
Abstract
Background:
Laparoscopic local resection of the stomach for gastric submucosal tumors (SMTs) is widely accepted by surgeons. For SMTs located near the esophagogastric junction (EGJ), simple laparoscopic wedge resection is rarely performed owing to concerns of causing cardia deformities or stenosis. Single-incision laparoscopic intragastric surgery (sLIGS) has been used to treat SMTs located near the EGJ in carefully selected cases.
Methods:
We modified sLIGS using a subxiphoid incision. Thirteen consecutive patients with intraluminal or intramural growth type gastric SMTs located near the EGJ underwent sLIGS at our institution from July 2018 to April 2020.
Results:
Thirteen operations were successfully performed using sLIGS, including eight full-thickness resections and five submucosal resections. There were no conversions to an open procedure and all tumors were confirmed to have negative margins on pathology. The mean operation time was 100 ± 10 minutes (range, 85–160 minutes). The mean blood loss was 50 ± 10 mL (range, 50–100 mL). The mean length of postoperative hospital stay was 7 ± 1.5 days (6–10 days). One patient was found to have oozing of blood confirmed by gastroscopy postoperatively and recovered after stopping antiplatelet therapy. Ten cases were gastrointestinal stromal tumor (GIST), two cases were leiomyoma, and one case was neuroendocrine neoplasm. Of the 10 GISTs, 9 were classified as low risk; 1 showed medium risk and the patient received adjuvant imatinib therapy. There were no tumor recurrences during a mean follow-up of 14 ± 4 months (range, 5–25 months).
Conclusions:
This modified sLIGS for the treatment of the gastric SMTs located near the EGJ is simple and safe. This can be used as an alternative treatment for gastric SMTs near the EGJ.
Introduction
Laparoscopic local resection of the stomach for gastric submucosal tumors (SMTs) is widely accepted by surgeons.1–3 Laparoscopic wedge resection with endoscopic linear staples is an ideal option for SMTs in favorable sites in the stomach. 4 However, for SMTs located at unfavorable sites, especially near the esophagogastric junction (EGJ), simple laparoscopic wedge resection is rarely performed owing to concerns of causing cardia deformities or stenosis. Several techniques has been used by surgical researchers, including laparoscopic intragastric surgery (LIGS) and laparoscopy/endoscopy cooperative surgery.5–10 Taniguchi et al. first reported applying LIGS to treat gastric SMTs. 11 A series of cases were reported and the outcomes were excellent. A limitation of LIGS is the escapement of the surgical port from the gastric wall. Single-incision laparoscopic intragastric surgery (sLIGS) was modified from LIGS to avoid this limitation and to improve the cosmetic outcomes. 12 Nevertheless, sLIGS still needs to be performed in conjunction with endoscopy. Furthermore, resection of the tumor involves use of staples; and therefore, careful patient selection is critical. We made some modifications of sLIGS and reported 13 patients of gastric SMTs using this technique.
Patients and Methods
From July 2018 to April 2020, 13 consecutive patients who were diagnosed with gastric SMTs located near the EGJ underwent sLIGS at the Department of Gastrointestinal Surgery, the Li Huili Affiliated Hospital, Ningbo University. All patients underwent gastroscopy and abdominal computed tomography (CT) preoperatively to determine the tumor location, size, and type of development. Endoscopic ultrasound was performed regularly to determine the involvement of adjacent organs or vessels.
This study was approved by the Institutional Review Board of the Li Huili Affiliated Hospital, Ningbo University (no. KYSB2020YJ064-01), and was performed in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants. The following data were collected retrospectively: gender, age, tumor size, tumor location and size, operation time, intraoperative blood loss (estimated blood loss), length of hospital stay, postoperative complications, pathological diagnosis, and follow-up.
Operative technique
The patient was placed in a supine position under general anesthesia. A 3-cm longitudinal incision was made on the upper abdomen. After exploration of abdomen, a gastrotomy incision was made on the anterior wall of the distal stomach under direct vision. A wound protector device (Disposable Trocar [Single Port]; KangJi Medical, Hangzhou, Zhejiang, China) was placed into the gastric lumen and we secured both the abdominal and gastric walls. Wound sealers (Disposable Trocar [Single Port, Gel type], KangJi Medical) were placed in three ports (12-, 10-, and 5-mm) through the gel cover and assembled on the wound protector subsequently. The stomach was insufflated with carbon dioxide gas at 12 mmHg, and then, a 30-° laparoscope was inserted via the 10-mm port above the other two ports. The lesion was clearly visualized and the resection line was marked using electrocautery if the margin was close to the EJG.
Depending on the growth type of the lesion, we performed two types of resection. Type A is a full-thickness resection if the SMT presents as an exophytic growth near the EGJ. All layers of the gastric wall around the tumor are divided using a harmonic scalpel (Harmonic Ace; Ethicon Endo-Surgery, Cincinnati, OH) and the tumor is resected en bloc. The tumor is brought out through the single port. The defect of the gastric wall is closed by hand-sewing using barbed suture (Stratafix Spiral PGA-PCL, SXMD1B405, Tensile Strength Size 3-0; Ethicon, Inc.). The wound on the anterior gastric wall is closed using continuous running suture with 3-0 absorbable thread under direct vision. Type B is submucosal resection when the SMT is an extremely endophytic growth. The mucosa around the tumor was cut and the submucosa is dissected to identify the pseudocapsule of the tumor by harmonic scalpel. The muscle layer is cut to ensure the integrity of the pseudocapsule. The tumor and the defect of the gastric wall are also treated as in Type A (Fig. 1).
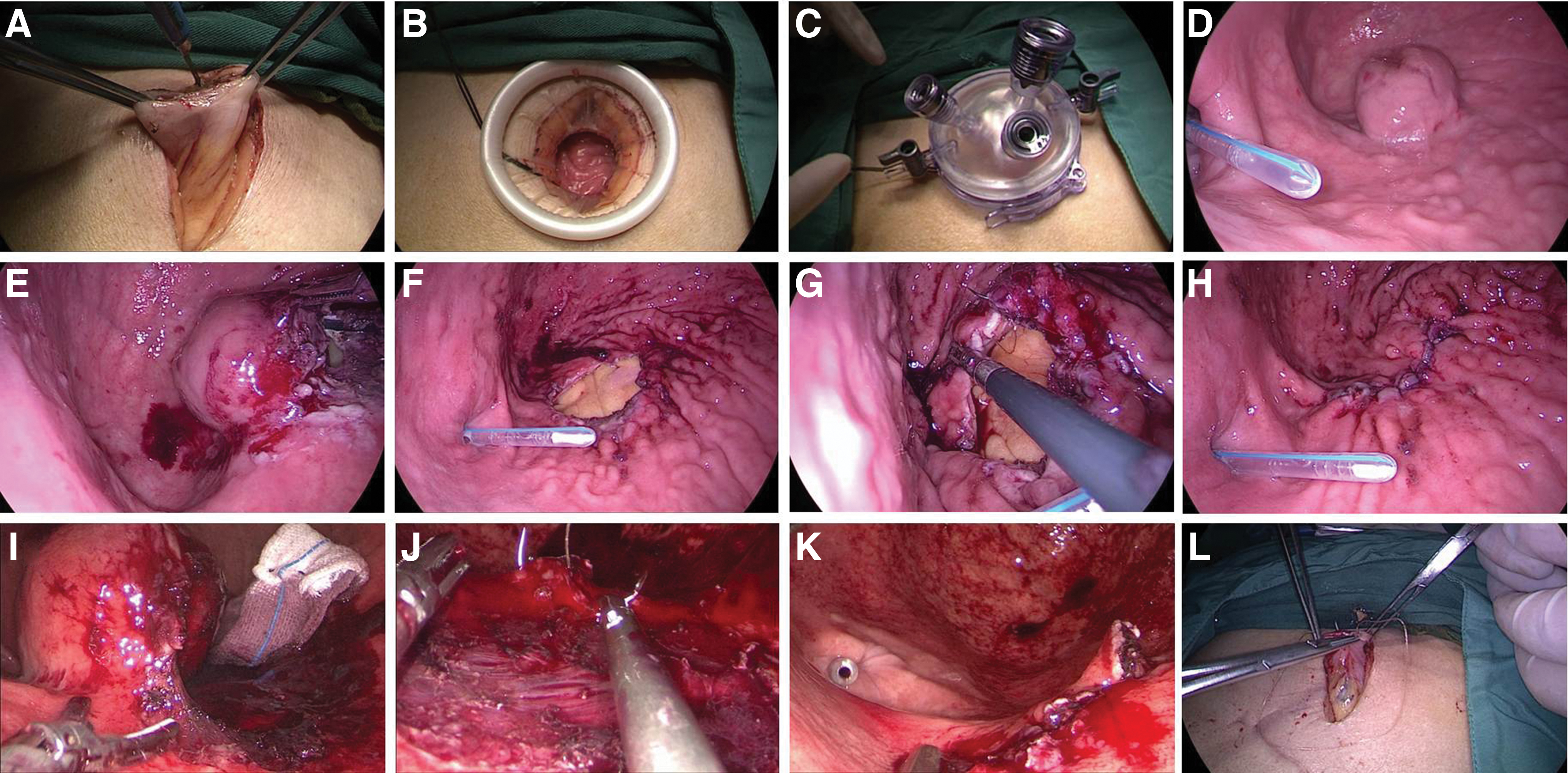
sLIGS for gastric SMTs located near the EGJ.
Results
Patient characteristics and outcomes are shown in Table 1. Thirteen patients (7 males and 6 females) with SMTs near the EGJ underwent sLIGS. Seven tumors were located at the gastric fundus, three at the lesser curvature, and three at the posterior wall, with a mean size of 3.4 ± 0.2 cm (range, 2.0–5.0 cm).
Clinical Characteristics and Outcomes of 13 Patients Undergoing Single-Incision Laparoscopic Intragastric Surgery
Operation type: A full-thickness resection.
B submucosal resection.
EGJ, esophagogastric junction; GIST, gastrointestinal stromal tumor; LOS, length of stay; NR, no recurrence.
All 13 operations were successfully performed using sLIGS with 8 full-thickness resections and 5 submucosal resections. There were no conversions to open procedure and all tumors were resected en bloc without any ruptures. The mean operation time was 118 ± 6.8 minutes (range, 85–160 minutes). The mean blood loss was 61.5 ± 7.0 mL (range, 30–100 mL). One patient presented melena 6 days postoperatively after 3 days of taking aspirin and clopidogrel. Gastroscopy confirmed oozing of blood along the barbed suture line. The bleeding resolved after stopping antiplatelet therapy. The mean length of postoperative hospital stay was 7.6 ± 0.4 days (6–10 days).
All tumors were confirmed to have negative margins on pathology. Ten cases were gastrointestinal stromal tumor (GIST), two were leiomyoma, and one was a neuroendocrine neoplasm. Of the 10 GISTs, 9 classified as low risk, 1 showed medium risk according to the modified Fletcher classification and the patient received adjuvant imatinib therapy. All patients were followed up with abdominal CT scan every 3 months and gastroscopy every 6 months. There were no tumor recurrences during mean follow-up of 12.5 ± 1.8 months (range, 5–26 months).
Discussion
With the popularization of gastroscopy and the development of endoscopic ultrasound technology in recent years, the detection rate of gastric SMTs has improved significantly. Of these tumors, GISTs are the most common. 13 Because SMTs rarely have distant metastasis, local resection may be used. With the development of surgical technology in recent years, a number of clinical studies have shown that, compared with traditional laparotomy, laparoscopic and endoscopic surgeries produce less postoperative pain, faster recovery, and shorter hospital stays.3,6,14–16 For these reasons, laparoscopic and endoscopic surgeries have been widely used in the treatment of SMTs.
For SMTs with a tumor diameter less than 2 cm, endoscopic submucosal resection (ESD) has been widely recognized because of the low risk of recurrence. Nevertheless, it remains unclear whether ESD is applicable to SMTs with a diameter of 2 to 5 cm, especially for those located around the EGJ, where the treatment methods depend on the location, the size, and the growth pattern of the tumor. For SMTs in unfavorable sites, especially extraluminal stomach tumors, conventional laparoscopic wedge resection is the standard treatment. However, for lesion positions close to the EGJ or around the pylorus, laparoscopic gastric wedge resection is not a particularly ideal procedure. Excessive gastric wall incisions often lead to stricture or deformation of the cardia, resulting in requirement for total or proximal gastrectomy. A number of laparoscopic or laparoscopic+endoscopic cooperative surgeries have been proposed by many scholars for treating SMTs near the EGJ.6,9,16–18
LIGS is one of these minimally invasive surgeries. LIGS was first proposed by Ohashito to treat early gastric cancer. 19 Since then, a substantial number of reports have highlighted the method of SMT treatment, especially for SMTs near the EJG, where good curative effects have been achieved.7,8,11,16 This operation provides sufficient surgical vision field, which can maximally facilitate preservation of the normal gastric wall tissue around the tumor.
Unlike conventional laparoscopic gastric wedge resection, this treatment avoids deforming the cardia. However, most LIGSs use Endo-GIA staplers to treat tumor tissues, and this may possibly damage the organs behind the stomach wall. Furthermore, transgastric trocar placement is a major challenge, because the trocar is prone to escape from the gastric cavity, or special balloon-type ports may be required. 5 In addition, the handling of specimens is a problem; smaller specimens can be taken out through the mouth or from the trocar incision, while larger specimens are difficult to remove through the mouth.
Katsuyama et al. modified LIGS to sLIGS, in which gastrostomy was performed on the anterior gastric wall through the umbilical incision. 12 Since the laparoscopic single-port channel was established, the operation then can be completed through the gastric cavity. This procedure has the advantages of LIGS while preventing the trocar from escaping the gastric cavity (port escapement). Nevertheless, this procedure still uses the Endo-GIA stapler to remove the tumor tissue, and therefore, for tumors presented as exophytic growth or located close to the EJG it may be difficult to handle.
We use an ultrasonic scalpel under direct vision in the gastric cavity to perform full resection along the edge of the tumor in cases of exophytic growth. Doing so maximally preserves the normal gastric wall tissue, maintaining the function of the stomach, and avoiding deformation or stenosis of the cardia. In addition, we use hand-sewing under direct vision to close the wound. This is not as difficult as imagined, especially using barbed suture, even in the context of single-port laparoscopy. We use a subxiphoid incision, certainly does not provide a good cosmetic appearance as an umbilical incision. Nevertheless, the incision is located directly on the anterior wall of the stomach, which makes it easier to perform gastrostomy and does not require the aid of a gastroscope. Although the procedure has been reported for gastroscope guidance, 12 it is possible to perform gastrostomy through a single port at the umbilicus; nevertheless, there are certain difficulties in various situations, especially when there are adhesions around the stomach, making it difficult to directly pull the stomach wall closer to the umbilicus. The incision under the xiphoid process can reduce associated complications. Furthermore, it is easier to use the original incision if conversion is needed, although no conversions were required in our series.
Compared with previous procedures, the advantage of our procedure is that it does not require the involvement of an endoscopist nor any special equipment. In our operations, we did not use any special laparoscopic instruments except for laparoscopic single-port devices. This device can freely adjust the position of the trocar with the gel characteristics to maintain a relatively soft operative feeling while fixing the trocar. However, if there is no special laparoscopic single-port device, we sometimes also use a homemade method for which a conventional incision protector and gloves are required, and the outcome is just as good (Fig. 2). Patient selection is important and the indications for sLIGS are similar to those of the original LIGS procedure. Because our modified sLIGS allows full-thickness resection, the most appropriate cases are intraluminal or intramural growth-type SMTs near the EGJ, with the tumor not larger than 5 cm. For extraluminal tumors, surgical methods such as laparoscopy/endoscopy cooperative surgery may be more appropriate. Although large tumors removed using laparoscopic resection have been reported at several institutions,20,21 we still perform laparotomy for gastric SMTs large than 5 cm because of concerns regarding tumor rupture.

A homemade laparoscopic single-port device.
The limitation of this operation is the possibility of perigastric vascular injury, especially for lesions located on the posterior wall of the gastric body close to the splenic hilum. Because the resection starts in the stomach cavity, the blood vessels outside the stomach wall are difficult to identify. For lesions that are close to large blood vessels before surgery, abdominal CT three-dimensional reconstruction before surgery ought to be carried out. During the operation, we lift the stomach wall when the ultrasound knife cuts it. Therefore, it is relatively safe to use an ultrasonic knife cautery for small blood vessels close to the stomach wall, including ones located in the stomach end, the short gastric vessels, and other blood vessels. Although this surgical incision fully penetrates through the gastric wall, there is almost no gastric content leakage in the operation due to preoperative gastrointestinal preparation and intraoperative indwelling nasogastric tube. Furthermore, the surgical suture under direct vision is more accurate. In addition to maintaining the indwelling gastric tube after surgery, no postoperative intra-abdominal drainage tube is placed. Postoperative preventive anti-infective therapy is required. Using this stringent procedure, there were cases of abdominal infection after the operation. In consideration of the gas leakage in the gastric cavity, some studies have mentioned that bowel clamp forceps should be used to clamp the jejunum. In our series, there were no issues with gas leakage, regardless of the use of jejunum clamping. This could be related to the current usage of the high performance insufflator. However, once the stomach wall is cut and the connection to the abdominal cavity is established, high-performance insufflator is required, or the stomach cavity will collapse, resulting in poor surgical vision.
Overall, this modified sLIGS to treat gastric SMTs located near the EGJ is simple and safe, and no skilled endoscopists are required. This can be used as an alternative treatment for gastric SMTs near the EGJ.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Li Huili Affiliated Hospital, Ningbo University. Written informed consent was obtained from all participants. The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
M.Z. and W.Y. conceived and designed the study; M.Z. and X.C. wrote the article; C.L. and Y.W. acquired and analyzed the data; W.Y. proofread and revised the article; all authors approved the version to be published.
Acknowledgment
We appreciate Professor Yi Yuan for the operations performed on patients.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.