
Abstract
Background:
It is unknown if surgeons are more likely to adopt or abandon robotic techniques given that bariatric procedures are already performed by surgeons with advanced laparoscopic skills.
Methods:
We used a statewide bariatric-specific data registry to evaluate surgeon-specific volumes of robotic bariatric cases between 2010 and 2019. Operative volume, procedure type, and patient characteristics were compared between the highest utilizers of robotic bariatric procedures (adopters) and surgeons who stopped performing robotic cases, despite demonstrating prior use (abandoners).
Results:
A total of 44 surgeons performed 3149 robotic bariatric procedures in Michigan between 2010 and 2019. Robotic utilization peaked in 2019, representing 7.24% of all bariatric cases. We identified 7 surgeons (16%) who performed 95% of the total number of robotic cases (adopters) and 12 surgeons (27%) who stopped performing bariatric cases during the study period (abandoners). Adopters performed a higher proportion of gastric bypass both robotically (22.9% versus 3.1%, P < .001) and laparoscopically (27.5% versus 15.1%, P < .001), when compared with abandoners. Surgeon experience (no. of years in practice), type of practice (teaching versus nonteaching hospital), and patient populations were similar between groups.
Conclusions:
Robotic bariatric utilization increased during the study period. The majority of robotic cases were performed by a small number of surgeons who were more likely to perform more complex cases such as gastric bypass in their own practice. Robotic adoption may be influenced by surgeon-specific preferences based upon procedure-specific volumes and may play a greater role in performing more complex surgical procedures in the future.
Introduction
Once considered high risk bariatric procedures are now among the safest in surgery, with rates of severe adverse events that are similar to those of laparoscopic cholecystectomy. 1 One important factor that has contributed to the success of surgical safety for bariatric procedures has been the rapid adoption of a minimally invasive approach. By 2013, nearly all (97%) of primary bariatric procedures were performed laparoscopically. 2
Robotic surgery has emerged as a new platform for minimally invasive procedures, with potential benefits that include enhanced instrument handling, ergonomics, and three-dimensional video imaging.3–5 However, robotic bariatric procedures have also been associated with an increase in resource utilization and operative time.6,7 Although trends in robotic utilization for general surgery procedures has increased over time it has varied depending on procedure type, ranging from a threefold increase for cholecystectomy to a 44.8-fold increase for hernia repair. 8 To date, it is unclear if there are similar trends in robotic utilization for bariatric procedures and if surgeons are more likely to adopt or abandon the robotic platform over time.
In this study, we used a statewide bariatric-specific data registry to better understand surgeon-specific trends in robotic utilization for bariatric procedures. We sought to characterize the evolution of robotic bariatric procedures over time and identify characteristics among surgeons who adopted or abandoned the platform.
Methods
Data source and study population
This study analyzes data from the Michigan Bariatric Surgery Collaborative (MBSC), a payer-funded statewide consortium that utilizes a bariatric-specific data registry for collaborative quality improvement.9,10 We evaluated annual laparoscopic and robotic bariatric volume, case mix, and patient characteristics among surgeons participating in the MBSC between 2010 and 2019.
Procedures include primary laparoscopic and robotic sleeve gastrectomy (SG), Roux-en-Y gastric bypass, biliopancreatic diversion/duodenal switch (BPD/DS), and revisions (i.e., patients with a prior history of bariatric surgery). Patient characteristics included age, preoperative body mass index (BMI), sex, race, and comorbidities, including diabetes, hypertension, hyperlipidemia, obstructive sleeve apnea, and a history of prior ventral hernia repair. Surgeon characteristics included type of practice (teaching versus nonteaching hospital), gender, and number of years performing bariatric surgery. Surgeons performing cases at a teaching hospital were assisted by surgical trainees (residents or fellows), whereas surgeons performing cases at a nonteaching hospital were assisted by an advance practice provider, nurse practitioner, or surgical scrub.
Study design
To assess trends in robotic bariatric surgery, we first plotted annual overall total bariatric procedure volume as well as percent robotic bariatric utilization during the study period. Next, we categorized annual surgeon volumes for robotic cases as low (<10 cases/year), medium (10–20 cases/year), and high (>20 cases/year) and plotted individual annual surgeon utilization by category. In addition, we assessed the number of surgeons who represented low, medium, and high robotic utilizers during 3-year time intervals and compared their robotic as well as laparoscopic case volumes.
Finally, we compared surgeon practices, procedure volumes, case mix, and patient characteristics between surgeons who adopted robotic bariatric surgery and those who abandoned it. Adopters were characterized as surgeons who were highest robotic utilizers during the most recent time period (2017–2019), whereas abandoners were characterized as surgeons who demonstrated robotic utilization followed by an absence of any robotic cases during the remaining study time period while remaining an active bariatric surgeon within the MBSC.
Statistical analysis
Comparisons of surgeon characteristics, mean annual case volume, case mix, and patient characteristics between adopters and abandoners were performed using t-tests for continuous variables and chi-squared tests for categorical variables. Risk-adjusted rates were calculated using an observed-to-expected adjustment. All statistical analyses were conducted using SAS 9.4. The study was approved by the institutional review board of the University of Michigan for the MBSC and surgeons signed consent before participation.
Results
A total of 44 surgeons performed 3149 robotic bariatric procedures during the study period and SG was the most common procedure (71.6%) (Table 1). Mean age of patients undergoing robotic bariatric surgery was 44.4 years, mean BMI was 48.5 kg/m2, 15.9% were male, and 44.9% were Caucasian. The highest rate of robotic utilization occurred in 2019, when robotic cases represented 7.24% of all bariatric cases (Fig. 1).

Trends in overall robotic utilization for bariatric surgery by year. Color images are available online.
Characteristics of Patients Undergoing Robotic Bariatric Surgery Between 2010 and 2019
BMI, body mass index; BPD/DS, biliopancreatic diversion/duodenal switch; RYGB, Roux-en-Y gastric bypass; SD, standard deviation; SG, sleeve gastrectomy.
Between 2017 and 2019, we identified 7 surgeons (16%) who were high utilizers of robotic bariatrics (adopters). These surgeons performed 95% of the total number of robotic cases during the study period and also performed more robotic bariatric cases than laparoscopic ones (1072 versus 614) during the most recent time period (2017–2019) (Table 2). There were 12 surgeons (27%) who did not perform any robotic cases in 2019 despite prior utilization (abandoners) (Fig. 2). When comparing the type of procedures performed robotically, adopters had higher rates of performing gastric bypass than abandoners (22.9% versus 3.1%, P < .001).
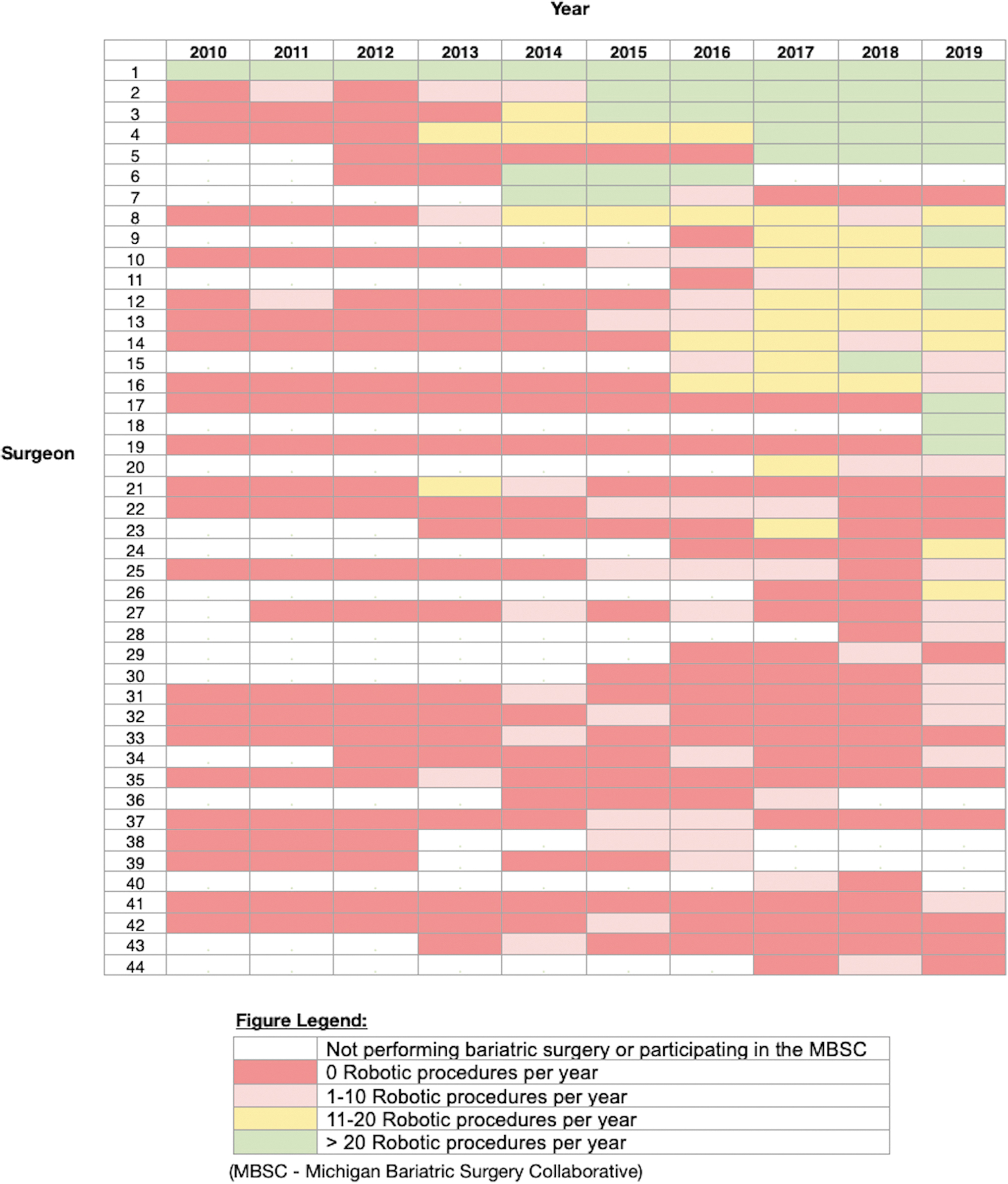
Surgeon-level utilization of robotic bariatric surgery by year. Color images are available online.
Comparison of Robotic and Laparoscopic Bariatric Operative Volume, Among Low, Medium, and High Utilizers of Robotic Bariatric Surgery
Likewise, when assessing the type of procedures performed laparoscopically by surgeons in the study, adopters of the robotic platform had higher rates of performing laparoscopic gastric bypass (27.5% versus 15.1%, P < .001) (Table 3).
Comparison of Operative Case Volume, Procedure Type, Practice Setting, and Patient Characteristics Between Adopters and Abandoners of Robotic Bariatric Surgery
BMI, body mass index; BPD/DS, biliopancreatic diversion/duodenal switch; RYGB, Roux-en-Y gastric bypass; SD, standard deviation; SG, sleeve gastrectomy.
Mean annual case volume for both laparoscopic and robotic bariatric cases was lower among robotic adopters than abandoners (73 versus 182); however, it did not meet statistical significance. Also, there were no significant differences between mean number of years performing bariatric surgery (14 versus 11 years) and type of practice (teaching versus nonteaching hospital) between adopters and abandoners.
Likewise, patient age, BMI, sex, and history of preoperative surgery (i.e., hernia repair) were either clinically similar or not statistically significant between groups, regardless if they were undergoing robotic or laparoscopic cases.
Discussion
In this unique study evaluating surgeon-specific practices over nearly a decade, we found considerable variation in robotic utilization, with the majority of robotic bariatric cases performed by a small group of surgeons. These surgeons performed more robotic bariatric cases than laparoscopic ones during the most recent time period, indicating near full adoption of the robotic platform. Despite an overall increase in robotic utilization over time, we also found that more than a quarter of the surgeons stopped performing robotic bariatric cases after demonstrating prior utilization, indicating that they had abandoned robotics for bariatric cases.
In addition, our data demonstrate that compared with abandoners, robotic adopters are more likely to perform gastric bypass in their own practice, regardless of operative approach (laparoscopic versus robotic). Although specific reasons for adopting or abandoning robotic bariatric surgery remain unclear, our data indicate that adopters may be more likely to benefit from the robotic platform given that they are more likely to perform procedures that require advanced technical skill.
Trends in the adoption of robotic surgery for common surgical procedures in Michigan had been previously evaluated by Sheetz et al., which demonstrated an 8.4-fold increase between 2012 and 2018. 8 They noted that the trend was associated with a decrease in laparoscopic surgery (53.2%–51.3%) and those hospitals that launched robotic surgery programs had a broad and immediate increase in robotic utilization. Although their study included common general surgical procedures (i.e., hernia repair, colectomy, cholecystectomy, and reflux surgery), it did not include bariatric procedures and was focused on hospital-level adoption rates, as opposed to surgeon-specific trends.
Our study expands on this work in several ways. First it demonstrates a similar trend in bariatric surgery, with an overall increase in robotic utilization over time. However, by assessing surgeon-specific practices versus hospital-level data, we found that the majority of cases were performed by a small number of high-volume robotic users who subsequently performed more robotic bariatric cases than laparoscopic cases within their own practice. In addition, despite the increase in robotic bariatric volume over time, we found that more than a quarter of surgeons had abandoned the robotic platform during the same time period.
Surgeon-specific reasons for adopting robotic surgery may include enhanced ergonomics and visualization, which may decrease workload and can increase the longevity of their operative career. 4 In addition, the prospects of machine learning, virtual/augmented reality, and integration of artificial intelligence may have incentivized some surgeons to adopt robotics so they may overcome the learning curve earlier in their career, despite being proficient in laparoscopy.11,12 Our data demonstrate that robotic adopters perform more gastric bypass in their practice, as it represented a higher proportion of both their robotic and laparoscopic case volumes than abandoners.
When compared with SG, gastric bypass requires more technical skill, including laparoscopic suturing, to perform gastrointestinal anastomoses. As such, robotic adopters appear to both recognize and utilize the augmented features the robotic platform has to offer to perform more complex tasks. Meanwhile, robotic abandoners may have realized they derive less benefit if their practice primarily involves SG procedures. Moreover, given that abandoners had a higher overall bariatric volume, they may have also questioned the impact on their overall operative efficiency. When compared with their own laparoscopic practice, robotic abandoners may have noted an increase in resource utilization and operative time with the robotic approach, which has been supported by prior studies.6,7,13,14
This is further supported by the variation in procedure-specific adoption of robotic cases for other general surgery procedures as noted by Sheetz et al., who found that minimal adoption for more simple procedures such as cholecystectomy (annual slope 0.4%) and a higher adoption rate for more complex procedures such as reflux surgery (annual slope 2.8%) and proctectomy (annual slope 4.0%). Another hypothesis is that surgeons who were more likely to perform open gastric bypass in the past were more inclined to perform the operation robotically as an alternative to a laparoscopic approach. This is also supported when comparing trends for open and robotic general surgery procedures (nonbariatric) during a similar time period. 8
Decreased operative efficiency may be a reason why some surgeons have abandoned robotic bariatric procedures. For gastric bypass, Sharma et al. noted longer median operative times (136 versus 107 minutes, P < .001) with comparable overall complication rates (10.6% versus 10.7%, P = .80) when compared with propensity matched laparoscopic cases. 7 Similarly, Celio et al. reported longer operative times for robotic cases (150.2 versus 111.8 minutes, P < .001), but also noted higher rates of complication (15.8% versus 12.5%, P = .002) and reoperation (8.8% versus 5.3%, P < .001). 13 As with gastric bypass, prior studies evaluating robotic SG also demonstrated longer operative times but comparable complication rates, when compared with a laparoscopic approach. 15
Although these studies provide a patient-level analysis of operative efficiency and outcomes, they do not consider surgeon-specific differences in experience, volume, or practice setting (i.e., teaching versus nonteaching hospital), which may influence their own decision to abandon or adopt the robotic platform. When evaluating large multicentered data registries, adverse events for robotic cases have decreased over time (5.2% versus 3.7% from 2015 to 2017, P < .05). 16 However, given the pattern of adoption among a small number of high volume surgeons as demonstrated in our study, the decrease in complication rates may be a reflection of improved outcomes among surgeons who have fully adopted robotics in their practice, as opposed to those who abandoned the robotic platform after performing a small number of cases.
Our study has several limitations. First, the data only include procedures performed in a single state, which may not reflect the same practice patterns across the United States or internationally. Moreover, we chose not to expose geographic regional practices to protect the anonymity of each program from commercial interests or marketing campaigns. However, the use of a longitudinal prospectively collected bariatric-specific data registry provides a unique glimpse of surgeon-specific evolution of robotic bariatric surgery across a diverse group of practice types (i.e., teaching versus nonteaching hospital), which is difficult to replicate.
In addition, although the MBSC data registry captures bariatric cases performed since 2006, it is unknown if surgeons began performing robotic cases, including nonbariatric procedures (i.e., hernia, biliary, and foregut) before that.
Performing nonbariatric robotic cases may have helped some surgeons overcome an initial learning curve that contributed to adoption of robotics for bariatric cases. In addition, surgeons who practice at hospitals that utilize the robotic platform commonly may have employed specialized teams to improve operative efficiency. Finally, the study was underpowered to assess gender differences in rates of adopting or abandoning a particular technology. This can be valuable data in the future, however, since adoption rates may be associated technologies that take gender differences into account. As such, surgeon-level studies that assess reasons for adopting or abandoning disruptive technologies can provide additional value when considering implementation strategies.
Conclusion
In this longitudinal statewide assessment of surgeon-specific utilization of robotic bariatric surgery, we found an overall increase in operative volume for robotic bariatric cases that were being performed by a small number of high-volume robotic surgeons who performed more robotic cases than laparoscopic. These surgeons were more likely to perform complex procedures such as gastric bypass in their own practice. As such, robotic adoption may be influenced by surgeon-specific preferences based on procedure-specific volumes and may play a greater role in performing more complex procedures in the future.
Footnotes
Ethical Approval Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
O.A.V. reports grants from Blue Cross Blue Shield of Michigan, during the conduct of the study. A.H.C.-N. reports grants from Blue Cross Blue Shield of Michigan and Blue Care Network, during the conduct of the study. M.H.W. and A.M.C. have nothing to disclose. A.A.G. reports grants from AHRQ, PCORI, and Blue Cross Blue Shield of Michigan, outside the submitted study. D.A.T. reports grants from Medtronic, NIDDK, and AHRQ, during the conduct of the study.
Funding Information
No funding source.