
Abstract
Background:
Minimally invasive repair of pectus excavatum (MIRPE) technique is the current most used surgical method for pectus excavatum (PE) correction. To avoid MIRPE-required invasion of the mediastinum or pleural cavity, we developed taulinoplasty approach as an alternative option for the reduction of the sunken chest.
Materials and Methods:
This is a single-center unblind nonrandomized prospective pilot study, involving 26 MIRPE and 23 taulinoplasty patients. The primary safety endpoint was the presence of surgical complications, and the primary efficacy endpoint was Haller index measured postoperatively in taulinoplasty patients. Secondary endpoints were intensive care unit (ICU) and hospital length of stay (LOS), duration of surgical procedure, and postoperative pain management. Chi-square, Mann–Whitney, or Student “t” tests were used for comparison as appropriate.
Results:
There were no difference in median age (14.5 and 14 years), Haller index (4.63 and 4.17), or comorbidities. MIRPE and taulinoplasty procedures showed no difference regarding major or minor surgical complications. The efficacy endpoint of taulinoplasty was measured 5.5 (1.5–12) months after the procedure, exhibiting a significant reduction in the Haller index [4.17 (3.7–4.7) at baseline and 3.7 (2.9–4.1) postoperatively, P = .03]. Taulinoplasty required less surgical time (60.4 ± 15.5 versus 70.7 ± 15.9 minutes, P < .01); shorter ICU and hospital LOS (P < .01, respectively); and required fewer days of peridural, intravenous, and oral analgesia (P < .01, respectively).
Conclusions:
In this pilot study, taulinoplasty technique was as safe as the MIRPE approach and effective for the correction of PE, reducing surgical time, ICU and hospital LOS, and achieving better postoperative pain control.
Introduction
Pectus excavatum (PE) is the most common congenital chest wall deformity, with an incidence of 1 in 400 births.1,2 PE is most often noted in the first year of life (86%), and the remaining cases present some time before or during the early teenage years. 3 The etiology remains unclear, but it appears to be polygenetic, following autosomal dominant, autosomal recessive, X-linked, or sporadic patterns of inheritance.4,5
Symptomatic patients with associated pulmonary or cardiac abnormalities, and a Haller index of 3.25 or greater, are candidates for surgical repair. 6 Until the end of the past century, the Ravitch procedure and its modified forms remained the standard surgical treatment of PE, involving a subperichondral resection of the affected costosternal joints with stabilization using an internal osteosynthesis of the fractures produced for the reduction of the defect.3,7,8
In 1998, Nuss published his noninvasive technique for lifting the sunken chest. 9 Nuss's technique achieved the reduction of sternal collapse by rotating the pectus bar, based on the physical principle of levers that states that any weight can be lifted by a fulcrum and a long enough lever arm. With only a few exceptions, open surgical procedures were replaced by the Nuss minimally invasive repair of pectus excavatum (MIRPE) technique, due to its excellent outcomes and the effectiveness of the bloodless reduction of the sternum achieved by levering from inside the chest.6,10–15
Based on the same principles as the Nuss technique, we hypothesized that sternal lifting might also be possible through external traction to avoid invading the mediastinum or pleural cavity. The taulinoplasty approach (“Pectus Up”) comprises a plate for extrathoracic implantation and a traction system specifically designed to support and distribute the necessary loads over the defect and counteract the reduction of the sunken chest. 16 The results of a small case-series study have been reported elsewhere 16 and have shown the main advantage of the procedure to be its ability to avoid the invasion of the mediastinum and pleural cavity and thus lower the morbidity rates reported with the intrathoracic approach.6,12,15
Encouraged by these results, we developed this pilot study to evaluate the efficacy and safety of taulinoplasty compared with the MIRPE technique in a single-center cohort study.
Materials and Methods
Design and study population
This prospective unblind nonrandomized pilot clinical study was conducted at a single teaching hospital (Hospital Universitarí Parc Taulí, Barcelona, Spain). Written informed consent was obtained. The database and the study protocol were approved by the Parc Taulí Health Corporation's drug research ethics committee and the institutional review board and by the Catalan Hospital Union Foundation's clinical research ethics committee. The guidelines applied in this study complied with current Spanish regulations (Biomedical Research Law 14/2007). From 2012 to 2017, 49 adolescents and children with severe PE (Haller index >3.4) underwent surgical correction. Twenty-six patients underwent the MIRPE repair procedure and 23 patients the taulinoplasty technique.
Demographics, clinical characteristics, and surgical outcome were retrieved from medical records. Cardiac involvement was measured with transthoracic echocardiography, and pulmonary function tests were performed with standardized spirometry. We used the same analgesic protocol for both groups.
Surgical technique
The taulinoplasty technique has been described in detail elsewhere. 16 In brief, a minimally invasive incision is first made for the placement of the plate in the middle of the sunken chest. Then, a hole is created in the sternum and the plate placed in the desired position, ensuring that the central hole coincides with the hole made in the bone. The elevating system is added, the sternum is raised to the ideal position, and the plate fixed to the sternum with the screws. Finally, the elevator is extracted and the skin incision closed.
Endpoints and statistical analysis
The primary safety endpoint was the presence of surgical complications, and the primary efficacy endpoint was Haller index measured postoperatively. Secondary endpoints were intensive care unit (ICU) and hospital length of stay (LOS), duration of surgical procedure, and postoperative pain management.
The descriptive analysis is shown as means and standard deviations for normal quantitative variables and medians and interquartile ranges for non-normal quantitative variables. Characteristics of patients were compared according to the surgical technique used (MIRPE or taulinoplasty) using chi-square, Mann–Whitney, or Student “t”-tests as appropriate. All the tests were two tailed with a level of statistical significance of 0.05. We used R 3.6.2 (R Core Team, Vienna, Austria) for all statistical analyses and graphics.
Results
Table 1 displays the baseline characteristics of the 26 patients undergoing MIRPE and the 23 patients undergoing taulinoplasty. There were no significant differences in median age [14.5 (12.2–16) and 14 (11.5–15.5) years P = .36] or Haller index [4.63 (4–6.1) and 4.17 (3.7–4.7) P = .30]. Male gender predominated in both groups (MIRPE 65.4% and taulinoplasty 82.6%). There were no differences in previous clinical characteristics such as chest pain, asthenia, pulmonary infections, and cardiac or pulmonary function test results.
Patients' Baseline Characteristics
MIRPE, minimally invasive repair of pectus excavatum.
Primary endpoints
There were no differences between MIRPE and taulinoplasty procedures regarding major or minor surgical complications. The rates of infections, pneumothorax, dehiscence, seroma, and pulmonary edema were also similar (Table 2).
Safety Endpoints
MIRPE, minimally invasive repair of pectus excavatum.
Cardiac taponade, cardiac perforation, major bleeding, death.
The efficacy endpoint of taulinoplasty was measured 5.5 (1.5–12) months after the procedure, presenting a significant reduction in the Haller index [4.17 (3.7–4.7) at baseline and 3.7 (2.9–4.1) postoperatively, P = .03], measured by chest X-ray (Fig. 1).
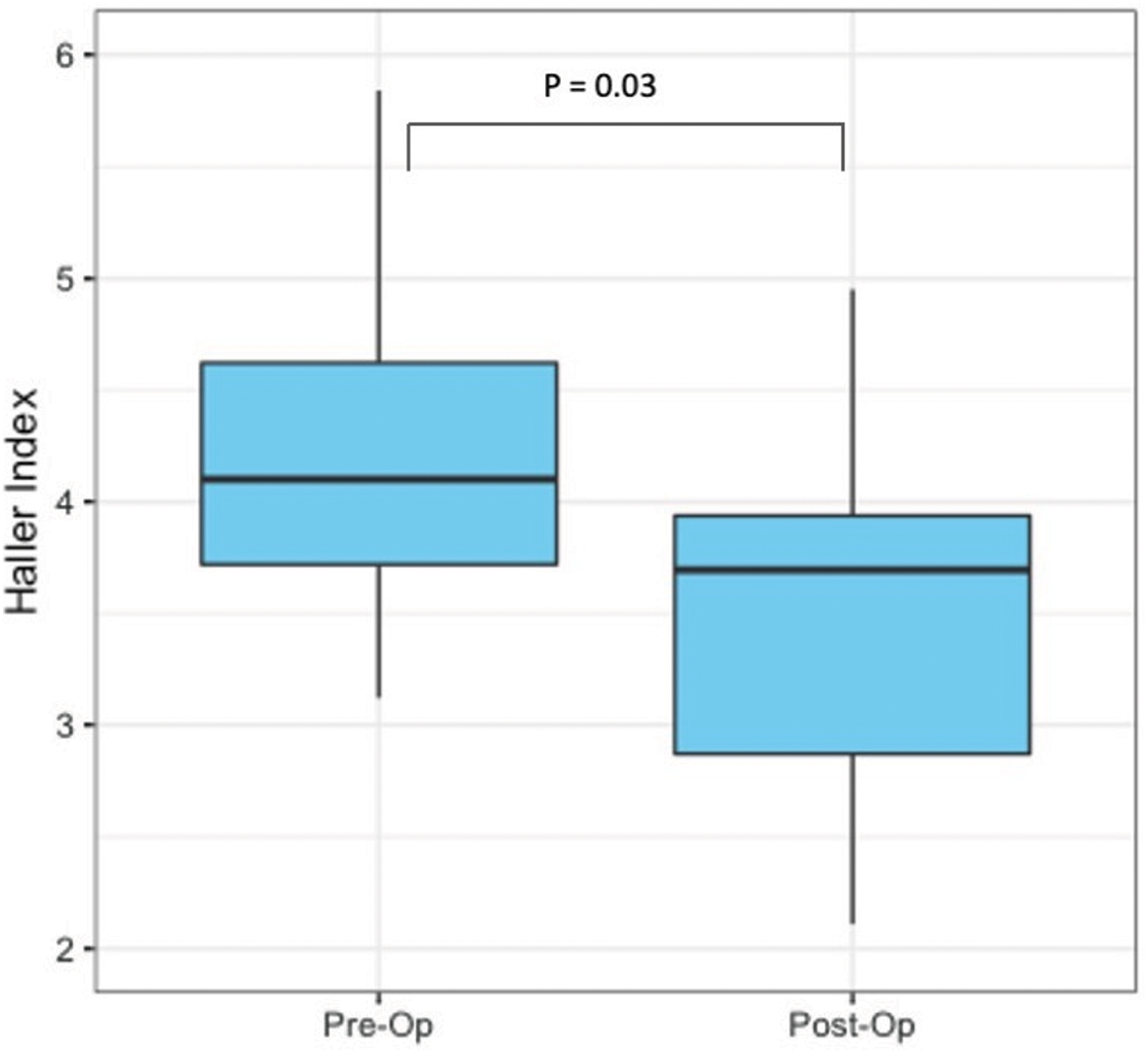
Haller index before and after taulinoplasty (Pectus Up) procedure. Color images are available online.
Secondary endpoints
Compared with the patients treated with the MIRPE technique, patients treated with taulinoplasty required less surgical time (60.4 ± 15.5 versus 70.7 ± 15.9 minutes, P < .01) and had shorter ICU (3.2 ± 1.1 versus 1.4 ± 0.9 days, P < .01) and hospital LOS (8 ± 2.4 versus 5.5 ± 1.2 days, P < .01) (Fig. 2).
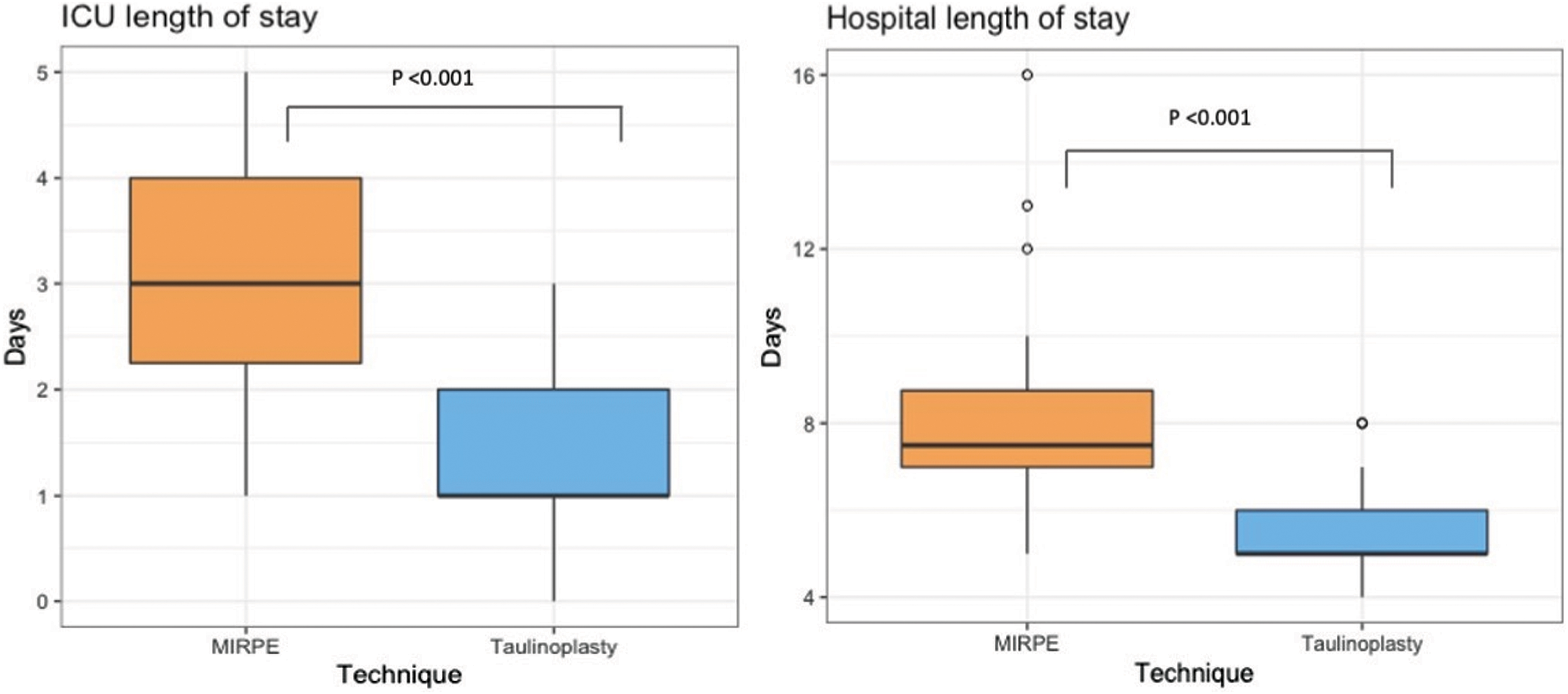
Intensive care unit and hospital length of stay according to surgical technique. Color images are available online.
Regarding postoperative pain management, patients with taulinoplasty required fewer days of peridural analgesia (3.1 ± 1.2 versus 1.5 ± 0.8 days, P < .01), intravenous analgesia (5 ± 2.2 versus 3.5 ± 1.2 days, P < .01), and oral analgesia (27.5 ± 11.5 versus 13.6 ± 11.2 days, P < .01) (Fig. 3).

Surgical time and postoperative pain management according to surgical technique. Color images are available online.
Discussion
In this single-center pilot study, taulinoplasty proved its safety and effectiveness as an extrathoracic surgical procedure for PE. Moreover, it also showed significant reductions in ICU stay and hospital LOS compared with the MIRPE technique, as well as better postoperative pain management.
Reducing the risk of injury to intrathoracic vital organs17,18 by avoiding the invasion of the mediastinum and the pleural cavity is the main advantage of taulinoplasty in the repair of PE. Several studies have reported a low early complication rate with MIRPE, with a trend toward further reductions over time.6,12–15 For instance, the rates of infection, pneumothorax requiring drainage, and hemothorax were <2%.14,15 The most common major complication of MIRPE is bar displacement, with a prevalence ranging according to surgical team from 3.5%, 12 7.3%, 19 8.6% 6 to 19%. 13 Nonetheless, it should be pointed out that major adverse outcomes such as cardiac, perforation, major vessel injury, and lung, liver, or diaphragmatic injury are underreported with an overall incidence ranging from 2% to 20%. 20
As taulinoplasty does not require bars, it avoids this frequent complication. Two recent meta-analyses showed that the MIRPE and Ravitch procedures do not differ in terms of effective correction of PE.21,22 Nevertheless, pediatric patients treated with MIRPE experienced shorter operation time and less blood loss, with similarly low complication rates and hospital LOS.
Our complication rate was in line with those previously reported.21–23 In addition, in our study, there were no major surgical complications in either group and the rate of minor complications was similar. Hosie et al.'s 12 study was the only large series study to report surgical time with MIRPE, recording a mean of 76 (40–345) minutes. Our surgical times with MIRPE were comparable with those reported by Hosie et al., and longer than those required for taulinoplasty. Taulinoplasty also reduced ICU and hospital LOS, indicating clear advantages with regard to resource utilization and patient safety. Considering that most surgical procedures reduce their complication rates and improve outcomes as surgeons gain experience with the technique, 15 we expect the taulinoplasty surgical time and LOS to improve further in the near future.
PE repair is associated with substantial pain. 12 High rates of epidural use of intravenous opioid for 2–4 days have been reported.24,25 As postoperative pain has implications for hospital LOS, activity, and quality of life, pain management is a pivotal component of postoperative care. Papic et al. 26 reported that MIRPE was more painful than the Ravitch technique, and required 25% more opioid use per day and double the intravenous dose of diazepam per kilogram. Moreover, in a large series case report, 6 peridural analgesia was used for 2–4 days, with an incidence of Horner's syndrome of 75% and one case of Reynaud's syndrome. Our results showed that patients with taulinoplasty received less peridural and intravenous analgesia, and that after switching to oral analgesia, the treatment duration was half that required in MIRPE patients.
These findings are in accordance with previous reports of pain management of MIRPE, 26 and suggest that taulinoplasty is better tolerated and less painful. In addition, the cost of the metal prosthesis is more or less the same in both techniques.
Our study has several limitations. The first is its single-center unblinded design. Therefore, some bias of this type of design could be argued. Nevertheless, the promising results encourage us to continue our analysis and validate our findings in other cohorts and with different surgical teams. Second, we did not include highly asymmetrical or long funnel (Grand Canyon) chested patients, and so this population should not be considered candidates for taulinoplasty until further studies have confirmed its suitability. Third, the median follow-up period was only 5.5 months, as this pilot study was designed to evaluate short-term outcomes; future studies should be carried out to establish the long-term efficacy of the procedure.
Finally, we used chest X-ray for the postoperative measurement of the Haller index in taulinoplasty patients instead of computed tomography. This decision complied with the standard practices at our center that seek to avoid unnecessary exposure to radiation in children and adolescents.
Conclusions
In this pilot study, taulinoplasty proved to be an effective and safe technique for the correction of PE, reducing operating time and hospital LOS and ICU stay, and achieving better postoperative pain control. Further studies are warranted to validate these findings and to study long-term outcomes.
Data Availability
The data sets generated and analyzed in this study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
The Comitè d'Ètica d'Investigació amb medicaments at the Corporació Sanitària Parc Taulí and the clinical research ethics committee of Fundació Unió Catalana d'Hospitals approved the database and the study protocol. The guidelines followed in this study complied with the applicable Spanish regulations (Biomedical Research Law 14/2007).
Footnotes
Authors' Contributions
Study concept and design were taken care of B.N.G.; data acquisition was done by B.N.G., N.A.G., and C.E.M.; data processing and interpretation were carried out by J.A.-E., B.N.G., and N.A.G.; statistical analysis and figure preparation were carried out by J.A.-E. and B.N.G.; drafting of the article was done by J.A.-E., B.N.G., N.A.G., C.E.M., J.R.G., and P.J.-A.; revision of the article for important intellectual content was taken care of B.N.G., N.A.G., and C.E.M.; study supervision was by N.A.G.; data access and responsibility were taken care of B.N.G.; N.A.G. had full access to all the data in the study and takes full responsibility for their integrity and the accuracy of the data analysis; and all authors reviewed the article.
Acknowledgment
We gratefully thank Laura Neuberger et al. for editing the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.