
Abstract
Background:
Securing of the appendix stump is one of the key steps in performing laparoscopic appendicectomy (LA). This can be achieved by a variety of methods including endoloops, stapler, and clips. An alternative technique, previously described by authors, is the use of Johan forceps as a knot pusher, to deploy an extracorporeal Roeder knot at the base of appendix. We aimed to evaluate the safety and cost-effectiveness of our technique.
Patients and Methods:
A single surgeon's, prospective cohort, and multicenter study was undertaken at three different hospitals in the United Kingdom. We collected data of all patients, who underwent LA by this technique between 2014 and 2019. Demographics, operative findings, postoperative complications and readmissions were recorded and analyzed.
Results:
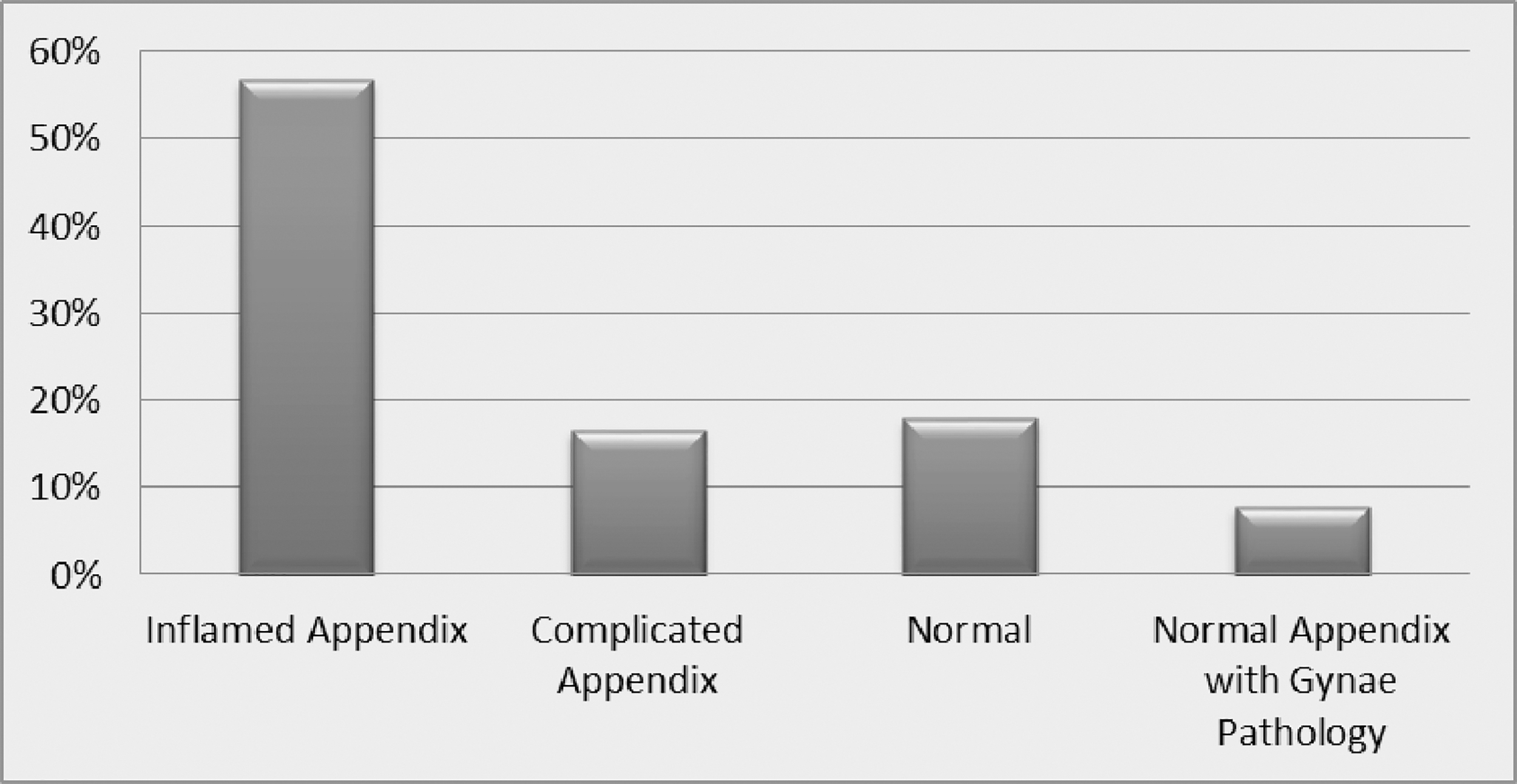
In total, 227 appendicectomies were performed. Median age was 24 years (interquartile range [IQR]: 16–58) with 58% male preponderance. Operative findings were 57% (n = 130) acutely inflammatory appendicitis, 16.74% (n = 38) were complicated appendicitis (perforated, gangrenous). Rest of the operative findings were macroscopically normal appendix (with no other pathology in 18.06% (n = 41), and macroscopically normal appendix but with gynecological pathologies in 7.9% (n = 18). Postoperatively, there were no cases to report complication of blow out stumps neither clinically nor radiologically. Surgical site infections rate has been 3.5% (n = 8). One patient had small intra-abdominal abscess (0.4%), treated by IV antibiotics. Mean hospital stay was 1.89 days (standard deviation [SD] 1–5 days). Thirty days readmissions rate was 4.8%. None of the complications or readmissions was related to the surgical technique. There were no deaths recorded in this series. Cost of handmade endoloop was $0.69.
Conclusion:
Use of Johan forceps as knot pusher for extracorporeal Roeder knot is a safe, feasible, cost-effective, and easily reproducible technique for carrying out LA.
Introduction
Appendicitis is the commonest cause of acute abdomen requiring appendectomy.1,2 Laparoscopic appendicectomy (LA) has become the “standard” in many centers. 3 This is due to less analgesics requirements, better cosmesis, and lower wound infection rates as compared with open procedure and with the additional benefit to perform simultaneous diagnostic laparoscopy, in cases of diagnostic uncertainty. 4 However, the high cost associated with laparoscopic procedures, including LA, is frequently debated. Routine use of expensive equipment is one of the prime reasons behind the high expenditure. 5 Hence, without compromising patient's safety, a careful selection of instruments will help reduce procedure cost. The high cost associated, in particular, with LA is mainly influenced by the choice of technique used to manage appendix stump (AS). 6
Securing of the AS is one of the key steps in performing LA. This can be achieved by a variety of methods including endostapler, 7 preformed endoloops, titanium clips, polymer clips, intracorporeal suturing, and hemolocks. 6 An alternative method is designing of an extracorporeal knot, deployed then by a knot pusher. 8 Majority of such extracorporeal knot techniques, described for appendectomy, involves negotiating the suture end around the base of appendix, later exteriorizing of that suture end through port to fashion an extracorporeal knot, so as to be then deployed by the knot pusher.9,10 However, there have been reports of tissue trauma due to complex repetitive actions, inadvertent excessive tension on the suture, and distraction from the operative field too. 11
We described an inexpensive option of fashioning a standard extracorporeal endoloop, using Roeder's knot, and then its safe deployment onto the base of the appendix by using universally available laparoscopic Johan forceps as a knot pusher through a 5 mm port. We have already reported this technique. 12
We undertook a prospective cohort study, at three district general hospitals in the United Kingdom, with the aim to assess the safety, feasibility, and cost-effectiveness of our technique of LA.
Patients and Methods
Study design and data collection
Single surgeon's prospective cohort study was conducted at Barnsley Hospital NHS Foundation Trust (BHFT), Dewsbury & District Hospital, and The Royal Oldham Hospital from March 2014 till June, 2019. All patients who underwent LA by the described technique during this period were included. Cases converted to open procedure were excluded. Data including demographics, operative findings, postoperative stay, postoperative complications, and readmissions were recorded on a structured proforma.
Statistical methods
Data were analyzed using SPSS version 20.0 (IBM corporation, Armonk). Descriptive statistics were computed. Categorical variables were represented by proportions, whereas mean and standard deviation (SD) were represented by continuous variables having normal distribution. Median and interquartile range (IQR) were calculated for continuous variables having skewed distribution. Patients with missing or incomplete records were censored in the analysis.
Our primary outcome measures were safety and cost-effectiveness of Johan as knot pusher for LA. Our secondary measures were length of postoperative stay, 30 days readmission rate, and mortality.
Ethical considerations
Procedure-specific trust coding was utilized to generate the patient list. Patients were allocated specific numbers to keep the data anonymized and only the principal investigator had the password-protected access to the confidential patient details. The data were securely locked onto the internally protected trust website once the analysis had been completed.
Surgical technique
LA was performed using a three-port technique with 10 mm port at umbilicus. Further 5 mm at left iliac fossa and 5 mm suprapubic ports were placed under direct vision. An endoloop was created extracorporeally. It is our standard practice to create an extracorporeal endoloop by using a standard Roeder knot. 12 Through the fenestrum of the mobile jaw of Johan forceps, we then passed the long end of suture, until we reached knot. Here we loosely approximate jaws of Johan's forceps with utmost care, not to close jaws too tight, as the forceps' serration will damage the suture material otherwise. The long end of the suture is then kept under adequate tension. By applying concomitant gentle push onto and behind the knot, the loosely approximated Johan forceps will then act a knot pusher to deploy the knot at a desired place (Figs. 1–3). In our experience, number 1 polyglactin polyglactin provides a secure knot with optimal strength and robustness. A total of three endoloops were used. Appendix was divided between two proximal and one distal endoloop. Appendix was usually delivered through the umbilical port. 12
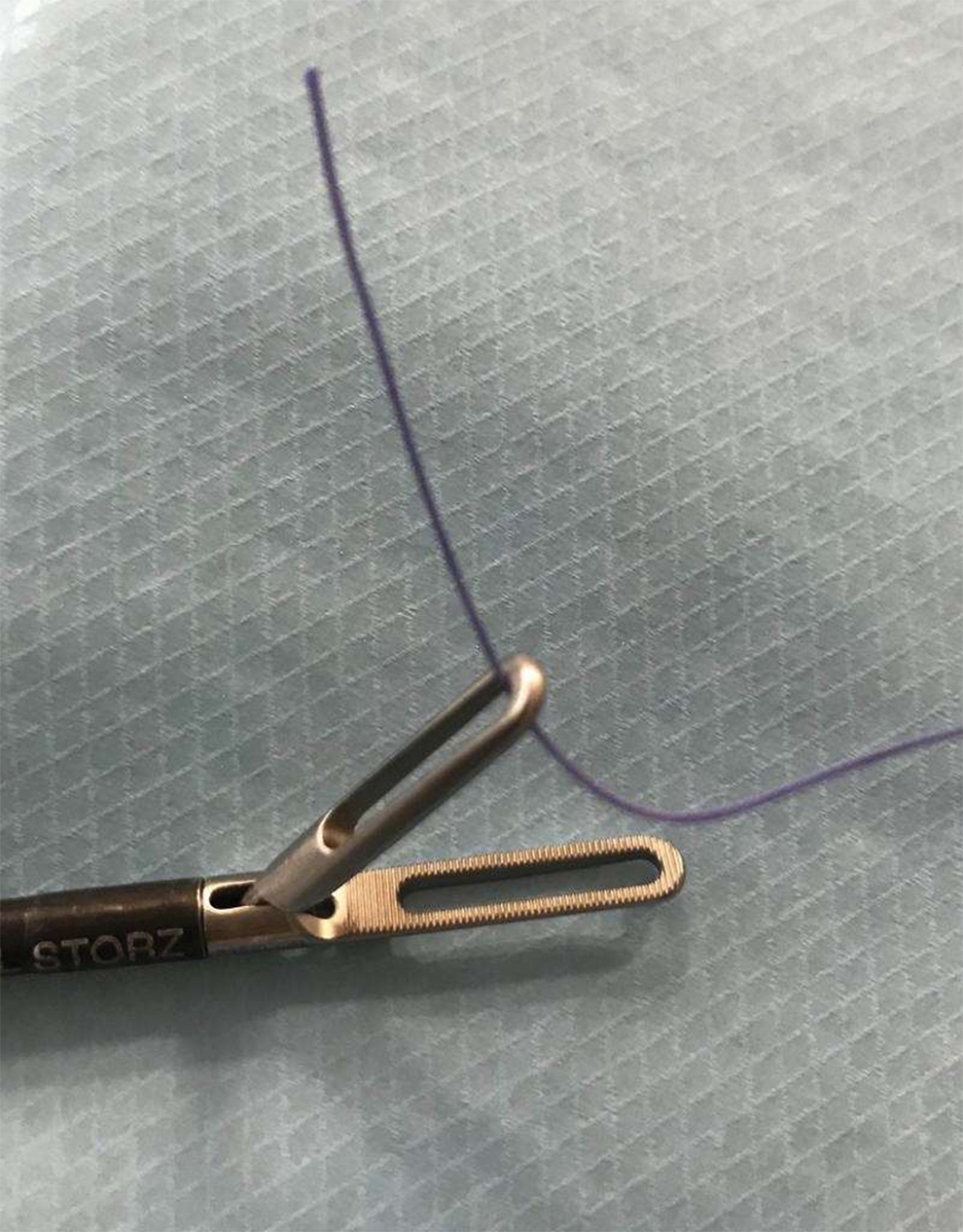
Long end of endoloop passed through the upper jaw of Johan forceps. Color images are available online.

Tip of Johan forceps in close approximation with the knot. Color images are available online.

Secure and precise placement of knot at the desired site for ligature tightening. Color images are available online.
Results
This multicenter study was carried out between March 2014 and June 2019. A total of 227 appendectomies were included. Majority of the appendectomies were performed at Dewsbury and District Hospital. Median age was 24 years (IQR: 16–58) with 58% male preponderance (Table 1). Operative findings were 57% (n = 130) acutely inflamed appendicitis, 16.74% (n = 38) were complicated appendicitis (perforated, gangrenous). Rest of the operative findings were macroscopically normal appendix with no other pathology in 18.06% (n = 41), and macroscopically normal appendix but with gynecological pathologies in 7.9% (n = 18) (Fig. 4). All cases were carried out laparoscopically. There was no conversion to open procedure.
Operative findings.
Gender Distribution
Postoperatively no cases of blowout stump were reported. However, superficial surgical site infections (SSIs) were noted in 3.5% (n = 8). Five of these patients were identified during same admission, whereas 3 of them got readmitted after being discharged from the hospital. Two patients had superficial SSIs that were treated with antibiotics. Whereas the third patient was admitted with a small intra-abdominal abscess (0.4%). It was successfully treated with intravenous antibiotics (Tables 2 and 3).
Thirty Days Readmission Rate
Reasons of Readmissions
Mean hospital stay was 1.89 days (SD 1–5 days). Majority, 81.93%, of patients stayed for <48 hours (Fig. 5). Thirty-day readmissions rate was 4.8%, as 11 patients out of 227 were readmitted. The main reason of readmission was abdominal pain in 8 of 11 patients, whereby no cause of abdominal pain was found. All such patients responded to conservative management. Whereas 3 of 11 patients were admitted with minor wound infections. There was no 30-day mortality in our series. None of the complications or readmissions was related to the surgical technique.
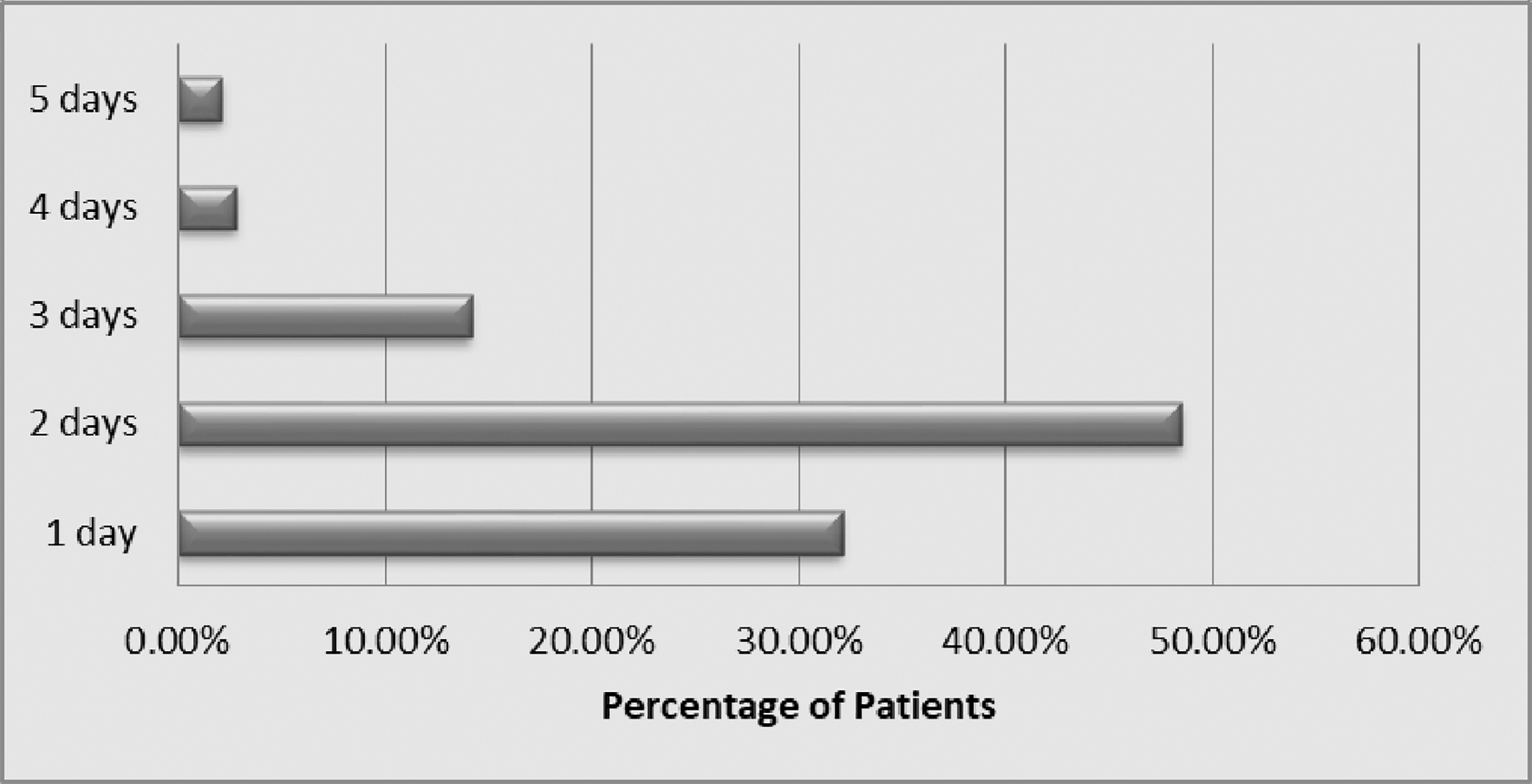
Postoperative stay.
The price of one polyglactin suture pack was $0.69. We required only one pack per case.
To assemble one handmade endoloop with a Roeder knot, our average time was 30 seconds. Hence, we would take ∼90 seconds to make three knots per case.
Discussion
Our results have demonstrated that our technique, which entails deploying of an extracorporeal Roeder knot onto the AS by using Johan forceps as a knot pusher, is safe and cost-effective with low post-operative complications after LA.
Over the past few decades, LA has gradually been becoming a preferred approach, over open procedure, due to its diagnostic ability and therapeutic efficacy with low mortality and morbidity.13,14 There are pros and cons of each technique adopted to secure AS. Dealing with AS is influenced mainly by the degree of inflammation of appendix as well as the surgeon's level of training, experience, and personal preference for particular equipment. 15 An inappropriate management of appendicular stump can lead to life-threatening events such as stercoral fistulas, postoperative peritonitis, and sepsis. 1 Recent Cochrane review found current evidence as insufficient to advocate preference of one technique over other in securing AS. 16 Use of endostaplers is limited by high cost and mandates a 12-mm port, with a risk of potential port site hernia. Furthermore, these may be associated with a risk of adhesional bowel obstruction. Intracorporeal suturing can be technical demanding. Harmonics and ligasure have also been used but their usage is limited by the high cost of installation of equipment. Polymer clips usage is limited by the stump diameter of up to 10 mm. 2 However, acutely inflamed appendix is majority of time much swollen than 10 mm. Extracorporeal sliding knots, described in the literature, involve repetitive steps. We think this is a major pitfall, as these knots usually involve using two hands and additional assistance during the key step for a slight longer duration, when compared with an endoloop. Our technique was not limited by any of the mentioned limitations including the size of the appendicular stump. In our series we dealt with various degrees of inflammation of appendix, with comparable level of complications with rest of techniques described in the literature.
Our results showed no complications related to appendicular stump. Our only complications were surgical site infections (SSIs). Our SSI rates were 4.9%, which is much lower, when compared with the literature, where it has been reported as 2.8%–11.5% with laparoscopic appendectomy.17,18 When it comes to deep tissue SSI, our rate of intra-abdominal abscess was only 0.44%, whereas recent meta-analysis reported it as 1.5%–18.5% after LA. 19 Our findings correspond to postappendicectomy complication rates reported in the literature, which are 6.6% from Turkey, 6 10.24% from Italy, 20 8.7% from the United Kingdom, 21 and 6.9% from Australia. 22 Recent systematic review, regarding use of polymer clips, showed postappendicectomy complications rate of 2.7%. 23 Comparative study, by Ates M & coworkers, on the usage of intracorporeal suturing with titanium endoclips to manage AS during laparoscopic appendectomy, concluded that no statistically significant differences were detected between the groups in terms of hospital stay, follow-up time, and perioperative and postoperative complications (P > .05). Our results are comparable to this study but with additional benefit of no return to theater. 24
Our results showed mean hospital stay as 1.89 days, with readmission rate of 8%. These outcomes match the various reports in the literature.22,25–27 Abu Foul et al. reported an average hospital stay of 3.41 and 9 days (uncomplicated appendicitis versus complicated appendicitis). 25 A large multicenter study from the United States reported its readmission rate of 8.7%. 26 Whereas another large multicenter study from Australia, with total of 1189 patients recruited across 27 centers, found its readmission rate as 6.6%, 27 after LA.
Our handmade endoloops are the cheapest of all techniques available to secure AS and yet safe too. These findings have been supported by Yıldız and Koca, who also found their handmade endoloops cost-effective. There were no reports of difference of complications rate and hospital stay, when a comparison was drawn between staplers, preformed endoloops, handmade endoloops, and hemo-o-lok. 15 Comparing it with rest of available methods, our handmade endoloops are the cheapest available in the market. Price of our handmade three endoloops was $0.69, whereas price of three commercially supplied prepacked endoloops is $67.58, 28 that of polymer clips is $28.96, 23 and that of endostaplers was ∼$689.55. 6 So in our cost analysis, we spend $156.53 to carry out these 227 appendicectomies. By using conventional endoloops and polymer clips, the total cost would have been $15339.72 and $6574.16, respectively. Gross saving, by incorporating our handmade endoloops and technique instead, would have then been $15183.19 and $6417.64, respectively.
The real strength of our study is the prospective design. We did not cherry pick our cases but instead followed a pragmatic approach. We dealt with a variety of degrees of inflammation of appendix, whereby extracorporeal Roeder knot was deployed safely on respective AS.
Our study had few limitations too. We have not randomized other methods to secure AS. This is due to the standard practice of the senior author to handmade endoloops and deployed those by knot pusher at AS. He achieved competency during his higher surgical training after undergoing vigorous training in the said technique. Our study is further limited by the operation cost associated with the requirement of the additional operation theater time to fashion these endoloops by a junior trainee. Perhaps a practice outside the operation theater can reduce the time a beginner would take to make these endoloops. Our technique is safe. Surgeons do need brief training. For United Kingdom trainees, this is a much easier skill to acquire, as learning of Roeder's knot is one of the main components of core laparoscopic skills course conducted by Royal College of Surgeons of England. We recommend teaching & training of extracorporeal Roeder's knot, later simulation or laboratory-based training (models/box trainer), and subsequent use under supervision during the learning curve.
Conclusion
Use of Johan forceps as knot pusher for Roeder's knot is a safe, feasible, cost-effective, and easily reproducible technique for carrying out LA.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.