
Abstract
Introduction:
The use of staples to perform intestinal anastomosis in children has gained popularity in the past years. The aim of this study is to evaluate the outcomes of pediatric patients who underwent intestinal anastomosis with a 5-mm staple in a tertiary health care center.
Material and Methods:
From April 2017 to November 2019, the records of all pediatric patients who underwent intestinal anastomosis with a 5-mm staple were retrospectively revised. The reconstruction technique was functional end-to-end anastomosis.
Results:
A total of 12 intestinal anastomoses were evaluated. Mean age at surgery was 120 days. Small bowel anastomosis was the most frequently performed procedure (eight cases). Stapling difficulties were found in 3 patients. The anastomosis could not be performed with the 5-mm endostapler in one of these patients. The median follow-up was 26 months (interquartile range 20–40 months). Postoperative complications included one bowel obstruction that was surgically treated.
Conclusions:
Mechanical suturing with 5-mm staple is a safe alternative technique to perform intestinal anastomosis in neonates and infants. The use of this staple has proven to be safe and feasible in pediatric patients. It is necessary to select patients carefully according to their bowel characteristics.
Introduction
Stapled anastomosis is increasingly used in pediatric surgery. Since Powell 1 described the use of intestinal staples in neonates, several studies have reported successful results in these patients. However, the size of the staples can be a limitation. Recently, the development of 5-mm endostaplers have rekindled interest in this technique, enabling its use in smaller patients. However, reports in the literature are limited.
The aim of our study is to evaluate our experience using 5-mm endostaplers to perform bowel anastomosis in neonates and infants. We also want to highlight the technical difficulties that we have experienced using this mechanical device, to increase the safety of the procedure.
Materials and Methods
From April 2017 to July 2019, all charts of the pediatric patients who underwent stapled intestinal anastomosis were retrospectively reviewed. The inclusion criterion was the use of a 5-mm endostapler to perform at least one intestinal anastomosis. Patients with an estimated bowel diameter of <5 mm were excluded from the study. Demographics, preoperative, intraoperative, and postoperative data were collected from patient's medical records.
Intestinal anastomoses were performed with a linear endostapler Microcutter 5/80 Dextera® (Aesculap). The diameter of the cartridges is 5.3 mm and its tip can be straight or curved. We used straight cartridges in all cases, as they were more appropriate for intestinal surgery. According to the closed staple height, there are two types of cartridges: 1.05 mm (white) and 1.43 mm (blue).
A functional end-to-end (FEE) anastomosis was performed in all cases. Care should be taken to avoid twisting the bowel. The two jaws of the endostapler are inserted into each limb (Fig. 1A). The antimesenteric bowel walls must be appropriately compressed before firing the staple device. This is described as a safety method in mechanical suturing, as the compression allows the adequate distribution of the liquid phase of the tissue, improving the adjustment of the staple to the bowel wall.2,3 The remaining enterostomy is closed with a further firing of the linear staple (Fig. 1B).
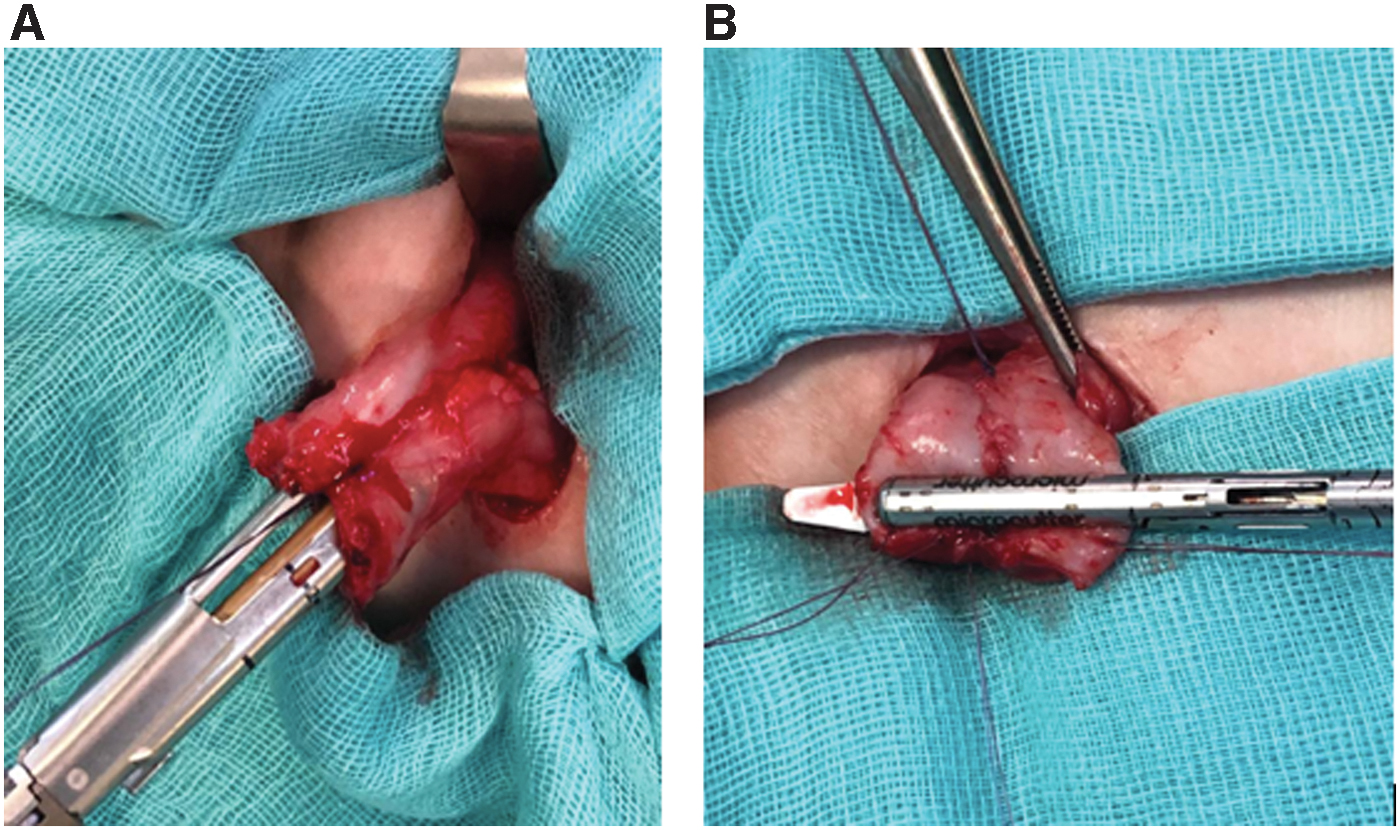
Functional end-to-end anastomosis.
Results
A total of 11 patients were included in this study. There were 6 boys (54.5%) and 5 girls (45.5%) with a median age of 120 days (range 1–375 days) at the time of surgery. Median patient weight was 3.2 kg (range 1.9–10 kg). Surgical diagnoses are summarized in Table 1. A total of 12 FEE anastomoses were performed. Small bowel anastomosis was the most common enteroenterostomy (eight cases), followed by colocolonic anastomosis (three cases). After resection of the ileocecal valve, an ileocolic anastomosis was performed in 1 patient.
Patient Data
Intraoperative stapling difficulties were found in 3 patients (27.3%). In one of these cases, related to a colostomy closure in a 224-day-old child, the anastomosis could not be completed with the 5-mm staple, using a 12-mm one instead. In the remaining two cases, the intestinal union could finally be performed with the 5-mm staple.
The median postsurgical follow-up time was 26 months (range 20–40 months) Postoperative complications included a case of bowel obstruction that was surgically treated. The patient had a history of bowel tapering due to an intestinal atresia. There were no dehiscences or anastomotic stenosis.
Discussion
Intestinal anastomoses are common procedures in neonatal surgery. However, they are often related to technical difficulties. Several factors have demonstrated to affect the difficulty of neonatal intestinal anastomosis: complex suture technique, discordant bowel caliber between segments, urgent procedures, and rarity of these pathologies. Therefore, it is necessary to optimize the safety of neonatal surgical care. Mechanical suture devices have gained popularity over the past years. They have demonstrated to be a safe alternative to traditional technique in small children.
Powell reported the first use of intestinal mechanical sutures in neonates in 1995. They included 7 patients with a median age of 79 days at the time of surgery who underwent stapled anastomosis without complications. 1 Subsequently, Simmons et al. have published 18 cases 4 and Mitchell et al. have reported 64 cases. 5 Several comparisons between stapling and hand suture in neonates and infants have been reported in the past years. Stapled anastomosis has demonstrated shorter operative time. No differences were found in postoperative complications.6–8 The first studies describe the use of 12-mm staples. However, these staples are not suitable for small children. In addition, some authors observed anastomotic dehiscence due to the use of 2.5-mm staples. Because of its size, these staples are not appropriate for thin bowel wall. 7 New 5-mm staples are more accurate for small children,9,10 and they have been tested in animal models. 11
In our study, there were intraoperative complications during colostomy closure in older infants. These failures can be explained by an excessive thickness of the tissue with respect to the closed staple height. Other authors have reported similar complications related to an incomplete staple closure. 12 Therefore, it is mandatory to select the patients who will benefit from a 5-mm endostapler, keeping in mind three important aspects: the characteristics of the staple, the differences between intestinal segments and the age of the patient. Nowadays, we think that the main indication for the 5-mm staple in neonatal intestinal surgery is small bowel anastomosis in children younger than 6 months.
It is important to consider other technical issues to ensure the safety of the intestinal anastomosis. FFE anastomosis is a relatively easy technique to be performed. In addition, this technique may be employed to address discordant bowel caliber between intestinal segments. 13 However, FEE anastomosis can also lead to complications. For example, volvulus has been described in patients with a too wide anastomosis.14,15
Technically, the weakest point of FEE anastomosis is the joint between longitudinal and transverse intestinal sections. Overlapped staples cannot grasp the tissue accurately. 13 In our experience, although we did not have any case of leakage, we have observed staple malfunction during the remaining enterostomy closure in one of the cases. Therefore, we think that it could be beneficial to modify the position of the staples, as it is described in the literature. 13 The lesser intraoperative failures presented, the safer the procedure will be.
We keep all of these considerations in mind as we continue to evolve our skills. The standard hand technique in small children is well documented. However, there are not enough studies regarding mechanical suture in that population. In addition, it is necessary to develop 5-mm staples specifically designed for neonatal open surgery. Then, prospective comparisons between hand and mechanical sutures must be made to determine the optimal surgical technique. Studies of a prospective nature will allow selecting patients who may profit most from this procedure.
In conclusion, mechanical suture with 5-mm staple is a safe alternative technique to perform intestinal anastomosis in neonates and infants. According to our initial experience, an adequate patient selection based on their intestinal characteristics improves safety and efficacy of the procedure. It is important to develop suitable staples for use in pediatric patients, especially in neonates and infants.
Ethical Approval
All procedures performed in our study were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all legal guardians of the children included in the study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding received.