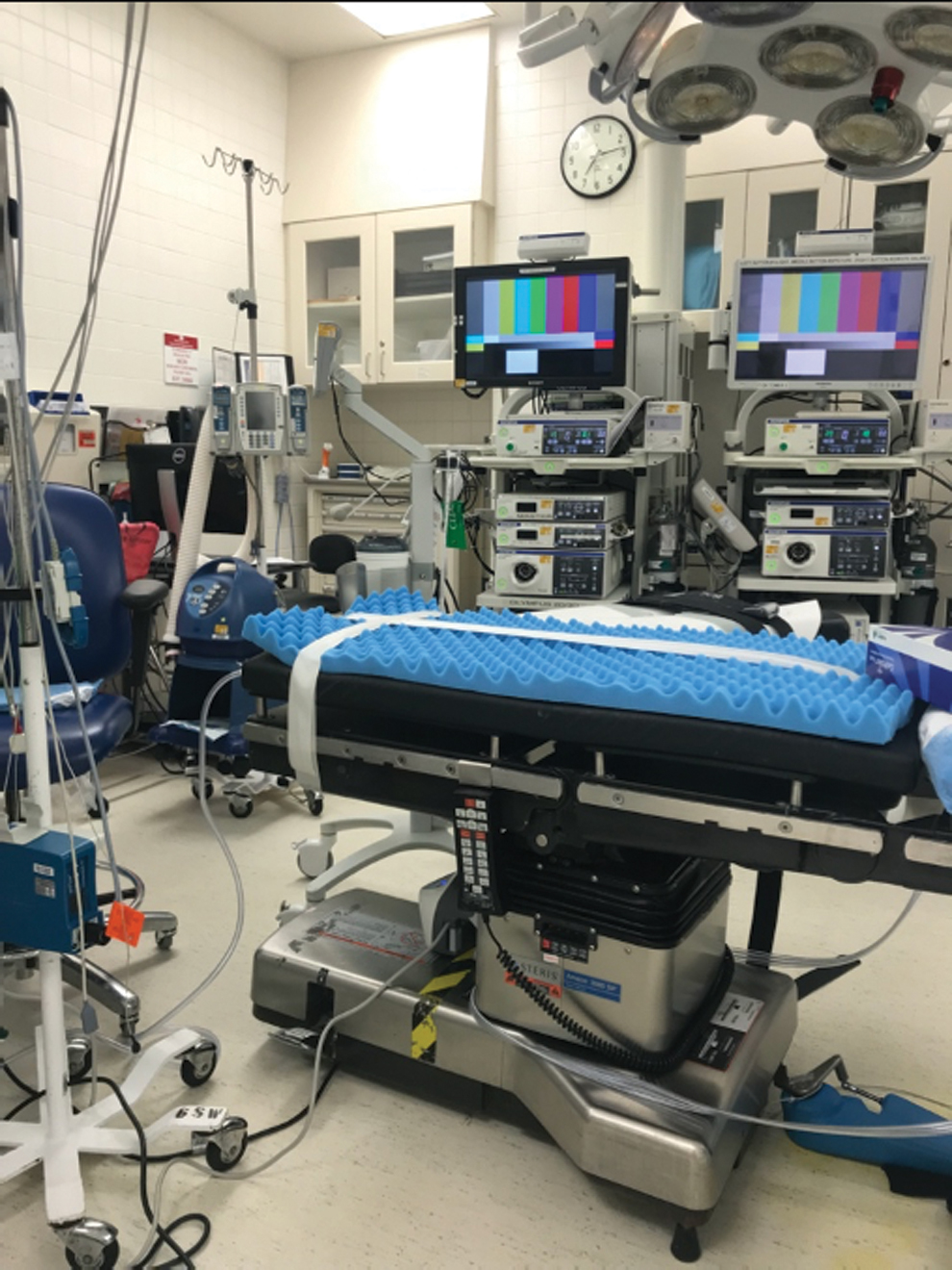
Operating room with convoluted foam used to provide padding and prevent patient movement during positioning. Color images are available online.

Schematic demonstrating surgeon and assistant positioning, video tower and back table set up for abdominal and transanal teams. Color images are available online.
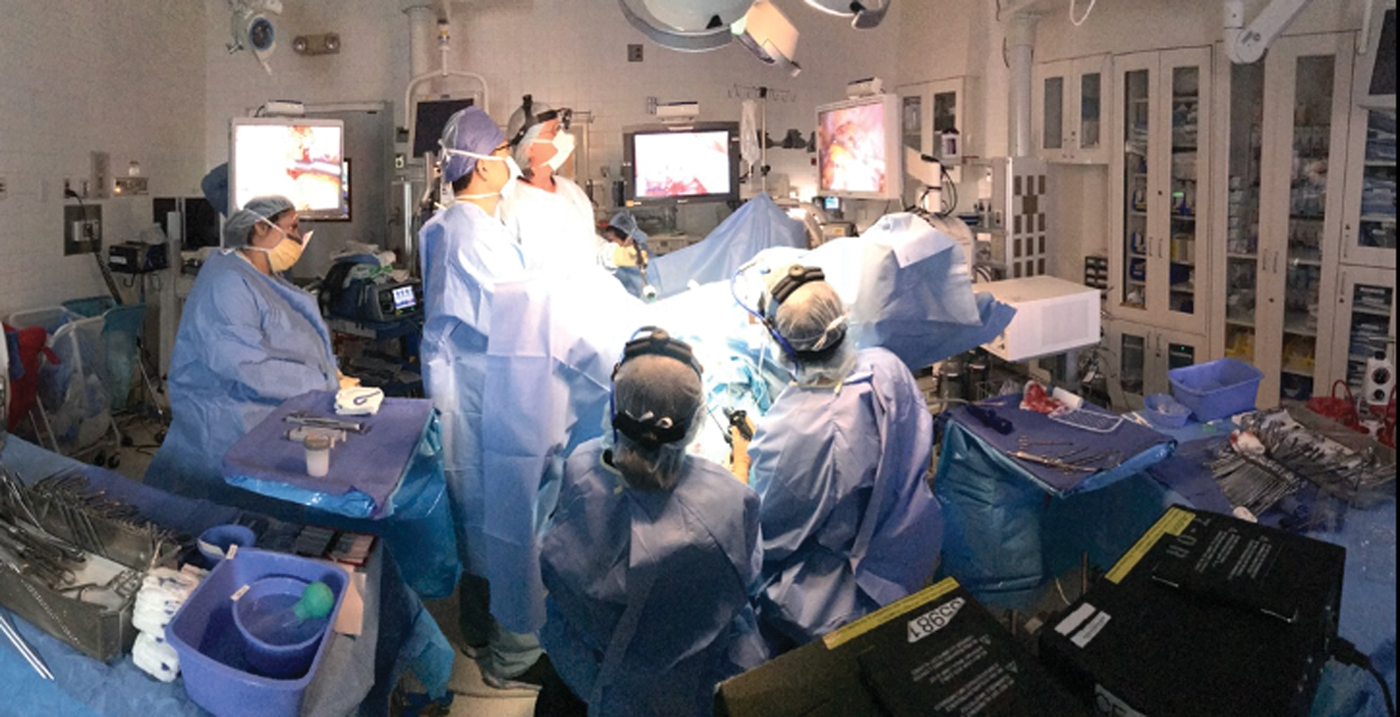
Operating theater set up for simultaneous abdominal and transanal team operation. Color images are available online.
The transanal team is seated between the patient's legs with the back table placed next to the patient's left leg. The Airseal iFS® insufflation management system (Conmed, Inc., Utica, NY) is placed on the patient's left between the abdominal team's laparoscopic tower and the transanal back table (Fig. 3). The electrocautery unit for the transanal equipment is seated on the back table. The video tower for the transanal team is placed to the left of the patient's head and the tower arm is rotated to the midline in a manner that allows the anesthesiologist to access the patient's airway (Fig. 4). For the transanal team, tubing and cords are draped and secured over the patient's left leg. A draped Mayo stand is placed by the patient's left leg on which we can rest the transanal equipment or camera (Fig. 5).

Operating view for the transanal team with video tower positioned by patient's left shoulder with the screen extended, allowing the anesthesiologist access to the patient. Color images are available online.
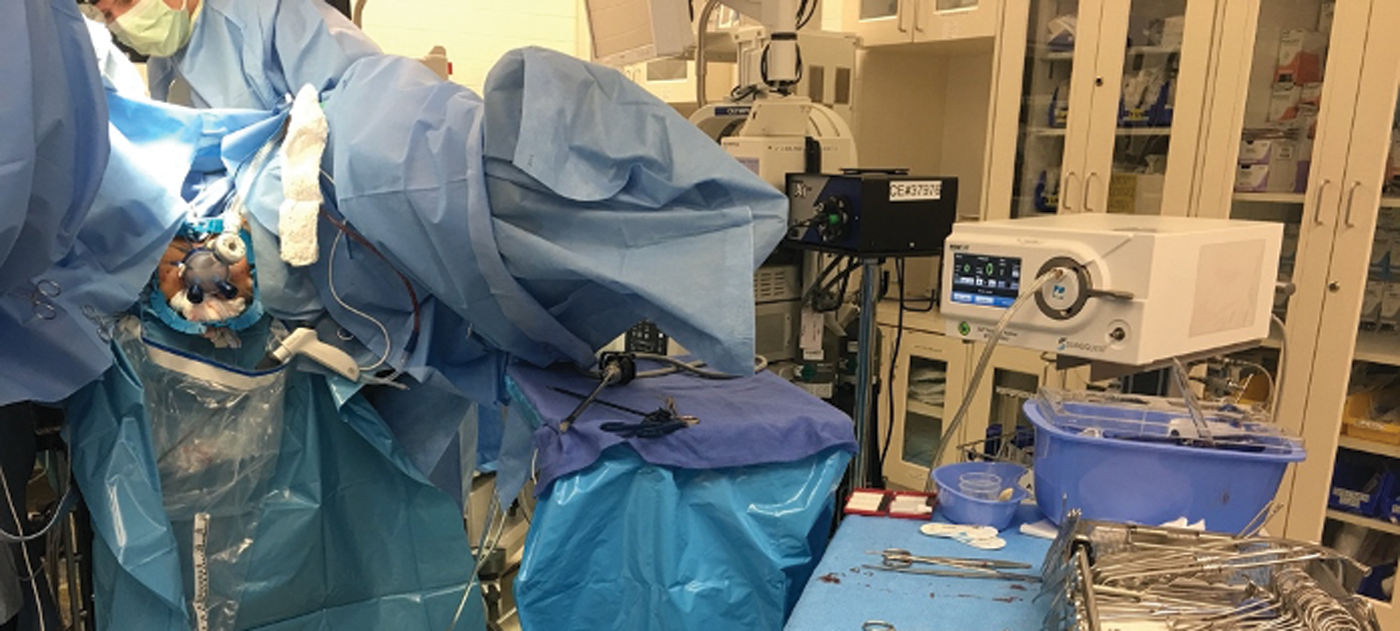
Equipment and instruments for the transanal team passed across patient's left side and draped over the left leg. A sterilely draped Mayo table placed near the patient's left foot to rest the camera and equipment when not in use. Color images are available online.
Abdominal team: laparoscopic colectomy and assessment of pouch reach
In patients undergoing a two-stage IPAA, the abdominal colectomy is performed through a single port access system (GelPOINT® Mini Advanced Access Platform; Applied Medical, Inc., Rancho Santa Margarita, CA) in which we place three 10 mm trocars as a widely spaced triangle through the gel cap with the camera placed at the apex. An additional 5 mm suprapubic port is used to assist the dissection. After completing the colonic mobilization, the mesentery is divided while preserving the ileocolic pedicle. The small bowel and its mesentery are assessed for adequate length and to ascertain pouch reach. Next, the terminal ileum is transected laparoscopically with a stapling device (Echelon Flex™ Powered Plus 60; Ethicon, Inc., Somerville, NJ) before mobilizing any additional mesenteric attachments to the duodenal sweep. During this dissection, because the table position is constantly changing as are the surgeons around the operating table, the transanal dissection cannot occur concurrently during this portion of the case. After the terminal ileum is mobilized and exteriorized through the GelPOINT mini, the abdominal team can create the ileal pouch while the transanal team begins the proctectomy. When the ileal pouch is created, the pouch apex is controlled by placing a betadine-soaked gauze into the pouch and using a 2-0 prolene purse-string suture to close the apex and prevent any spillage. This suture also can be used as a handle during manipulation of the pouch. The pouch is placed back into the abdominal cavity and the gel cap is replaced to reestablish pneumoperitoneum and commence the abdominal laparoscopic dissection.
If the patient has already undergone the first stage of a three-stage approach, the abdominal portion begins with complete mobilization of the end ileostomy and stapled closure of the distal end, taking care to preserve as much terminal ileal length as possible. The ileum is placed in the abdomen and the GelPOINT platform is placed through the previous stoma aperture with three 10 mm trocars widely spaced for triangulation. Mesenteric attachments of the small bowel are mobilized off the duodenal sweep to the pancreatic head and origin of the mesenteric vessels. If the reach of the pouch is limited by the ileocolic pedicle, this vessel can be divided proximally with a Ligasure device while ensuring that vascular arcades and vasa recta supplying the terminal ileal segment are preserved.
Abdominal team: upper rectal mobilization
The upper rectum is mobilized after division of the superior hemorrhoidal artery near the rectal wall taking care to avoid injury to the hypogastric nerves. The presacral space is entered and dissection carried down toward the pelvis in the largely avascular total mesorectal excision (TME) plane between the fascia propria of the mesorectum and presacral fascia. The 5 mm suprapubic port can be helpful in retracting pelvic organs anteriorly.
Transanal team: transanal proctectomy
Before beginning the transanal dissection, the patient is positioned in Trendelenburg position and the Lone Star® retractor (CooperSurgical, Inc., Trumbull, CT) and GelPOINT path access channel are placed. A 2-0 prolene purse-string suture is placed at a uniform distance from the edge of the access channel where the mucosal folds can be seen to converge. The suture is tied down with 20 knots to create a handle which will be used to provide counter traction during the mesorectal dissection. The GelPOINT is capped and pneumorectum of 12 mmHg is achieved using Airseal® insufflation.
If the abdominal team is also working laparoscopically at the time of the mesorectal dissection time, the intra-abdominal insufflation pressures should be reduced to 12 mmHg or lower to avoid pressure mismatch causing the transanal team's field of view to collapse. If the abdominal team is working through an open mini GelPOINT port such that there is no pneumoperitoneum, the transanal insufflation can create a vacuum effect and may cause retraction of the rectum intraabdominally. To counteract this effect, lower transanal Airseal pressures (8 mmHg or less) may be needed to maintain visibility for the transanal team.
Once adequate pneumorectum is achieved, the rectum is scored ∼1 cm distal to the purse-string suture. A full thickness proctotomy is then created at the level of the scored mucosa using the Endopath® Probe Plus hook (Ethicon, Inc.). Doing so generally allows for a 2 cm rim of rectal mucosa between the cut edge of the rectum and the dentate line. It is important to maintain a dissection angle of 90° relative to the plane of the lumen as the proctotomy is carried through the layers of the wall circumferentially. Full thickness proctotomy is confirmed by the visualization of perirectal fat after which the dissection is carried upward toward the peritoneal cavity and abdominal operator. Given the benign pathology, a close rectal dissection has been advocated by some to preserve autonomic nerve function and minimize risk of injury to anterior structures. The anterior plane is typically an easier point to break into the peritoneal cavity, however if the anterior dissection is challenging or the transabdominal dissection is more advanced posteriorly, taking advantage of a posterior entry is certainly appropriate. It is helpful to assess frequently that the transanal dissection is being carried out circumferentially to ensure that a uniformly thin ring of tissue remains before meeting the abdominal dissection. Getting carried away in the dissection of one quadrant can lead to an unintended entry into the peritoneum resulting in spillage of air and fluid from the abdominal dissection and impairment of the transanal view.
Transanal/abdominal team: bringing down the pouch, anastomosis, and final steps
When the abdominal and transanal dissection meet, termed the “rendezvous,” completion of the dissection can be facilitated by either retracting the rectum into the abdominal cavity or by using a retractor to widen the space created at the point of rendezvous. After the rectum has been mobilized completely and dismounted, the transanal GelPOINT cap is removed and the table position is neutralized. We irrigate the pelvis copiously with warm saline allowing it to drain transanally. The specimen is removed transanally by grabbing the distal purse-string suture and removing the access channel. A laparotomy pad is placed through the anus and used as a seal to allow abdominal re-insufflation. The pouch is oriented correctly by the abdominal team and placed at the pelvic brim while retracting the pelvic organs anteriorly. This allows the transanal team to grasp the pouch by passing a ring forceps around the laparotomy pad and to deliver it down to the anus under visualization by using the abdominal team's video monitor.
After determining the desired level of the anastomosis, the residual mucosa can be tailored to pouch reach and a full mucosectomy performed. We perform a hand sewn anastomosis using 2-0 polygalactin sutures on a UR6 needle to the dentate line. If tension on the anastomosis prohibits the extent of a mucosectomy, the pouch can also be anastomosed directly to a rectal cuff of ∼2 cm length. Effacing the anus further by adjusting the Lone star hooks can allow for improved access to the proximal extent of the rectal cuff and facilitate the creation of an anastomosis.
Alternatively, a double purse-string stapled anastomosis can be used during which the anvil of a circular stapling device is placed into the apex of the pouch and a 2-0 polypropylene purse-string is secured around anvil. A red rubber catheter is placed over the spike and the pouch can then be guided into the pelvis in correct orientation using a laparoscopic instrument passed transanally when ready. The distal purse-string can be placed directly around the anus from the transanal approach or using the transanal access system with pneumoperitoneum. It may be helpful to place the purse-string under direct visualization from the abdominal perspective to ensure full-thickness bites are used and that extrarectal tissue is not accidentally incorporated into the anastomosis. The abdominal operator must again confirm that the pouch and ileal mesentery are correctly oriented before closing the distal purse-string suture. The anvil and EEA stapler are mated, and the distal purse-string suture is tied before the stapler is closed. In females, the vagina is manually palpated by the transanal operator to assure it has not been inadvertently included in the anastomosis. The EEA stapler is then fired and removed.
A “reverse” air leak can be performed by maintaining abdominal pneumoperitoneum and checking for leaks through defects in the staple line. Any defects can be oversewn transanally. During this time, the abdominal team is placing drains, performing a laparoscopic tranversus abdominis plane block and creating a diverting loop ileostomy. A full-length 0.25-inch Penrose drain is placed transanally into the pouch.
Perfecting the two-team approach
The most advantageous aspect of the two-team ta-IPAA is the transanal/abdominal rendezvous, which can pose a large challenge for those with limited experience with this technique. Coordination between the two teams is paramount to a successful and efficient dissection. As mobilization of the rectum progresses, it can occlude the transanal view, so during this critical time, it is often helpful to have the abdominal team retract and straighten the rectum, which can afford the transanal team more working space. When the rendezvous has been reached, the two teams must work closely together to dismount the rectum. The abdominal team can initially provide anterior retraction for the transanal team using a fan through the 5 mm suprapubic port. As the dissection continues circumferentially, the rectum can be everted into the peritoneal cavity and the dissection completed by the abdominal team if outside the transanal team's reach or visualization.
We have also found that insufflation pressures during a two-team ta-IPAA are important factors in maintaining adequate visualization for the transanal dissection. During the initial transanal dissection before transecting the rectum, the abdominal insufflation pressure has little effect on the transanal pressures if using a continuous insufflation platform such as the Airseal. However, once the rectum is transected and the mesorectal dissection is underway, maintaining equal abdominal and transanal insufflation pressures offers the most optimal view for the transanal team. Although some authors recommend setting higher transanal pressures, in our experience, this can displace the rectum proximally and flatten the TME plane laterally, making the dissection for the transanal team more challenging while forcing the abdominal team to work at lower insufflation pressure. We find that matching insufflation pressures at 12 mmHg works well for both teams.
Finally, the two teams must be able to compromise. Maximizing available resources to assure a successful and timely surgery is especially important with this approach. For example, the use of a headlight by the transanal team members allows overhead room lights to be kept dim, allowing the abdominal team to continue their portion of the laparoscopic procedure. The abdominal operators may require stepstools to operate comfortably while the operating table is in a raised and Trendelenburg position for the transanal team to begin their dissection. Very importantly, the training and familiarity of the operating room personnel with the procedure and needed equipment is crucial, as is having a dedicated and experienced team of nurses and surgical technicians routinely assigned to these cases. Throughout the case, early communication of needed instruments or equipment is essential as these cases can be quite overwhelming for the operating room staff. Lastly, scheduling the surgery on a day that both surgeons are available for the entire duration of the procedure without any other commitments is essential, particularly during the ta-IPAA learning curve.
Discussion
The transanal platform for a proctectomy offers better visualization and access to the narrow pelvis. This reduces the risk of inadvertent injury to pelvic structures and autonomic nerves, which can have significant implications on functional and sexual outcomes. 24 Conversely, the use of insufflation to establish pneumorectum can cause distortion of planes by showing planes beyond the scope of a transanal dissection resulting in injury to the adjacent autonomic nerves and venous plexuses. 25 Ta-IPAA also has the potential advantage of providing an operative field in a fairly unperturbed plane, where a safe dissection can be accomplished despite chronic inflammatory changes or postsurgical scarring and fibrosis. 26 Most importantly, the transanal approach with a hand-sewn or stapled anastomosis facilitates an easier dissection of the distal rectum, allowing the surgeon to evaluate the mucosa and length of the remnant rectal cuff to determine the precise level of the anastomosis.18,20 Moreover, avoidance of multiple staple firings sometimes required to transect the distal rectum due to the oblique pelvic angle during a laparoscopic proctectomy can result in theoretically decreased rates of anastomotic leaks.21,27 Despite these advantages, the transanal approach has a significant learning curve and is subject to procedure-specific risks, which include premature transection of the rectum leading to bacterial contamination and presacral abscesses 28 or urethral injuries, 29 which can result in significant morbidity.
Although several reports have described the ta-IPAA to be a safe and feasible procedure, the literature regarding outcomes of this relatively novel technique is still surfacing. Currently, there are no prospective randomized data available and few comparative studies evaluate the outcomes of ta-IPAA against a transabdominal approach. The first comparative study by De Buck et al. 20 looking at surgical outcomes, described 97 transanal patients and 119 transabdominal patients. While there was decreased morbidity associated with the ta-IPAA group (P = .003), attributable in part to the close rectal dissection facilitated by the transanal platform, there was no difference in the severity of complications when they were present, and the odds of experiencing an anastomotic leak was comparable for both groups. The conversion rate was significantly lower for the transanal group (23.5% versus 5.2% [P < .001]) as was the postoperative hospital stay (7.34 days versus 9.08 days for the transabdominal approach [P = .001]).
For a procedure in which quality of life and bowel function are integral, there is a dearth of quality data on long-term functional outcomes after ta-IPAA. A recent comparative study by Chandrasinghe et al. 30 of 374 patients included 100 patients undergoing ta-IPAA, and showed significantly better quality of life and energy-level subscores compared with the transabdominal IPAA group; although, overall Cleveland global quality of life scores were comparable, even after adjustment for anastomotic leaks. Thirty-day morbidity rates (33% versus 41%) and anastomotic leak rates (6% versus 13%) were lower for the ta-IPAA group, however, these differences were not found to be statistically significant.
In our own comparative study, which consisted of 36 patients who underwent a transabdominal IPAA and 77 patients ta-IPAA, we found that the overall complication rate (Clavien–Dindo Classification 1 or greater) was significantly higher in the ta-IPAA (57% versus 36% [P = .04]). The incidence of pouch-related complications was much higher in the ta-IPAA group (14% versus 3%) compared with the transabdominal IPAA as was the incidence of CDC grade 2 or higher complications (44% versus 28%). CDC grade 4 complications were observed in two ta-IPAA patients and none in the transabdominal IPAA group. Operating time, opioid narcotic use, and pain scores were similar between the two groups. 31
While multiple reports have shown the ta-IPAA procedure to be technically feasible with acceptable outcomes, comparative data to determine whether it is superior to a minimally invasive transabdominal approach is lacking. In the authors' experience, there appears to be a higher incidence of pouch-related complications with the transanal approach and a significantly increased rate of overall complications. Operative factors, such as a close mesorectal dissection and a single stapled anastomosis have been suggested to reduce complications and risk of inadvertent injury; however, the true impact of these techniques on the outcomes after ta-IPAA remain to be elucidated. The minimally invasive IPAA is an evolving procedure with many technical variations, including more recently, the use of a robotic platform, and large-scale controlled studies are still needed to determine whether one approach truly offers the best functional outcomes for our patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.