
Abstract
Background:
For laparoscopic gastrectomy, it is significant to reduce the incidence of anastomotic leakage. The authors develop a novel technique for safe extracorporeal anastomosis that employs the bronchus forceps to reinforce the esophageal ring.
Methods:
From January 2017 to July 2020, 173 consecutive patients with gastric cancer received laparoscopic total gastrectomy or laparoscopic proximal gastrectomy. One hundred thirty-one patients only underwent extracorporeal anastomosis with a purse-string suture instrument (PSI) and a 25 mm circular stapler (Ethicon Intraluminal Circular Staplers CDH25A, Ethicon) (Conventional Surgery Group). In addition to these tools for extracorporeal anastomosis, the surgeon creatively used bronchus forceps to reinforce the esophageal ring on the anvil of circular stapler in 42 patients (Bronchus Forceps Ligation Group). The condition and the mean diameter of the narrowest part of the esophageal rings, postoperative outcomes, and complications were compared between the two groups.
Results:
Under direct vision, the esophageal rings were more complete in the Bronchus Forceps Ligation Group. Furthermore, the mean diameter of the narrowest part of the esophageal rings in the Bronchus Forceps Ligation Group was wider than that in the Conventional Surgery Group (4.34 ± 0.84 versus 2.68 ± 0.74 mm; P < .001). Meanwhile, the incidence of anastomotic leakage was lower in the Bronchus Forceps Ligation Group. Although reinforcing the anvil with the bronchus forceps will add additional surgery time, almost all can be done in less than 5 minutes.
Conclusions:
With applying the bronchus forceps to reinforce the esophageal ring on the anvil of the circular stapler, the extracorporeal anastomosis can be performed more safely.
Introduction
Gastric cancer (GC) is a common malignant tumor in the gastrointestinal tract. Around the world, GC ranks third among cancer deaths, and its incidence rate ranks fifth. 1 The treatment of GC is mainly based on surgery, among which proximal gastrectomy and total gastrectomy are the two common surgical procedures. 2 In both cases, there are various ways to reconstruct the digestive tract after surgery. However, either surgical approach requires an anastomosis with the esophagus.3,4 Excluding the manual anastomosis, the equipment can be broadly divided into two categories—circular staplers and linear staplers. 5 Both are preferred for the esophageal-jejunostomy (EJ). 6
Due to the progress of the medicine and laparoscopic technology in recent years, totally laparoscopic total gastrectomy (LTG) has become feasible. 7 However, the laparoscopic anastomosis is complicated, technically demanding, and not widely available. So far, extracorporeal anastomosis is still common. 8 However, in some cases, especially in patients with gastric tumor invading the lower esophagus, obesity, or large anteroposterior diameters, it is difficult to execute the extracorporeal anastomosis because of the narrow and deep surgical field. 9 In addition, when circular staplers are used for extracorporeal anastomosis, the esophagus ring can be weak and even discontinuous, increasing the risk of anastomotic leakage and postoperative complications. Meanwhile, the anastomotic leakage could result in more postoperative complications, reoperation and even death. 10
The study describes a novel anastomotic technique that reduces the incidence of anastomotic leakage and makes the esophageal ring fuller and wider at its narrowest part after laparoscopic gastrectomy. The details and evaluation of this technique are described below.
Patients and Methods
Patients
We retrospectively collected the clinical data of 173 consecutive patients with GC, who had undergone extracorporeal anastomosis with the 25 mm circular staplers and conventional purse-string suture instrument (PSI) after laparoscopic proximal gastrectomy (LPG) or LTG between January 2017 and July 2020. Patient's clinicopathological features are summarized in Table 1. In 42 of them, we further used the bronchus forceps to reinforce the esophageal ring on the anvil of circular stapler (Bronchus forceps Ligation Group). The remaining 131 patients were artificially assigned to the Conventional Surgery Group. We observed the operative outcomes, postoperative recovery, and postoperative complications of both groups.
Patient's Clinicopathological Features Compared Between Conventional Surgery Group and Bronchus Forceps Ligation Group
ASA, American Society of Anesthesiology; BMI, body mass index; LPG, laparoscopic proximal gastrectomy; LTG, laparoscopic total gastrectomy; SD, standard deviation.
Each patient signed an informed consent before surgery. Patients were managed based on the critical protocols of our institution. The Institutional Review Board of Southwest Medical University approved this retrospective study.
Surgical techniques
We performed Roux-en-Y reconstruction after LTG. Also, double-tract reconstruction was performed after LPG. Before the operation, the instruments were prepared first. In addition to the circular stapler and PSI, the bronchus forceps was required (Fig. 1).

Surgical equipment.
Under the condition of general anesthesia, the patient was placed in the split-leg supine position. The surgeon stood on the left side of the patient, while the first assistant stood on the right side of the patient, and the laparoscope operator stood between the patient legs. After pneumoperitoneum was established, a 10 mm camera trocar was introduced blow the umbilicus. Four additional trocars were created in the upper abdomen (Fig. 2).
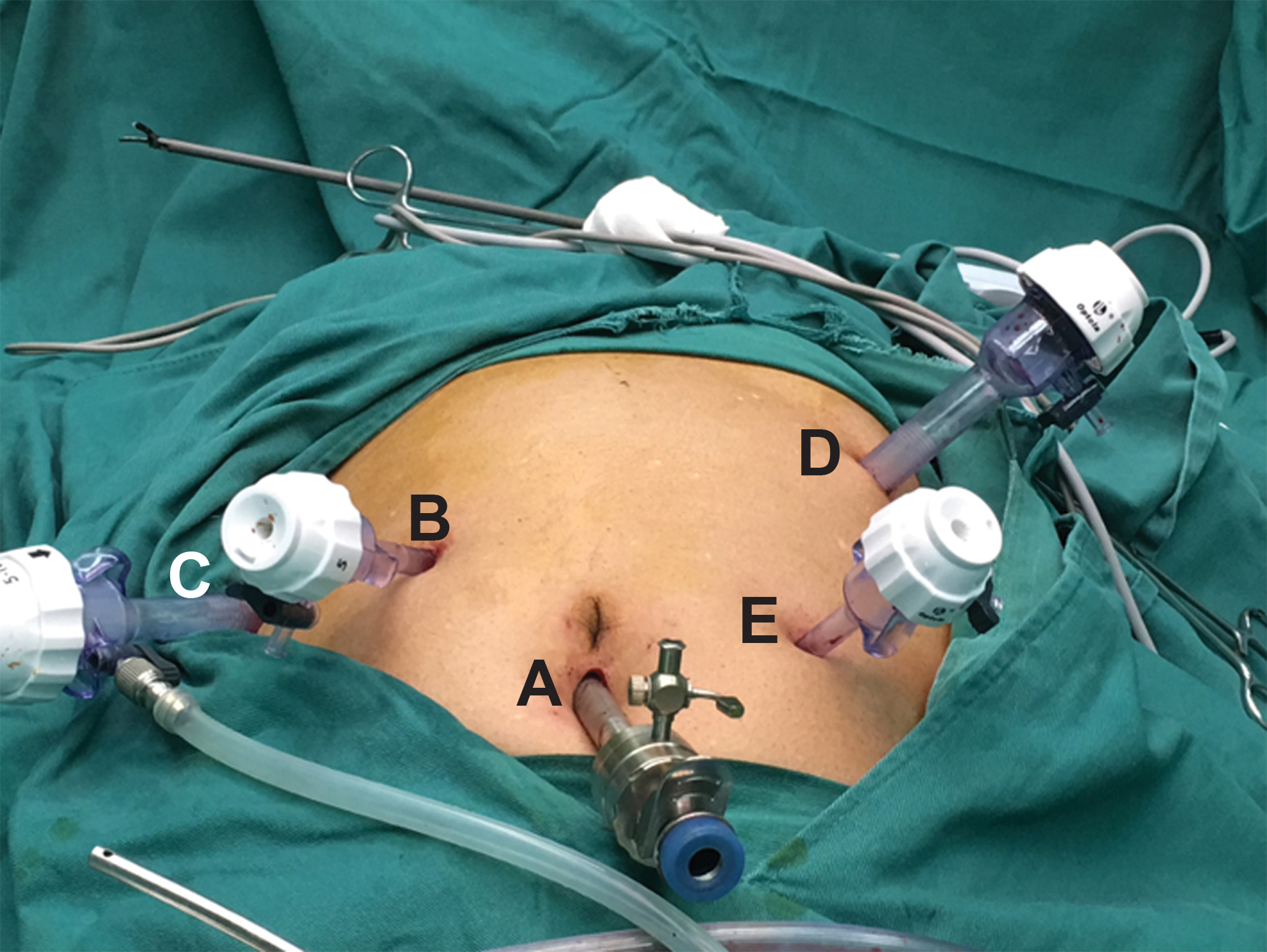
Placement of trocar.
LPG, LTG, and en bloc lymph node dissection were performed as described in the Japanese classification of gastric carcinoma 11 and the Japanese gastric treatment guidelines. 12 Then the esophagus located proximal to the tumor was bared under the laparoscope. After the pneumoperitoneum was closed, a surgical incision, ∼5 to 8 cm, was made under the xiphoid. The surgeon clamped the naked esophagus about 3–5 cm away from the upper edge of the tumor by PSI, and used two straight needles to thread through the entrance hole of the PSI from left to right. Next, the distal end of the esophageal stump clamped by PSI was transected by scissors before the PSI was removed. Finally, the anvil of the circular stapler was inserted into the esophagus and secured with a knot by purse-string suture (Fig. 3).
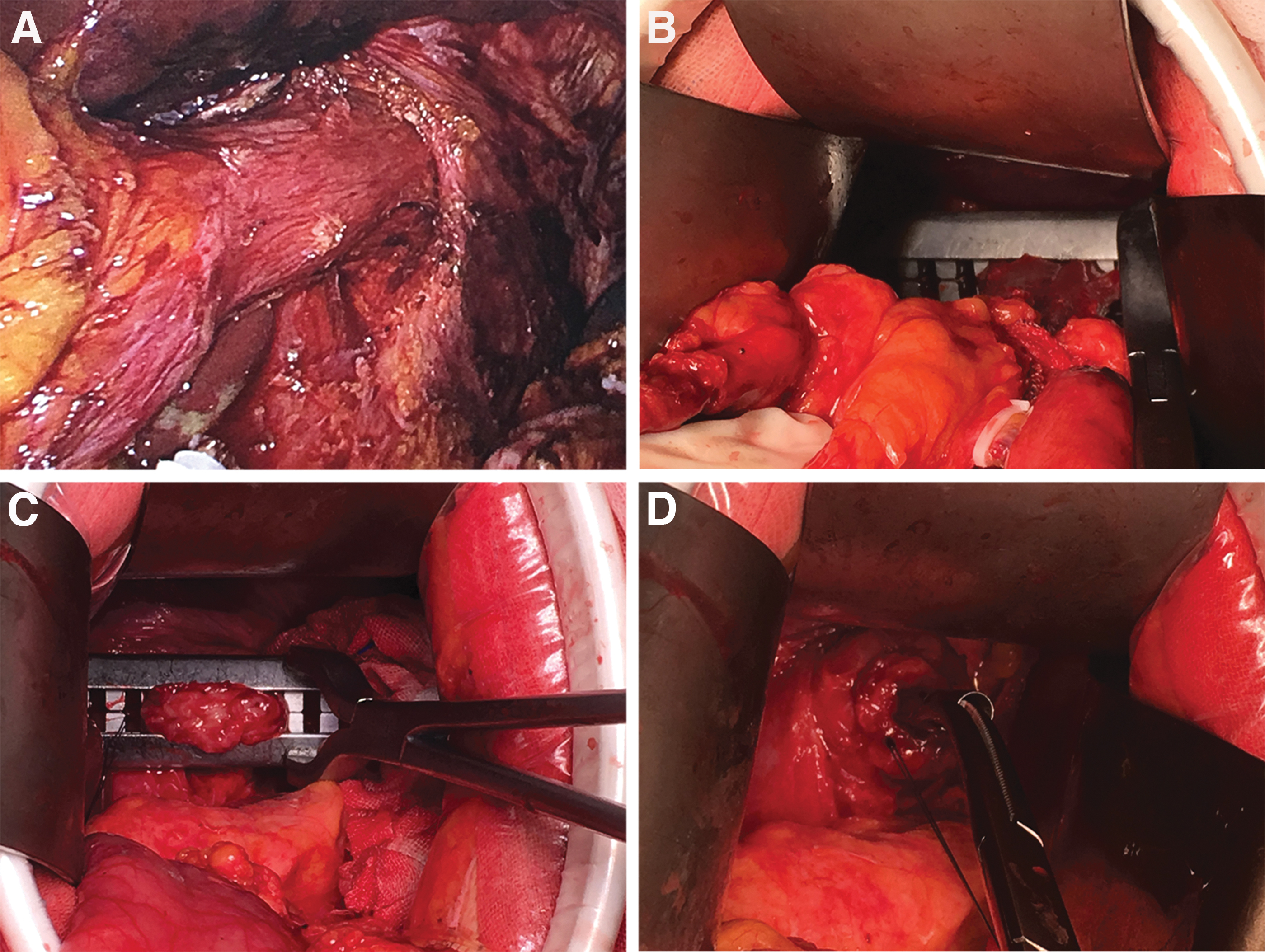
Placement of circular stapler.
Different from the traditional anvil placement, the novel technique applied the bronchus forceps to strengthen the esophageal ring on the anvil of 25 mm circular stapler with two perpendicular ligations on the lower edge of the purse-string suture, after the anvil was fixed by PSI in the esophageal stump (Fig. 4).
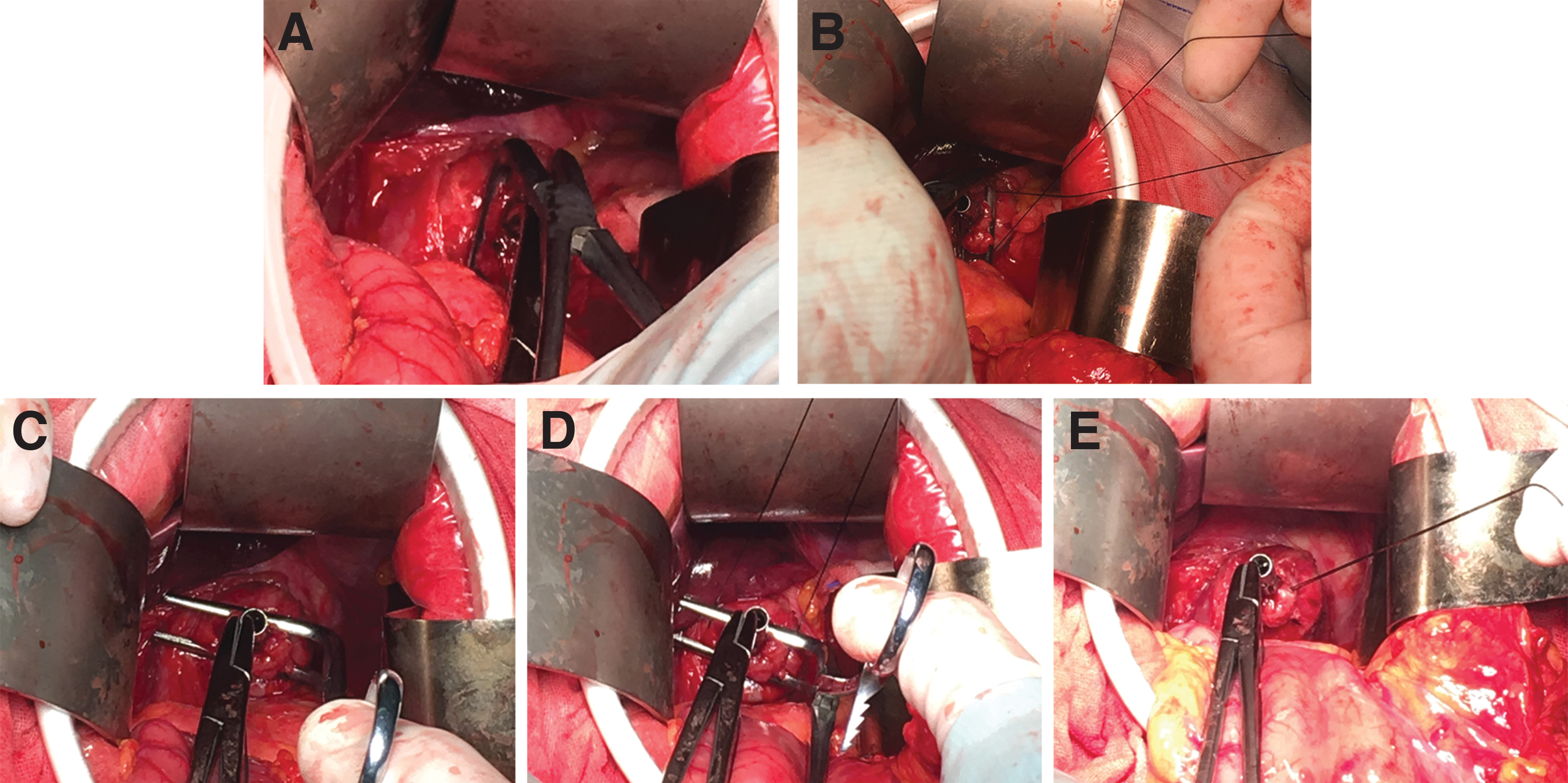
The novel technique.
The jejunum was cut at 25 cm from the ligament of Treitz with a linear stapler. Then a circular stapler was inserted into the distal jejunum stump, and the center rod of it was brought out to pierce the bowel wall. After ensuring no torsion of distal jejunum and no other organ injury, EJ anastomosis was performed by circular stapler. Finally, the stump of the distal jejunum was closed with a linear stapler, and then the staple line was reinforced with an absorbable running suture. For patients who received LPG, the surgeon executed the double-tract reconstruction.
Statistical analyses
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS®) version 23.0. Quantitative data were described by mean ± standard deviation if they obeyed normal distribution, otherwise they were described by median and upper and lower quartiles; qualitative data were described by number of cases and percentage. The comparison of quantitative data between two groups was based on whether the data obeyed normal distribution using Student's test or Mann–Whitney U test, respectively. The comparison of qualitative data was based on whether the data were ordered using Mann–Whitney U test or Pearson chi-square test, and when the theoretical frequency was too small, the Fisher's exact probability method (Fisher's exact test) replaced the chi-square test. P < .05 was considered statistically significant.
Results
Clinicopathological features
Table 1 shows the summary of patients' clinicopathological features. There were 131 cases in the Conventional Surgery Group and 42 cases in the Bronchus Forceps Ligation Group, with average ages of 61.7 ± 9.8 years and 63.8 ± 10.1 years, respectively (P = .231). In the Conventional Surgery Group, 95 (72.5%) patients were male compared to 29 (69.0%) in the Bronchus Forceps Ligation Group (P = .664). The mean BMI in the Conventional Surgery Group was 19.1 ± 3.0 kg/m2 compared to 19.3 ± 2.7 kg/m2 in the Bronchus Forceps Ligation Group (P = .712). Seventy-three (55.7%) patients received LPG in the Conventional Surgery Group compared to 23 (54.8%) patients in the Bronchus Forceps Ligation Group (P = .913). There was no significant difference in American Society of Anesthesiology (ASA) classification (P = .970), the proportion of pathologic depth of invasion (P = .860), and lymph node metastasis (P = .206).
Operative outcomes and postoperative recovery
We visually observed the condition of the esophagus rings in both groups after the anastomosis was completed. The esophagus ring was fuller and wider at its narrowest part by ligating and reinforcing the esophageal ring with the bronchus forceps (Fig. 5). The summaries of operative outcomes and postoperative recovery are shown in Table 2. There was no significant difference in the aspect of the proportion of intraoperative bleeding (P = .835), the time of first postoperative meal (P = .744), the time of first anal exhaust (P = .222), and postoperative length of hospital stay (P = .439). However, compared with the Conventional Surgery Group, the narrowest part of the esophageal ring was wider in the Bronchus Forceps Ligation Group (P < .001). In terms of the operative time, reinforcing the esophageal ring with two ligations using bronchus forceps could almost always be done in less than 5 minutes.
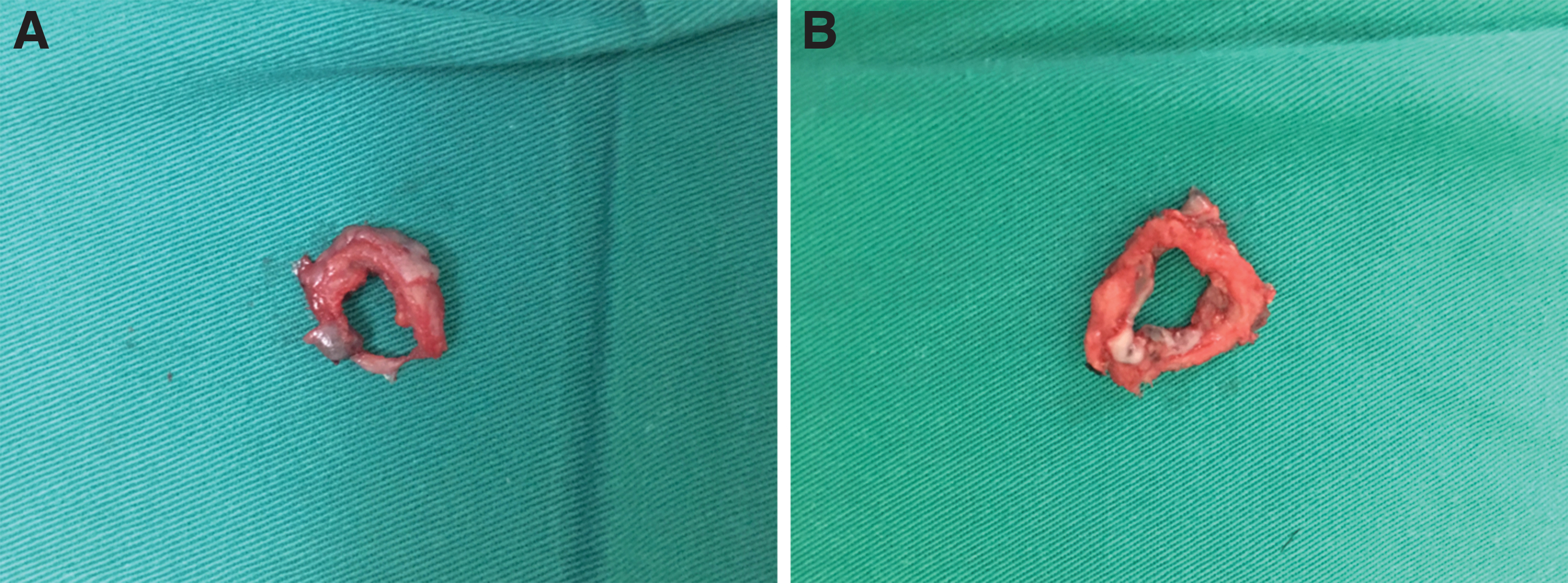
Direct visual inspection of the esophagus ring.
Operative Outcomes and Postoperative Recovery Compared Between Conventional Surgery Group and Bronchus Forceps Ligation Group
Postoperative complications
The statistical analysis of postoperative complications is summarized in Table 3. It shows that the incidence of anastomotic leakage in the Bronchus Forceps Ligation Group is lower than that in the Conventional Surgery Group (P = .041). Also, there was no significant difference in abdominal infection (P = .596), anastomotic bleeding (P = 1.000), anastomotic stenosis (P = 1.000), postoperative obstruction (P = 1.000), and pulmonary complication (P = .729).
Postoperative Complication Compared Between Conventional Surgery Group and Bronchus Forceps Ligation Group
Discussion
In this study, with ligating and reinforcing the esophageal ring by bronchus forceps, the esophageal ring is fuller and wider at its narrowest part. Besides, it reduces the incidence of anastomotic leakage. Moreover, although the novel technique adds additional operative time, almost all can be done in less than 5 minutes.
After LPG or LTG, many difficulties of esophagogastroanastomosis and EJ anastomosis still exist. It is very difficult to place the anvil, especially in patients with gastric tumor invading the lower esophagus, obesity, or large anteroposterior diameters. Up to now, there are various methods to place the anvil into the esophagus, mainly including hand-sewn purse-string suturing, 13 anvil insertion using a purse-string instrument, 14 anvil insertion with a suture and needle through esophagostomy, 15 the lift-up method, 16 and the use of an oral anvil insertion system (OrVil™). 17 Recently, laparoscopic placement of the anvil into the esophagus stump using a conventional PSI and the four stay-sutures method has been reported.9,18 There is no best way to insert the anvil into esophagus, and the purse-string devices continues to play an important role in extracorporeal anastomosis. Besides, extracorporeal EJ anastomosis with a circular stapler is still a generally accepted approach for LTG, 19 which allows a higher anastomotic rate in patients with gastroesophageal junction or epigastric tumors invading the esophagus. 20 However, due to the difficulty of the extracorporeal exposure, the anvil is often out of place. In addition, small tears often occur in the esophageal serosa layer around the anvil due to excessive stretching of the esophageal stump. Therefore, we sometimes see a weak or even discontinuous esophageal ring after anastomosis with a circular stapler is completed, greatly increasing the risk of postoperative anastomotic leakage. Also, the direct visual inspection of the esophageal ring after the circular stapler was fired is an important method for predicting anastomotic leakage. 21 As one of the serious complications after proximal or total gastrectomy, anastomotic leakage can lead to death in severe cases. 22 It is currently reported that EJ anastomotic leakage incidence is 2.6%–14.6%. 23 Increased tension and limited vascular supply are two important risk factors of anastomotic leakage, especially in patients whose esophagus lacks the serosa. 24
In this regard, to let esophagus ring fuller and wider at its narrowest part, we creatively use the bronchus forceps to reinforce the esophageal ring on the anvil of 25 mm circular stapler with two perpendicular ligations on the lower edge of the purse-string suture, after placing the anvil in the esophageal stump with a conventional PSI. Besides, this technique reduces the incidence of anastomotic leakage. Furthermore, being widely used during traditional surgery, the conventional PSI and bronchus forceps are familiar to surgeons and available in almost every institution. Therefore, this useful technique has the advantage to popularize easily. The weaknesses of the study lie in the retrospective nature and small number of patients. Further studies will include more patients and studies of short-term and long-term surgical outcome.
Conclusion
For extracorporeal anastomosis using a circular stapler in proximal gastrectomy or total gastrectomy, it is necessary to ligate and reinforce the esophageal ring on the anvil with the bronchus forceps, after placing the anvil into the esophagus with a conventional PSI.
The Source of a Study
The General Surgery, the Affiliated Hospital of Southwest Medical University.
Footnotes
Authors' Contributions
R.Y. and Y.Y. are members of our team who have made a direct and substantial contribution to the study by conceiving and designing the study, collecting and analyzing the data, and writing this article. Q.Y. is leader of our team, who has been involved in the design and revision of this study. X.C. is a member of our team, who has been involved in the related operations and collection of data.
Acknowledgments
We would like to thank the Affiliated Hospital of Southwest Medical University for its support to our research work.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.