
Abstract

W
The authors skillfully presented a descriptive article, elucidating the substantial technical issues for a successful laparoscopic Nissen fundoplication, in patients with refractory gastroesophageal reflux disease (GERD). The authors stressed the importance of creating a short and floppy wrap; adopting the division of the short gastric vessels, starting midway along the greater curvature till the left crus.
We would like to congratulate Schlottmann et al. for sharing such an impressive experience and would like to elaborate on the “Tension-free Nissen Wrap,” from another perspective.
We propose that the well-known natural antireflux mechanisms2,3 might additionally comprise the fundus receptive relaxation and the physically compressible fundus air bubble. Both work—alongside—to absorb the antiperistaltic waves generated within the grinding pyloric antrum. The organoaxial axis of the stomach is typically aligned between the pyloric antrum and the dome of the gastric fundus, which is expanding under the capacious left diaphragmatic copula. Thus, the sided gastroesophageal (GE) junction is, luckily, exempted from receiving such antiperistaltic waves (Fig. 1a).
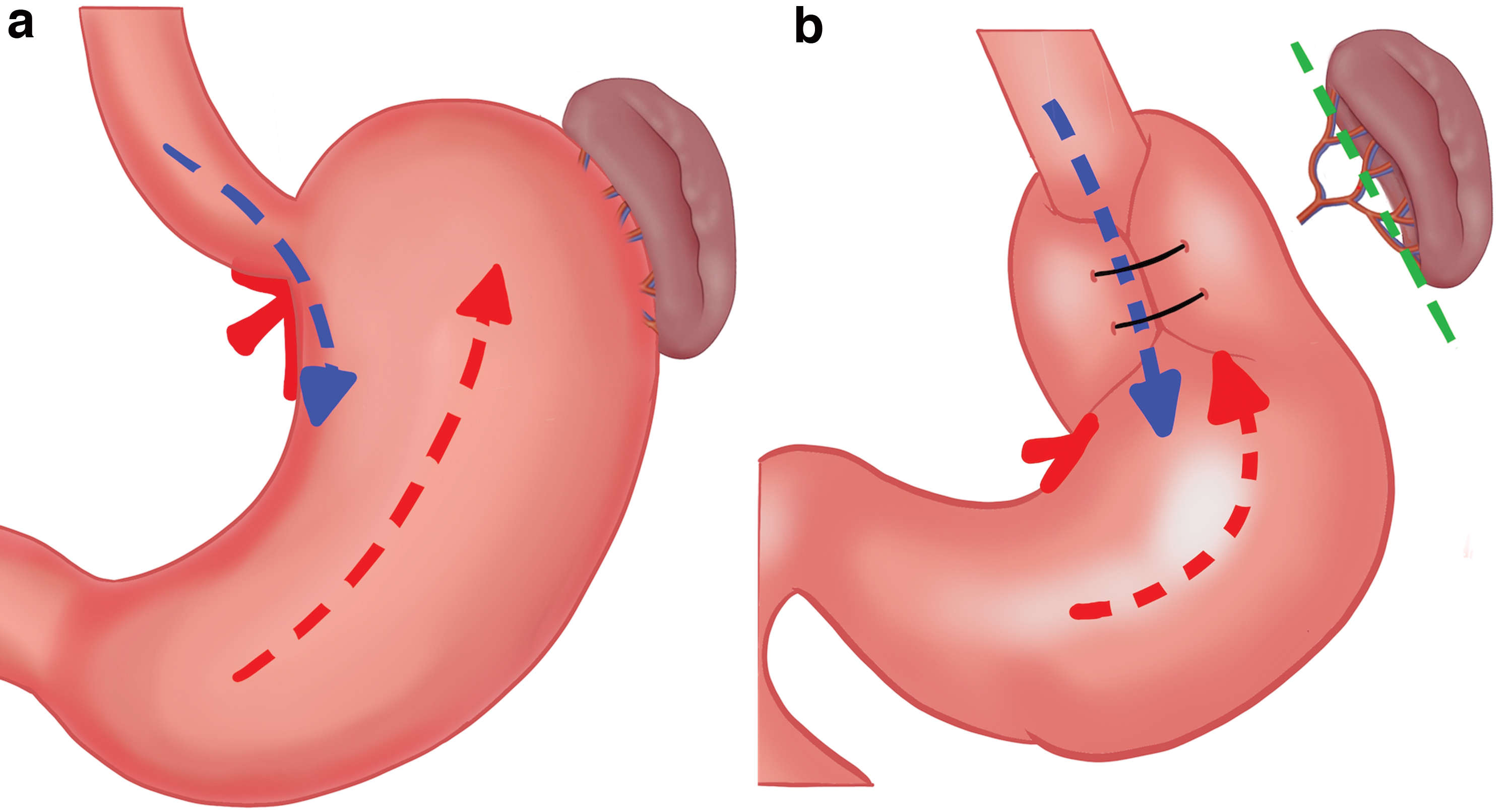
The advocated surgical division of the gastrosplenic ligament to wrap a fully mobilized fundus around the abdominal esophagus would inevitably sacrifice the aforementioned antireflux mechanism and would render the new anatomical alignment vulnerable to pressure/tension, whenever an antiperistaltic wave is propagated. Such straining waves would potentiate wrap slippage, migration, or disruption, according to our proposal (Fig. 1b).
On that account, we believe that the dome of the gastric fundus and the nearby greater curvature are not favorably incorporated into the constitution of any surgical wrap, the alongside anterior ± posterior gastric walls possibly are. The inclination angle between the axis of the lower esophagus and the organoaxial “pyloro-dome” axis of the stomach should never be placed at 0°, whenever a surgical wrap is created.
Considering such a physical concept might preserve the designed wrap from the consequences of a high-pressure zone: that is, the motility-generated dynamic tension, what differs from the rather habitually attributed static tension encountered at suturing of a tight wrap. Herein, we would like to draw the attention of the interested surgeons to such a potentially exciting intellectual concept, that possibly might improve the outcomes of the anti-GERD surgeries.
Compliance with Ethical Standards
Ethical approval
This letter to the editor does not contain any studies with human participants or animals performed by the author. Informed consent: Not applicable.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.