
Abstract
Background:
Laparoscopic partial splenectomy is a surgical option for removing part of the spleen with a pathological mass in a way that ensures preservation of the spleen's physiological functions. We aimed to evaluate the efficacy and feasibility of this procedure, performed while preserving the blood supply from the left gastroepiploic artery, in children.
Materials and Methods:
Following institutional review board approval, this retrospective study was conducted on patients who, between January 2015 and December 2019, underwent laparoscopic partial splenectomy with preservation of blood supply from the left gastroepiploic vessels. In the article, we described patient indications for surgery, surgical technique, surgery time, complications, and follow-up outcomes.
Results:
Eleven patients (mean age: 12.3 ± 3.4 years) underwent laparoscopic partial splenectomy. Indications for surgery included nonparasitic cysts (n = 8), pseudocysts (n = 2), and hamartomas (n = 1). The mean benign mass diameter was 60 ± 22 mm. The mean operative time was 193.2 ± 55.1 minutes. The mean size of the retained lower pole was 31.1% ± 3.8%. There was no conversion to open splenectomy or any significant complication. The mean postoperative stay was 9 ± 0.7 days. No thrombosis of the splenic and portal veins was noted in the follow-up period, and no splenic remnant infarction occurred.
Conclusions:
Laparoscopic partial splenectomy with preservation of blood supply arising from the left gastroepiploic vessels seems to be safe in children. However, a larger study is needed to confirm our results.
Introduction
The indications for splenectomy include a ruptured spleen, treatment of splenic cysts and abscesses, and tumor resection; however, the most frequent medical indications comprise hematological disorders. 1 Life-threatening sepsis represents the most important complication of splenectomy, and is mainly caused by Streptococcus pneumonia and other encapsulated organisms. 2 The annual incidence of life-threatening postsplenectomy sepsis in adults is estimated to be 0.23%–0.42%, with a lifetime risk of 5%. 3 Although immunization and prophylactic antibiotics have decreased the overall risk, there are concerns about serotypes not included in the vaccines. Moreover, the risk of developing life-threatening infection after splenectomy persists for decades. 4
Other postsplenectomy complications include acute hemorrhage, severe thrombosis, and acute pancreatitis, which can occur within a short period after the surgery. For instance, thromboembolic complications following splenectomy for hematological disorders occur in up to 10% of the patients and may range from portal vein thrombosis to pulmonary embolism and deep vein thrombosis. 5 Considering these factors, the benefits of splenectomy must be balanced against its immediate and long-term risks. 6 Although autologous splenic tissue transplantation is an option for preserving splenic function, it is inferior to partial splenectomy in terms of regeneration, blood flow, reticuloendothelial clearance, and immunological function. 7
The increased awareness of asplenia-related life-threatening complications has led to the development of parenchyma-sparing splenic resections. The indications include idiopathic splenomegaly, splenic cysts, benign tumors, metastases, splenic infarctions, iatrogenic injuries, and hereditary spherocytosis. 8 Focusing on partial splenectomy for benign lesions of the spleen, the laparoscopic approach is as safe and effective as laparotomy.7,9,10
The vitality of the splenic remnant and its vascular supply, with preservation of the blood supply through the left gastroepiploic artery (LGEA), remains a goal of partial splenectomy. Some authors have suggested maintaining the spleen's lower pole, while others have suggested maintaining the spleen's upper pole. 8 In most cases, the vital remnant of the spleen is supplied with the vessels of the splenic artery. Since 2000, we started to perform partial resections of benign splenic lesions by laparotomy, while preserving the lower pole supplied by branches of the left gastroepiploic vessels. 11 This approach proved to be suitable for benign formations located in the upper and central portions of the spleen (Fig. 1), and thus, we switched to laparoscopy in 2015. This study aimed to describe a series of pediatric patients who underwent laparoscopic partial splenectomy for focal benign splenic lesions with this innovative technique.
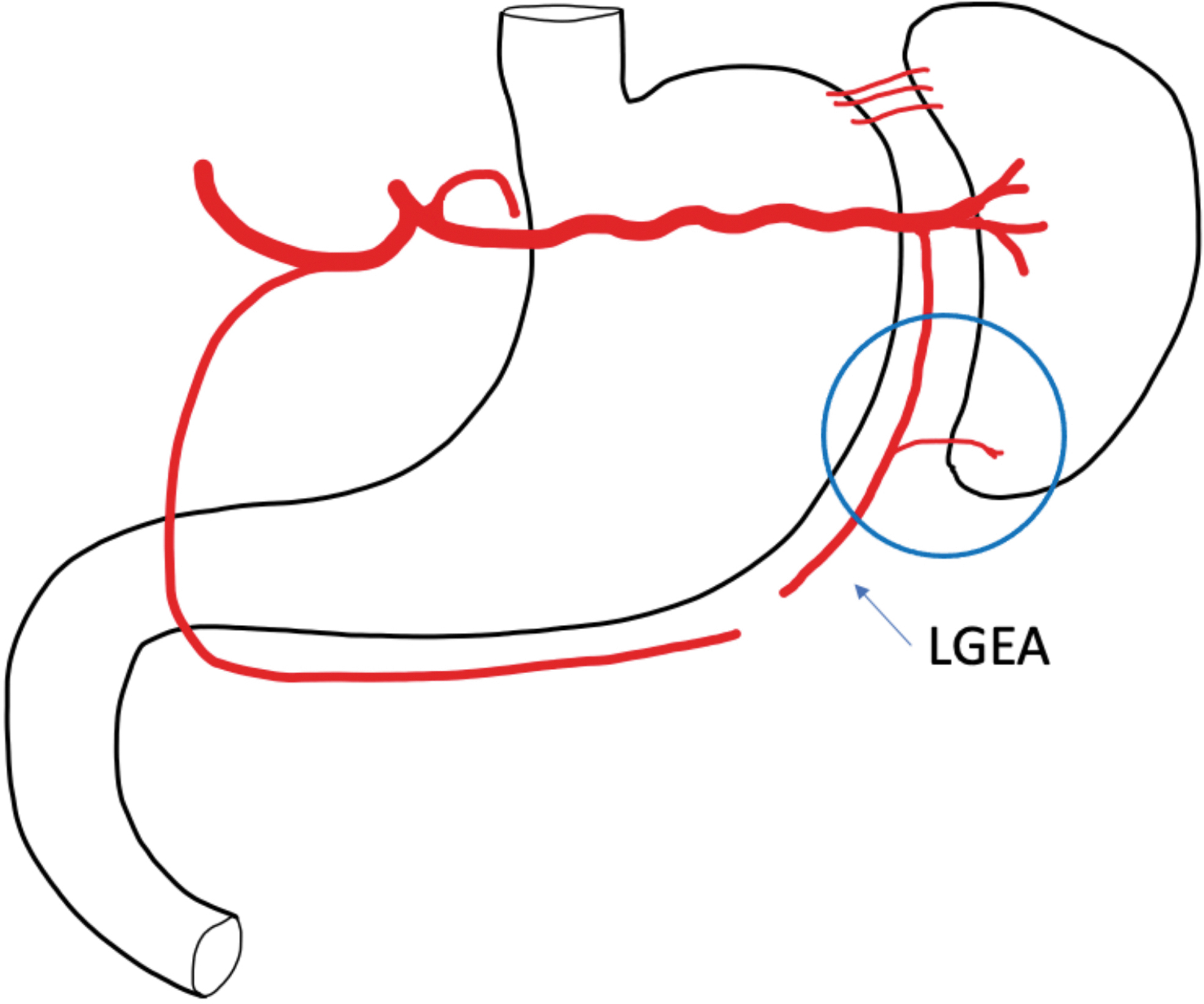
Scheme of branches of the LGEA entering the spleen's lower pole. LGEA, left gastroepiploic artery.
Materials and Methods
Patients and indications
This retrospective study collected data recorded between January 2015 and December 2019. All consecutive patients treated at the Pediatric Surgery Department of Comenius University and the National Institute of Children's Diseases in Bratislava, Slovakia, were included. The indications for laparoscopic partial splenectomy with lower pole preservation included the presence of clinical symptoms and an increase in the lesion size (confirmed by sonography and computed tomography [CT]). Institutional review board approval was obtained for this study.
Preoperative procedures
All patients received preoperative prophylactic immunization against pneumococci, meningococci, and Haemophilus influenzae Type B. Immunization was performed in cooperation with a hematologist, using a meningococcal group A, C, W-135, and Y conjugate vaccine Nimenrix; meningococcal group B vaccine Bexsero; and polyvalent pneumococcal vaccine Pneumovax 23. All patients also received postoperative prophylaxis with antibiotics. We collected data on the patients' hematological and clinical features, indications for partial splenectomy, and radiographic evaluations of the spleen.
Perioperative management
Data on preoperative and postoperative laboratory results (including the complete blood cell and platelet counts, abdominal ultrasonographic findings, and abdominal CT findings) were obtained from the medical records. The operative time, blood loss, need for transfusion, and length of postoperative stay were evaluated. The possible occurrences of intraoperative and immediate postoperative complications were recorded.
Postoperative follow-up
Splenic remnant growth and vitality were also investigated. Patients were re-assessed 1, 3, and 6 months postoperatively. The patients' laboratory values were compared to their corresponding preoperative and postoperative values, including the ones recorded at follow-up examinations.
Surgical technique
The surgical setting is described in Figure 2. The patients were positioned prone with a slight left flank elevation. A 4-port approach was used (Fig. 3). Pneumoperitoneum was created using a Veress needle, and the CO2 pressure was maintained between 10 and 14 mmHg. Port for the camera with adjustable diameter from 5 to15 mm was placed in the umbilicus. Three operative 5-mm ports were placed to the epigastrium, in the midline between the epigastrium and the umbilicus, and into the left hypochondrium.

Operative position on the back with the left side raised under the left flank.

Positioning in the surgeon-spleen-monitor axis. Four-port access.
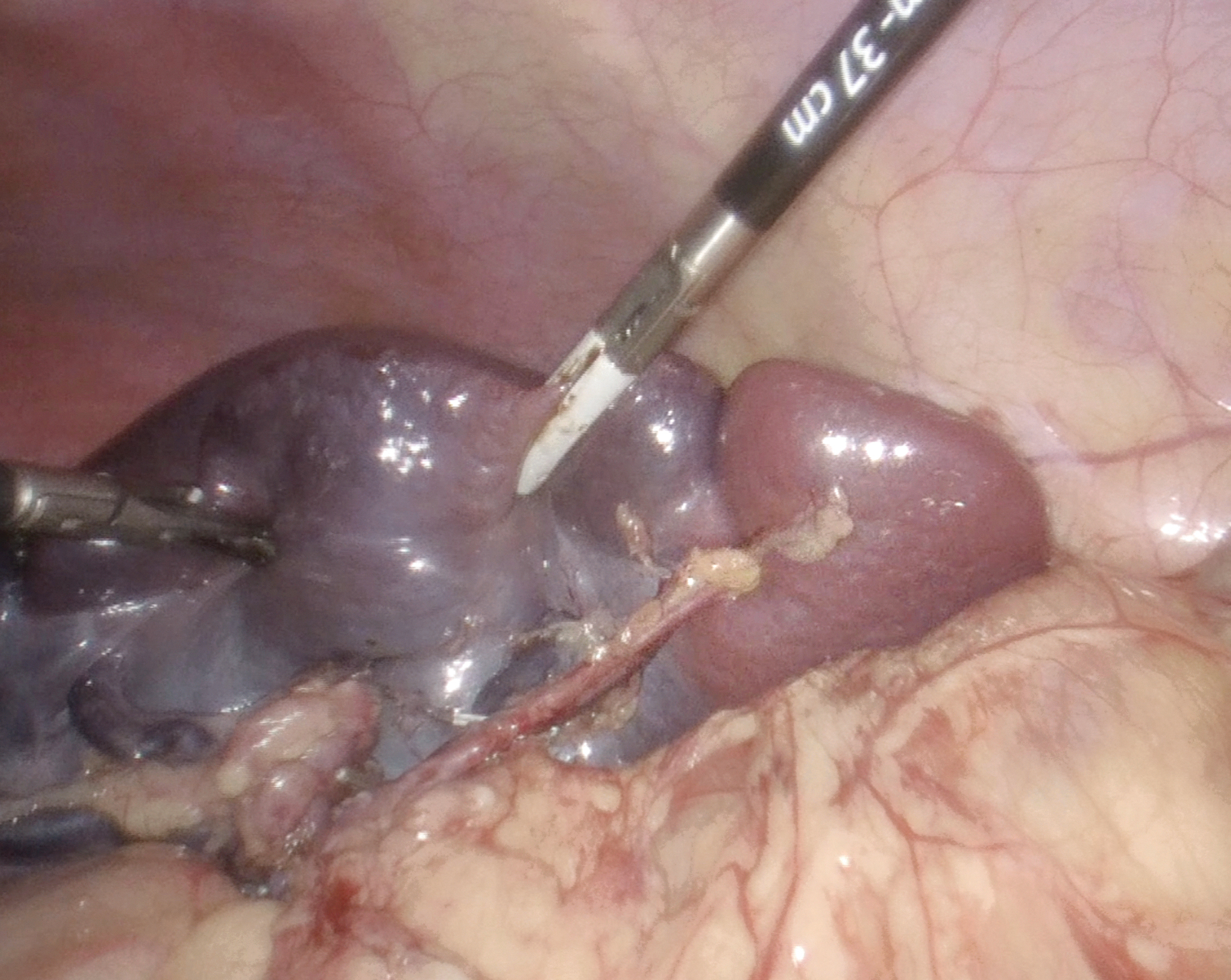
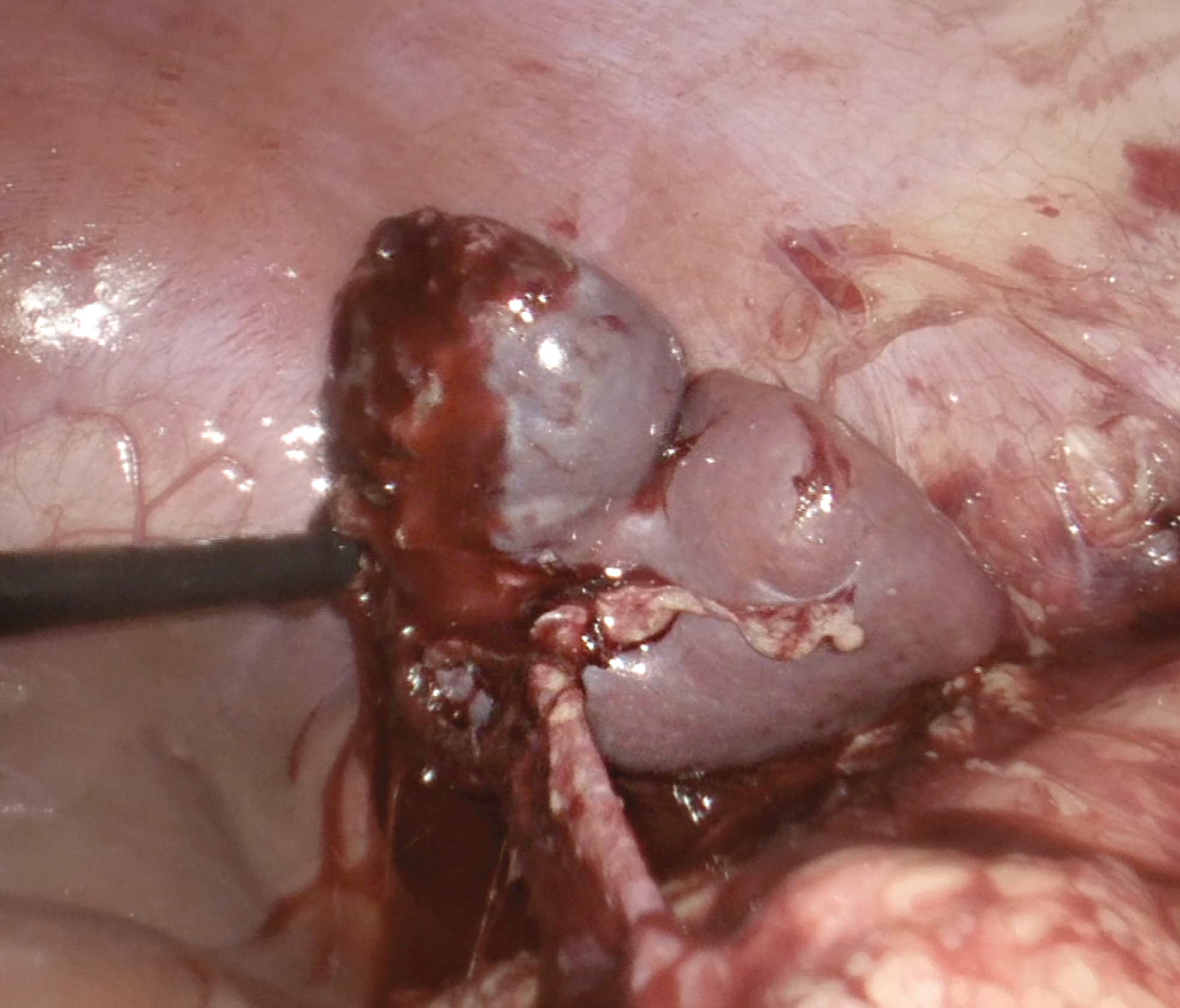
The operating table was further rotated to the patient's right to achieve a 45° position for the procedure (Fig. 4). The lower pole of the spleen was then examined to verify whether the branches of the gastroepiploic vessels were separated and whether they supplied the lower pole of the spleen outside the branching of the hilar vessels (Fig. 5). The splenorenal ligament was partially released, and the stomach was pulled medially. Short gastric vessels were divided with LigaSure to release the spleen's upper pole (Fig. 6). The artery and vein were clipped and divided (Fig. 7). The remaining ligaments were divided extremely carefully, because large splenic cysts can adhere to the diaphragm. At this stage, the demarcation between the ischemic and perfused portions of the spleen was evident, and 20%–30% of the healthy parenchyma was identified (Fig. 8). The spleen was then divided 1 cm from the demarcation line in the ischemic area (Fig. 9). All small bleeding vessels were sealed using bipolar LigaSure coagulation. Because the splenic remnant is very mobile with impending torsion (Fig. 10), it was fixed to the abdominal wall with a large stitch passing through the parenchyma (Fig. 11). The spleen was inserted into an endobag through the umbilical port and extracted by fragmentation. Because we left the resection area of the spleen free, a drain was inserted into the splenic bed through the subcostal port when required.
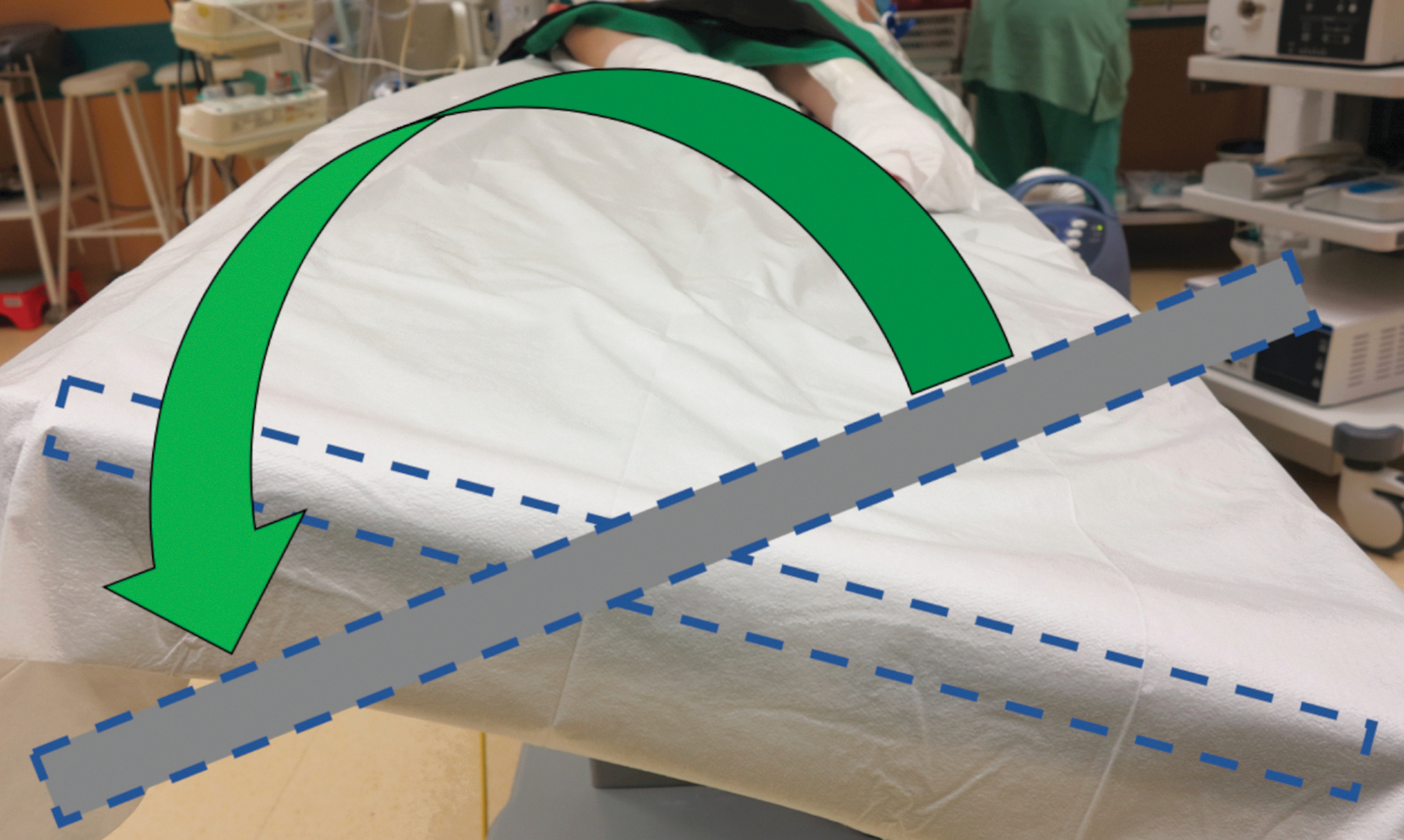
By rotating the table to the left side, the patient was put into a horizontal position to insert the first port. Then we rotated the table to the right to a 45° lateral position for the operation.

Perioperative examination of the branches of the LGEA and veins entering the spleen's lower pole. LGEA, left gastroepiploic artery.

The interruption of short gastric vessels.

Clipping of the splenic artery centrally with two clips and peripherally with one followed by cutting. Similarly, we intersected the splenic vein.
After hilar and short gastric devascularization, the demarcation line of the ischemic and perfused part of the spleen was clear.

The spleen parenchyma was intersected 1 cm from the demarcation line in the ischemic zone using LigaSure.
A well-perfused splenic remnant on the vascular LGEA pedicle is very mobile with a risk of twisting. LGEA, left gastroepiploic artery.

Fixation of the spleen remnant through the parenchyma to the lateral abdominal wall by a stitch to prevent torsion.
Statistical analysis
Descriptive statistics are reported as absolute frequencies and percentages. Semiquantitative and quantitative variables are described using medians and interquartile ranges. A two-tailed Fisher's exact test was used to compare the categorical variables, and a paired t-test was used to compare the continuous variables. Statistical analyses were performed using SPSS, version 27 (IBM, NY). Statistical significance was defined by P < .05.
Results
Between January 2015 and December 2019, laparoscopic partial splenectomy was performed in 11 patients between 6 and 18 years of age (mean age: 12.3 ± 3.4 years). The male-to-female ratio was 0.6:1. Demographics are reported in Table 1. Indications for partial splenectomy included nonparasitic cysts (n = 8), hamartomas (n = 1), and posttraumatic pseudocysts (n = 2). Six patients had abdominal pain, and 5 were asymptomatic. In 3 patients, the indication for partial splenectomy was cyst growth with gradually increasing abdominal discomfort. All patients underwent preoperative abdominal CT to confirm the benign nature of the splenic lesions and to demonstrate blood supply to the healthy spleen. The mean diameter of the lesions was 60 ± 22 mm (range, 20–185 mm). The upper pole and the central portion of the spleen were involved in 7 and 4 patients, respectively. The largest splenic cyst was identified in a 15-year-old patient and measured 185 × 160 × 162 mm, with an estimated volume of 2400 mL. In all patients, the lower pole was healthy. The mean size of the retained lower pole was 31.1% ± 3.8%.
Demographic and Clinical Data
As shown in Table 2, the mean operative time was 193.2 ± 55.1 minutes (range, 73–294 minutes). The median estimated blood loss was 110 mL (range, 20–400 mL). Two patients required postoperative blood transfusion, but none required conversion to open surgery. Two patients experienced postoperative complications: 1 experienced fluid collection around the splenic recess and 1 experienced pleural effusion. The mean postoperative stay was 9 ± 0.7 days. No case of postoperative complications, including bleeding, infection, or pancreatic fistulas, was noted. All patients received long-term prophylactic antibiotics and antiplatelet therapy and were discharged uneventfully. Postoperative follow-up demonstrated a change in the splenic remnant's size during the follow-up period. The mean volume of the spleen remnant at discharge was 52.6 ± 28.5 mL and after 6 months, the mean remnant size was 63.6 ± 42.2 mL, respectively; this difference was not statistically significant (P = .591). None of the patients experienced overwhelming sepsis during follow-up. The laboratory results during the follow-up period are reported in Table 3.
Perioperative Data
ICU, intensive care unit.
Laboratory Values: Preoperative and Follow-Up
Discussion
EIn 1991, Delaitre, and Maignien reported the first case of laparoscopic splenectomy, 12 and since 1996, it has been a standard method. 13 The increased awareness that splenectomized patients face a lifelong risk of overwhelming life-threatening infections led to the popularization of partial splenectomy, 14 which was first described by Christo, Morgensten, and Shapiro in 1980.15–17 Uranues et al. assessed the safety of laparoscopic partial splenectomy for benign and malignant spleen diseases in 38 patients. The indications included splenomegaly of unknown origin, splenic cysts, benign tumors (hamartomas), and metastases from ovarian carcinomas and schwannomas. They observed no postoperative mortality or reoperation, and concluded that laparoscopic partial splenectomy is safe for patients with localized benign or malignant diseases of the spleen. 18
In 2018, Serra et al. 19 reported the first case of partial laparoscopic splenectomy in a 7-year-old child with splenic hamartoma. The procedure was performed after segmental chemoembolization of the splenic artery for preserving the branches of the spleen's lower pole. Dissection was performed using a harmonic scalpel and titanium clips. The authors recommended intraoperative examination of a frozen section of the specimen to identify any malignancy.
Our approach was inspired by the finding of a wholly separated lower pole of the spleen in a patient with spleen rupture. 11 Since 2015, we have performed laparoscopic partial splenectomies using this preservation method. Of note, we did not diagnose any benign or malignant mass in the lower pole of the spleen in this study; therefore, we could use the vascular supply from the left gastroepiploic vessels.
There are different techniques for performing a partial splenectomy. Slater et al. 20 described a laparoscopic approach for partial splenectomy in children with hereditary spherocytosis. They advocated preserving the upper pole with blood supply from the short gastric vessels. The results of our experience are in accordance with those of Vasilescu et al., 21 who advocated leaving the lower pole, rather than the upper pole, to reduce postoperative complications. They suggested that preservation of the lower pole could be the gold standard for optimal evaluation of the residual splenic tissue. Vasilescu et al. 22 also compared conventional and robotic laparoscopy for the partial resection of the spleen; they highlighted the precision of vascular dissection and a more accurate evaluation of the remnant volume with the robotic method.
In cases of partial splenectomy in children, the percentage of the preserved splenic remnant is a critical consideration for maintaining hematological and immunological functions. Previous studies have demonstrated that preserving 25% of the splenic parenchyma is sufficient for permitting an appropriate immunological response to antigen stimulus.14,23
Many authors have reported partial splenectomies in patients with congenital hemolytic anemia, including sickle cell disease, thalassemia, and hereditary spherocytosis; these authors managed to preserve 10%–30% of the spleen, supplied by the short gastric arteries.19,22,24 Hafezi et al. 24 advocated a splenic preservation of 10%–15%, rather than of 15%–20%, due to disease recurrence and secondary procedures such as completion splenectomy and delayed cholecystectomy.
In our study, there was no risk of recurrence due to splenic volumes, because there are no patients with haematological disease in the cohort. On the contrary, after removing the pathological process, we attempted to preserve the entire perfused remnant.
Both the liver and spleen can be regenerated after a significant parenchymal loss. Spleen regrowth has been reported, 25 and normal immunoglobulin M levels have been reported in such cases. Thus, it can be assumed that the spleen remnant provides a sufficient level of immunoglobulins.
In this study, laparoscopic partial splenectomy was accomplished by preserving an adequate lower-pole remnant (>25%), while preserving the blood supply by the LGEA. To prevent torsion of the spleen remnant (which is likely to occur in cases of an unfixed, wandering spleen), we decided to fix it to the corresponding site in the left hypochondrium in the native position.
Bader-Meunier et al. described the growth of most splenic remnants after laparoscopic subtotal splenectomy and concluded that growth velocity is high during the first postsurgical year, but slows down with stabilization of the remnant size in the long term. 14 However, we did not observe remnant growth in our study; conversely, the remnants decreased at the 6-month follow-up, suggesting the need for longer monitoring. Remnant regrowth has been reported in patients with hereditary spherocytosis, which induces increased spleen function. 14 However, in our study, no patient had systemic hematological diseases or hypersplenism.
Collateral vascularization of the upper pole through the short gastric vessels appears to be more effective than gastroepiploic collateral vascularization, which may cause poorer perfusion. 25 We can assume that the resection line in the ischemic zone may undergo postoperative scarring with a temporary reduction in the remnant size. However, we did not observe any loss of remnant due to ischemia in any patient. It seems that follow-up may be helpful in further evaluation of the function and size of the splenic remnant.
This study has some limitations, the most significant being the small number of included patients. An inherent limitation was that there were no patients with hematological diseases, hypersplenism, and splenomegaly. Furthermore, we were able to apply this procedure only because the pathological lesion did not affect the lower pole of the spleen. Nonetheless, the cohort of patients who underwent laparoscopic partial splenectomy was homogenous, thus supporting the reliability of our results.
Conclusion
To conclude, a separate vascular supply from the LGEA to the lower pole was consistently recorded in all patients. None of the patients had lesions affecting the spleen's lower pole. Based on our data, the blood supply from the LGEA seems sufficient for preserving more than 25% of the vital spleen tissue, which is believed to be adequate for retaining long-term immunological and hematological functions.
However, confirmation of the relationship between functionality and the size of the splenic remnant remains a topic of debate. The method described appears to be safe for children with local benign spleen processes. However, more studies are needed to confirm our findings and their consistency in the long term.
Authors Contribution
All authors reviewed the results and approved the final version of the article.
Footnotes
Acknowledgments
The authors wish to thank the reviewers who read the numerous revisions and showed a lot of patience and professionalism. They also thank A.P. Prato, who has been an ideal mentor, offering advice and encouragement.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.