
Abstract
Background:
Patients with hereditary diffuse gastric cancer (HDGC) and germline mutations in the E-cadherin gene, CDH1, have a very high cumulative lifetime risk of developing diffuse gastric cancer. In these patients, it is formally recommended to perform a prophylactic total gastrectomy (PTG).
Materials and Methods:
We analyzed the course of patients with HDGC who have undergone PTG in our institution. Pedigree analysis, preoperative screening results, operative course, postoperative data, and complete stomach pathologic examination were performed in all patients.
Results:
Seven patients with confirmed CDH1 mutation underwent PTG, five were women, and average age was 27 years (range 17–42). Signet ring cell carcinoma was found in 1 patient in the preoperative surveillance endoscopic biopsies. Laparoscopic PTG was performed in all patients. There were two complications, an intestinal obstruction that required reintervention and an asymptomatic esophagojejunal anastomosis leak that resolved with conservative treatment. In all gastrectomy specimens, intramucosal signet ring cell carcinoma foci limited to the lamina propria were found (range 1–31), 83.5% were in the body-fundus region. The mean follow-up was 28.5 months (range 8–72). The mean weight loss was 9% (range 2–18). Postoperative symptoms associated with Dumping syndrome were the most frequent. All the patients reported of being very satisfied with the procedure and of having a better quality of life than expected before the procedure.
Conclusion:
Laparoscopic PTG is an excellent resource to prevent the development of advanced diffuse gastric cancer (DGC) in patients with HDGC with CDH1 mutation. The procedure was well tolerated with a high satisfaction rate and very good functional results. It should be considered in these patients due to the high risk of developing advanced DGC and the lack of effective and reliable surveillance studies.
Introduction
Gastric cancer is the third leading cause of cancer death worldwide, with approximately 1 million new cases and nearly 780,000 deaths per year. 1 Despite the fact that the majority of gastric cancer cases are sporadic, about 10% demonstrate some type of familial aggregation.2,3 One to three percent of gastric cancers correspond to hereditary gastric cancer syndromes. Hereditary diffuse gastric cancer (HDGC) is included in this syndrome. It was first described in 1964 in three Maori families from New Zealand. 4 In 1998, Guilford et al. described the germinal mutation of the CDH1 tumor suppressor gene in charge of encoding the protein E-cadherin, a transmembrane glycoprotein that mediates cell adhesion and differentiation of the epithelium during its growth.5,6
The germline mutation in the CDH1 gene and the loss of E-cadherin is expressed clinically by increasing the risk of developing diffuse gastric cancer (DGC) and lobular breast cancer (LBC).7,8 In carriers with CDH1 mutation, the cumulative risk in men at age 80 of developing DGC is 70%. In women, it is 56% for DGC and 42% for developing LBC. 9 Hereditary gastric cancer syndromes are characterized by their early onset, generally before the age of 45. In HDGC, it has been reported that the average age for the onset of symptoms is 38 years. 10 The International Gastric Cancer Linkage Consortium (IGCLC) has established, for more than a decade, the management guidelines for families with HDGC and the criteria to identify families with CDH1 mutations.11–13 In the year 2020, these criteria were reviewed and updated 14 (Fig. 1).
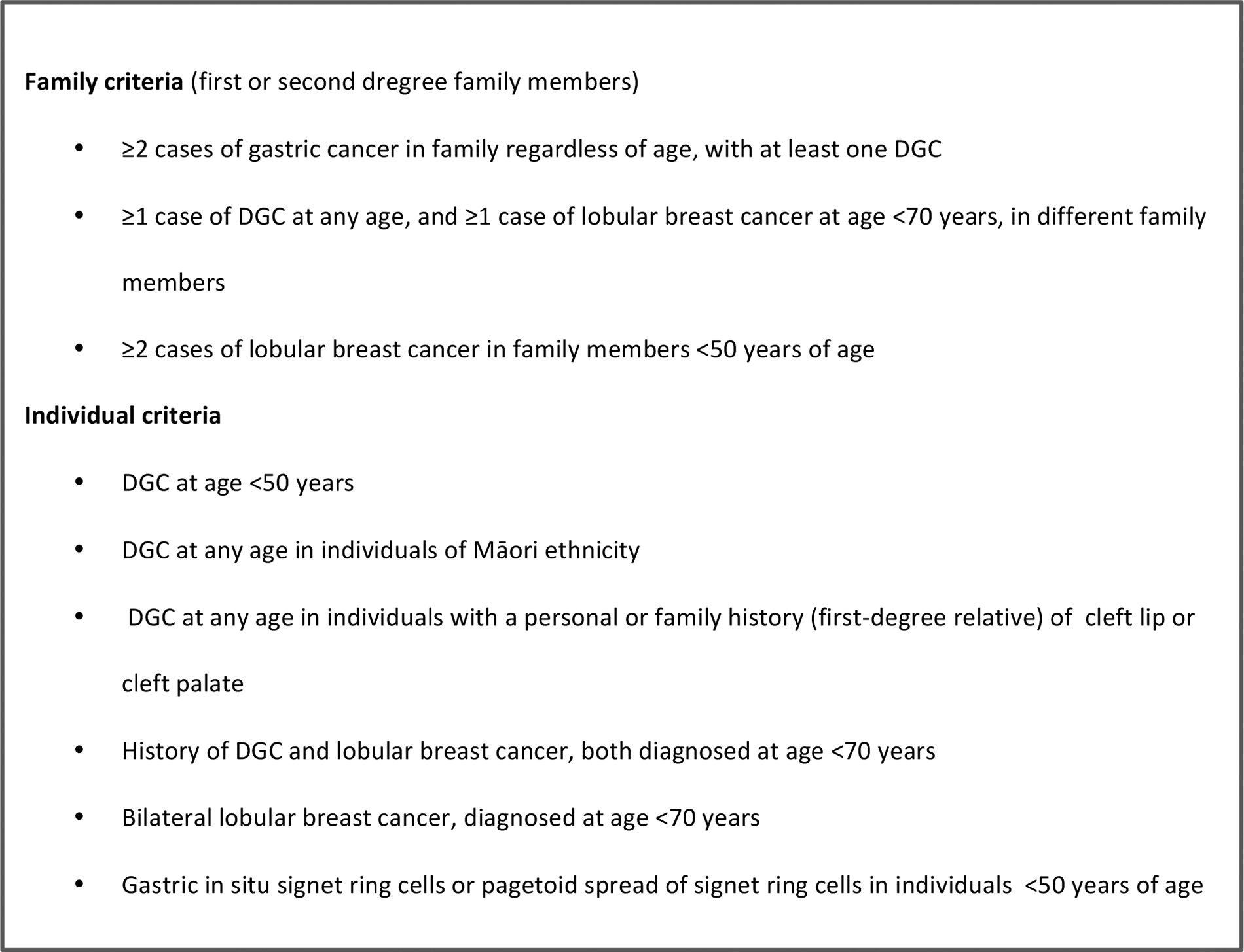
2020 HDGC genetic testing criteria. HDGC, hereditary diffuse gastric cancer.
Endoscopic surveillance at an early age should be a cornerstone in the prevention of the development of DGC in these patients, given the high penetrance and aggressive nature of HDGC. Random biopsies in all the areas of the stomach looking for a possible nonvisible foci of early stage DGC should be performed in these individuals.
However, most series have shown that endoscopic surveillance are not effective enough to identify microscopic foci (T1a) of signet ring cells carcinoma (SRCC) in HDGC and detect the disease at an early stage.15–39 Negative biopsy results do not mean that patients are free of SRCC foci and that they are not at risk of developing advanced DGC. Almost the majority of series have described that 80%–100% of the patients who underwent a prophylactic total gastrectomy (PTG) had microscopic focus (T1a) of SRCC in their final pathology despite having a normal preoperative endoscopy.15–39
Given the lack of effective and reliable surveillance methods and the high risk of developing advanced DGC, it is strongly recommended to perform a PTG in patients with HDGC at an early age. 14 The best moment or opportunity for a PTG depends on each patient, being recommended between the ages of 20 and 30, and in those families with a history of early DGC onset in young patients, it even requires the decision to perform a PTG in patients younger than 20 years.13,36 Patients planning to have a PTG require a multidisciplinary team to address the preparation for the procedure and understanding of the disease.
Our objective is to report the experience and results of PTG in our series of patients with HDGC and CDH1 mutation. Worldwide PTG series have been reported in North America (Canada and USA), Europe, and New Zealand.15–39 To our knowledge, this is the first series of patients with PTG in HDGC and CDH1 mutation in Latin America.
Materials and Methods
We performed a retrospective review of prospectively collected data from patients with HDGC and a positive genetic test for the germline mutation of the CDH1 gene that underwent a PTG from January 2014 to December 2019. Pedigree analysis, preoperative screening results, operative course, pathological specimen analysis, and postoperative data, including complications and symptoms questionnaire, were collected and reviewed. The study was presented and approved by the institutional review board.
Preoperative workup
In all patients, at least one preoperative endoscopy was performed according to the IGCLC guidelines for HDGC. 12 Precise and detailed inspection of the entire gastric mucosa was performed, with biopsy of suspicious focal lesions, if any, and six random biopsies from each of the following regions: cardia, fundus, body, transition zone (between body and antrum) and antrum. All patients were counseled by a specialized multidisciplinary group of geneticists, esophagogastric surgeons, oncologists, gastroenterologists, nutritionists, and psychologists. In all cases, the risk of developing DGC was explained, and in women, equally for LBC.
Surgery
In all patients, we performed a laparoscopic approach. We performed a total gastrectomy with Roux-en-Y reconstruction with a D1 lymphadenectomy in patients with negative biopsy in the screening endoscopy and a D2 lymphadenectomy in the patients with positive biopsy. The omentum was partially extracted up to 5 cm below the gastroepiploic arch. The duodenum was transected at the superior part of the duodenum and the esophagus was transected at least 2 cm above the esophagogastric junction.
Intraoperative frozen sections of the proximal and distal margin were evaluated by a pathologist for esophageal squamous and duodenal mucosa, respectively, to confirm complete resection of gastric mucosa. We created a 70 cm Roux limb, performing a stapled or manual side-to-side (functional end-to-side) jejunojejunostomy. Depending on surgeon's choice, the esophagojejunal anastomosis was performed manually or stapled, side-to-side (45 mm) or circular end-to-side (25 mm).
Pathology
The surgical specimens were handled following the recommendations of the IGCLC. 12 Fresh gastrectomy specimens were opened along the greater curve (after painting the margins, dissection of the omentum and retrieval of lymph nodes) and pinned onto a cork board with overnight fixation in buffered formalin. A life size specimen photo was used as a template to identify the exact location of the tissue blocks (a schematic map was used for that purpose). Sections of the margins were taken and labeled and the remainder of the stomach was sectioned completely (each section 2 cm long and 0.3–0.5 cm thick) and blocked (paraffin embedded). This results in between 120 and 160 blocks per stomach.
The histological examination confirmed invasive (intramucosal) carcinoma(s) and/or precursor lesions such as in situ carcinoma and pagetoid spread. Its anatomical site (cardia, fundus, body, transitional zone, and antrum) and its location (greater curvature, lesser curvature, anterior wall, posterior wall, and circumferential) were marked on the map of the stomach.
Postoperative workout
Postoperative clinical and surgical results were analyzed. Complications were classified according to the Dindo-Clavien classification. 40 Patients were followed at least at 2 weeks, 1, 2, and 6 months, and 1 year postoperative. Symptoms comprehensive questionnaire, UGI, and endoscopic examination were done in all patients. Each patient received a questionnaire to assess various aspects of their symptoms and were asked to score the frequency from 0 to 4: 0 = never, 1 = once a month, 2 = once a week, 3 = once a day, and 4 = several times a day, and the severity on a 10-point visual analog scale with 1 being “mild” and 10 as “most severe.” Their perception and satisfaction of the procedure was also evaluated. Weight loss was recorded.
We add a breast magnetic resonance imaging (MRI) to the yearly breast surveillance for all female patients with at least 30 years of age or above.
Results
Seven patients with HDGC criteria, with a positive genetic test for the germline mutation of the CDH1 gene, performed a laparoscopic PTG. All the patients belonged to the same family. The index case in this family was a 33-year-old woman who underwent a total gastrectomy (T3 N3b M1) for DGC. He died 3 months after surgery due to disease progression. Her mother and uncle (his mother's brother) had died from DGC at the ages of 60 and 67. Upon suspicion for HDGC criteria, their kindred decided to be tested for CDH1 mutation. In total, 11 relatives were found to carry a nonsynonymous germline sequence in the CDH1 gene, a nonsense pathogenic variant, c.1531C>T (p.Gln511*), in exon 10.
Seven patients decided to accept a PTG. Two patients decided to follow endoscopic surveillance. In the first one, during her first year of endoscopic surveillance, they found a small ulcer with a positive biopsy for SRCC. A total gastrectomy was performed at another institution (T1b N0). She is still alive and disease free. The second patient, in the second year of surveillance, developed an intestinal obstruction with ascites and peritoneal carcinomatosis with biopsy for DGC. He died 3 months later. The remaining 2 patients were 10 years old, so clinical surveillance was decided.
Of the 7 patients who decided to undergo PTG, 5 were women. The mean age was 27 years (range 17–43). Only in 1 patient (14%) preoperative endoscopic biopsies reported SRCC. Two patients were 17 years old (Fig. 2 and Table 1).
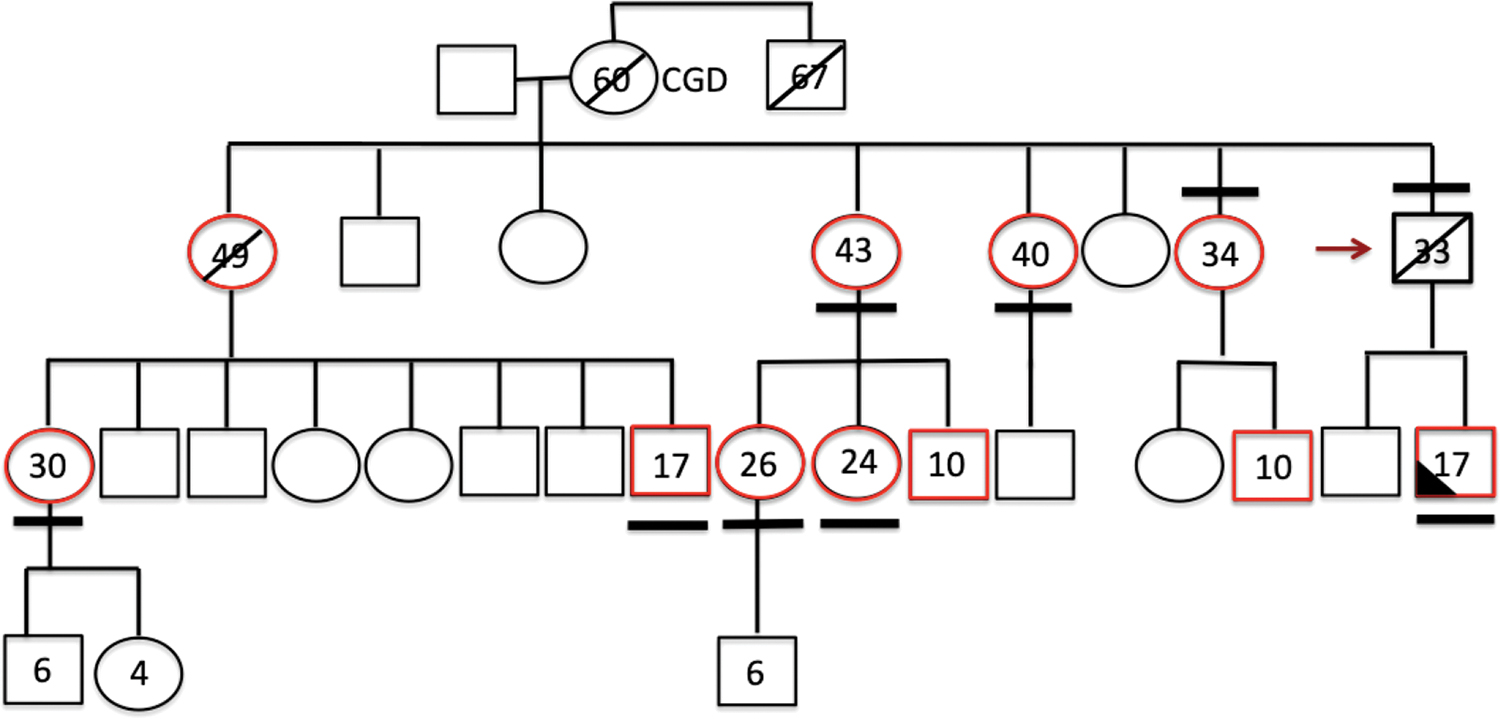
Family pedigree. Circle: female. Red arrow: index case. In red: patients who test positive for germline mutation of the CDH1 gene. Cross line: DGC deceased patients. Line above: therapeutic total gastrectomy. Line under: laparoscopic prophylactic total gastrectomy. Black triangle: positive biopsy for SRCC in preoperative endoscopy. DGC, diffuse gastric cancer; SRCC, signet ring cells carcinoma. Color images are available online.
Results
EGD, esophagogastroduodenoscopy; E-J, esophagojejunal; I.O, intestinal obstruction; Lap, laparoscopic; PTG, prophylactic total gastrectomy; SRCC, signet ring cells carcinoma.
Postoperative results
All patients were approached laparoscopically and there was no conversion to open surgery. The mean operative time was 298 minutes (range 227–338). Two patients had postoperative complications. One patient presented an asymptomatic leak of the esophagojejunal anastomosis found during the radiologic water-soluble swallow study at the 7th postoperative day (Dindo-Clavien II). She was managed with conservative treatment and she received enteral nutrition through the nasoenteral feeding tube. She was discharged with soft diet in the 28th postoperative day. One month after discharge, she referred a mild dysphagia and required an endoscopic dilation due to a mild stenosis of the esophagojejunal anastomosis.
The second patient presented an intestinal obstruction in the 5th postoperative day. He required intervention and revision of the enteroenteric anastomosis with good postoperative evolution (Dindo-Clavien IIIb). He was discharged on postoperative day 15. The rest of the patients had a radiologic water-soluble swallow study and started a liquid diet on the 7th postoperative day. They were discharged with a soft diet on the 9th postoperative day. The median length of stay was 9 days (range 9–28) (Table 1).
Mean follow-up was 28.3 months (range 10–72). The symptoms and results described after the symptoms comprehensive questionnaire were:
(1) 100% of the patients presented symptoms compatible with Dumping syndrome, almost always represented by sweating, postprandial chills, in cases accompanied by abdominal colic, and to a lesser extent, by diarrhea. They were always related to significant volume or rich in carbohydrates intakes. The median frequency was 2 (range 1–2) and intensity 7 (range 6–8). (2) Four (57%) patients reported feeling of postprandial abdominal distension with a median frequency of 2 (range 1–3) and intensity of 4 (range 3–6). (3) Five (71%) patients reported early fullness in meals with a median frequency of 2 and intensity of 4 (range 3–6). (4) Five (71%) patients reported not being able to eat the same amount of food as before surgery and the median number of intakes or meals per day was 5 (range 4–7). The mean weight loss was 9% (range 3–18).
All the patients reported a better quality of life than expected before the operation, and they were all very satisfied with the procedure and the results. Five of our patients are women. In the family pedigree, there was only one history of ductal breast cancer in an aunt who received a total mastectomy with a disease-free survival of 35 years. They were advised on the possibility of receiving prophylactic mastectomies, but all opted for annual clinical and imaging surveillance. Three of them are older than 30 years and are undergoing annual surveillance with mammography and breast MRI.
Pathology
In all gastrectomy specimens, intramucosal SRCC foci limited to the lamina propria were found. The mean of SRCC foci was 11 (range 1–31). In all patients, the SRCC foci were in the body-fundus region, and in 1 patient, they were also found in the antrum and prepyloric. In 5 patients, multiple foci of carcinoma in situ also coexisted in the corporeal region. The distal and proximal edges had free margins with gastric mucosa in all the resected specimens. The mean number of lymph nodes resected was 20 (range 8–33). Pathological staging in all patients was pT1a pN0 (Table 2).
Gastrectomy Specimens Pathology
B, body; F, fundus; SRCC, signet ring cell carcinoma.
Discussion
More than 20 years have passed since the initial description of the germline mutation of the CDH1 gene in patients with HDGC. 5 In 2001, Huntsman et al. described, for the first time, the PTG in a series of patients with HDGC and a germline mutation of the CDH1 gene. 15 Since then, about 25 series with at least 2 or more patients with PTG have been presented. Most of these series have less than a dozen patients, showing the low prevalence of this hereditary syndrome. These series have been described in North America (USA and Canada) and Europe, as well as in New Zealand.15–39,41
Our study presents a series of 7 patients corresponding to an Argentine family with a history of HDGC and a germline mutation of the CDH1 gene. In few Latin American countries, it has been described germline mutations of the CDH1 gene associated with patients with HDGC.10,42–44 Norero et al. in a series of Chilean patients with a history of HDGC and germline mutation of the CDH1 gene has described 1 case of PTG in a female patient. 44 To our knowledge, this is the first series of PTG cases in patients with HDGC in Latin America.
The heterozygous pathogenic mutation in this family was c.1531C>T (p.Gln511 *) in exon 10 of the CDH1 gene. This mutation was recently described for the first time in a Chilean family. 44 Interestingly, our family lives in a border province of our neighboring country Chile, which is very likely that these two families have some common ancestor and explain the same germline mutation of the CDH1 gene.
The index case in our family was a 33-year-old patient who died 3 months after being operated for a DGC. The age of presentation of this patient is slightly earlier than the average of 38 years described for patients with HDGC. 10 In our series, 2 of our patients were <20 years, both had 17 years at the moment of the operation. The first patient, after knowing that he was positive for SRCC in his first screening endoscopic biopsies and after consulting with his parents, decided to accept the PTG. The second patient, having evidenced the death of his mother a few months before due to an advanced DGC, decided to do a PTG, consulting also previously with his father. Both patients had full growth and the psychological and intellectual maturity to perform the process.
The IGCLC recommends performing GTP between the ages of 20 and 30, however, in those patients with relatives with early presentation, the age for performing PTG can even be younger than 18 years. 14 Wickremeratne et al., who performed a total gastrectomy, presented a review of the literature for patients younger than 20 years old, asymptomatic, and carriers of the germline CDH1 gene mutation. He described about 11 patients, including two 16-year-old patients and one 15-year-old patient. 45 Gullo et al. described a PTG in the youngest patient in the literature, a 14-year-old patient with a family member with an early debut of DGC at the age of 18 years. 36
We believe, that according to each particular case and taking into account the presentation of each family, it is possible to perform a PTG in young patients, younger than the age of 20 years. In these teenage patients, the multidisciplinary approach is not only necessary to evaluate the growth development but also the intellectual and emotional development.
In our family, only 1 patient (14%) had a surveillance endoscopic biopsy positive for SRCC. The literature shows that patients with PTG and positive results for SRCC foci in their gastrectomy specimens had only 28% positive SRCC biopsies in their surveillance endoscopies. 46 The Cambridge Group has described two prospective studies where they have obtained higher results for positive biopsies in the surveillance endoscopies than the rest of the series with PTG and HDGC. They described 61.1% and 63.6% positive biopsies for SRCC in patients undergoing surveillance endoscopy.47,48 The IGCLC has recommended the use of the Cambridge protocol for endoscopic surveillance. However, even if the other groups could be able to reproduce the results of these studies, which mostly no one did, almost 40% of the gastric biopsies of HDGC patients will be false negatives.
This is why we do not believe that endoscopic surveillance in patients with HDGC is currently safe and effective enough to detect diffuse early gastric cancer, and we agree with the recommendations of the IGCLC, and we advise our patients with HDGC to have a PTG.
In all of our patients, the approach was laparoscopic. For the surgical groups with previous experience in laparoscopic gastric cancer surgery, we believe that the laparoscopic approach for this type of patient is ideal. We believe that being able to offer these asymptomatic patients a procedure with less postoperative pain, earlier return to work and social activity, and with a better aesthetic result can help the decision and smooth the initial concerns of having to undergo a PTG. HDGC patients have a stomach without tumor and are generally young adults, this makes the situation favorable to carry out the surgery by minimally invasive approach. Few series have described the laparoscopic approach for PTG, and if they did, the majority described it in few patients.25,26,34,35,38,49 However, there is a trend in new series to increasingly use this approach.
All of our patients with negative surveillance biopsies received a D1 lymphadenectomy. In 1 patient with positive biopsy for SRCC in his surveillance endoscopy, we decided to do a D2 lymphadenectomy. In all cases, the resected nodes were negative. The vast majority of the series that reported the technique of lymph node dissection performed a D1 dissection as recommended by the IGCLC. Few authors have described that they have performed both D1 and D2 lymph node dissections or exclusively D2 in their series.20,21,34,35
We know that the postoperative gastrectomy specimens in almost all the literature studies have reported small intramucosal foci of CAS and are concentrated in the lamina propria (T1a). 46 However, Rocha et al. in a review of the literature has found at least 5 cases of total gastrectomy specimens from asymptomatic HDGC patients with invasive carcinoma beyond the lamina propria, T1b to T3. 46 Rocha et al. also described that a positive association existed between the yield from endoscopy and the number and size of intramucosal carcinoma in PTG specimens. 46 More recently, Vos et al. described 2 more cases of T1b. 35
An important datum from the published series is that no lymph node metastases were found in all the lymph nodes analyzed.15–39,41 This matches with recent studies that have shown that in early gastric adenocarcinoma (EGC) with CAS, lymph node metastases are rarely found. 50 Park et al. reported that the incidence of lymphatic metastases was 7.9% for EGC with CAS, 6% for submucosal infiltration, and 1.9% for intramucosal tumors. 51 Wang et al., in turn, demonstrated that the frequency of lymph node metastases in EGC with CAS was 3.8%, but in those tumors smaller than 2 cm and without lymphatic invasion, the frequency of metastasis was 0%. 52 Kim et al. described that in intramucosal tumors with CAS of <1.5 cm without lymphovascular invasion, the frequency of lymph node metastases was 0%, as did Lee et al. for those smaller than 2 cm and without lymphovascular invasion.53,54
Therefore, taking into account that we know that practically all the gastrectomy specimens in patients with HDGC have intramucosal microscopic foci of CAS limited to the lamina propria (T1a), associating a D1 lymph node dissection should be safe and effective enough.
However, as we said, positive endoscopic biopsy for SRCC previous to PTG is associated with bigger size and number of foci. 46 Also, most of the few patients described with invasive carcinoma beyond the lamina propria had previous positive endoscopic biopsy for SRCC.29,33 Taking this into account, we feel safer doing a D2 lymphadenectomy in a PTG when a preoperative or surveillance endoscopic biopsy for SRCC is positive, foreseeing that we may have a small chance of a more invasive carcinoma and leading this to a higher rate of lymphatic node metastasis.
In our series, only 2 patients had complications before and after 30 days postoperatively. We had an esophagojejunal anastomosis leak that resolved with conservative management with subsequent mild stenosis of the anastomosis and endoscopic resolution, and an intestinal obstruction that required reoperation. We know that open or laparoscopic total gastrectomy is a challenging and complex procedure and that it is not free of complications.
Vos et al. described 101 PTG, by far the biggest series in the literature, 43 of them by minimally invasive approach. 35 In this series, 48 (48%) patients had complications, 28 (28%) within 30 days of surgery. Thirty-four (34%) were D-C III or major complications. Among the early complications, the most frequent were 6 (6%) esophagojejunal anastomosis leaks, in which 3 required reintervention, 8 (8%) pulmonary complications, including 2 pleural effusion and 2 pneumothorax, 2 (2%) hemorrhage requiring surgery, and 1 (1%) duodenal stump leak. Twelve (12%) patients were readmitted within 30 days of surgery, and 3 (3%) required a percutaneous endoscopic feeding tube. Among the late complications, it is important to mention that 15 (15%) were esophagojejunal anastomosis stenosis, which required dilation. One patient died.
Kaura et al. presented 52 patients, 6 were approached laparoscopically. 38 Twenty-three (46%) patients presented complications, and 10 (19.2%) presented the complication within 30 days of surgery. He reported 4 (9%) major complications: 2 (3.8%) anastomosis leaks, one pleural effusion, and one pulmonary thromboembolism. After 30 days of surgery, there were 12 (23%) patients with anastomotic stenosis, 1 (4%) patient with bile reflux, and 2 (8%) patients with obstruction of the digestive tract, one duodenal and another at the level of the enteroenteric anastomosis.
Three more studies with patients with laparoscopic PTG, Haverkamp et al., Pantelis et al., and Hackenson et al. showed global complications in 5 of 11 (45%) patients, 3 of 12 (25%) patients, and 2 of 6 (33%) patients, respectively.26,32,34 As we have seen, PTG, even in high-volume centers and/or performed by specialists in gastric surgery, continues to have a high rate of complications.
All (100%) of the resected gastrectomy specimens in our series had intramucosal SRCC foci limited to the lamina propria (T1a), and 71% had carcinoma in situ foci. The number of foci ranged from 1 to 31, regardless of the age and gender of the patients. These findings correlate and are consistent with reports from previous studies.18,55 Rocha et al. described that 87.9% of the PTG showed SRCC foci. However, if you exclude those series that had not used the protocol suggested by the IGCLC, SRCC foci were found in 95.3% of the PTG specimens. Furthermore, he observed that in 48.5% of the PTG carcinoma in situ foci were also found. 46
In our series, the distribution of SRCC foci had a clear body-fundus trend. Many authors in recent years have reported a proximal distribution trend that is opposite to what was described in the first reports in the series of Maori families in New Zealand.21,47,56,57 In this series, the foci were mostly in the antral-body transition zone and in the distal stomach.18,58 It is unknown what are the factors for these topographic differences, but genetic susceptibility and environmental agents have been suggested as probable causes.58,59
Another concern to be taken into account in families with HDGC is the probable development of a LBC. The estimated risk of developing LBC varies between 39% and 55% and has remained consistent among the studies published, so the option of a prophylactic mastectomy (PM) in these patients should be considered strongly. 60 Foci of atypical lobular hyperplasia, lobular carcinoma in situ (LCIS), and foci of invasive LBC have been described in PM of CDH1 germline mutation carriers. 29
Few data have been described about breast screening and PM after PTG in PTG series. Kluijt et al. described that of the 17 female patients in their series, only one had a history of mastectomy for LBC. This patient underwent a PM of the remaining breast after the PTG resulting in multiple foci of LCIS and one foci of invasive LBC. The patient's sister also agreed a bilateral PM with the result of multiple foci of LCIS. 29 Bardram et al. described no history of breast disease in their female patients. Two patients underwent a bilateral PM with the result in one of them of invasive LBC and multiple foci of LCIS, and in the other of an intraductal papilloma, with ductal hyperplasia and apocrine metaplasia without findings of malignant pathology. 30
Of our 5 female patients, none had developed breast malignancies during the follow-up. Mostly, their decision not to undergo a PM for now is their lack of history for LBC in their family and to have a recent surgical procedure. However, they have stated that they do not rule out the possibility of a bilateral PM and are receptive to carrying it out in the near future. Three of them are older than 30 years and are undergoing follow-up with annual breast MRI and mammography.
Quality of life after gastrectomy in patients with HDGC is a very important issue since these patients, unlike the usual patients with advanced DGC, are expected to have a very long overall survival. The quantity and quality of food intake, weight loss, digestive symptoms, and quality of life are the most relevant issues in the follow-up after total gastrectomy.61,62
Strong et al. described in their PTG series that more than 65% of the patients reported not being able to eat the same amount of food as before the operation, average intake of 5 (range 3–8) daily meals and meals of smaller volume. In turn, 95% of the patients reported at least one symptom associated with Dumping syndrome. Forty percent reported better results and 45% the same results after PTG than expected. The mean weight loss after PTG at 16 months was 15%. 63 Van der Kaaij et al. described that their patients reported symptoms compatible with reflux and dumping syndrome in 60% and 44%, respectively. The mean weight loss at 1 and 2 years were 15% and 10%, respectively. After the first postoperative year, 79% of the patients had returned to their usual work tasks. 41 Kaura et al. reported that the satisfaction index after PTG was positive in 88% of the patients (79% very satisfied and 9% satisfied). 38
Although we did not measure formally validated quality-of-life parameters, our questionnaire for postoperative symptoms showed that symptoms consistent with dumping syndrome were present in all of our patients. However, these were mentioned infrequently, once a week or less, and only when they ingested larger portions than recommended, with fast intake and/or with foods rich in carbohydrates. However, when these symptoms occurred, they were noted as very intense. The majority decreased the portion and increased the number of daily meals.
All the patients stated that they were very satisfied with the surgery and that they had a better quality of life after PTG than was expected before the procedure. Undoubtedly, in our series, acceptance of the procedure was very good, strengthening the decision to continue implementing PTG as a primary option in patients with HDGC.
Conclusion
PTG is an excellent resource to prevent the development of advanced DGC in patients with HDGC and a germline mutation of the CDH1 gene. In our series, it was a well-tolerated procedure, with an acceptable complication rate, high satisfaction rate, and good functional results. PTG should be considered in these patients due to the high risk of developing DGC and the lack of effective and reliable surveillance studies.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.