
Abstract
Background:
Laparoscopic pancreaticoduodenectomy (LPD) is one of the most technically challenging operations of minimally invasive surgery. We aimed to analyze the learning curve of a single surgeon who conducted 115 LPDs at a single center.
Materials and Methods:
From August 2015 to August 2020, 115 patients underwent LPD. Patient characteristics and perioperative variables were retrospectively collected and analyzed. Cumulative summation (CUSUM) and risk-adjusted cumulative summation (RA-CUSUM) analyses were used to evaluate the LPD learning curve. All variables were compared after dividing the learning curve phases.
Results:
After 74 cases, operative time improved based on the CUSUM analysis of the operation time. From the RA-CUSUM analysis, three distinct phases of the learning curve were identified (phase I: 1–42 cases, phase II: 43–73 cases, and phase III: 74–115 cases). The mean operative time was significantly lower in phase III compared with that in phases I and II (348.5 minutes versus 444.6 minutes and 439.9 minutes, P < .001 and P < .001, respectively). The rate of estimated blood loss >500 mL was significantly decreased among the three phases (P = .017). The conversion rate significantly decreased from 11.9% in phase I to 6.5% in phase II to 0% in phase III (P = .023). The rates of overall complication (Clavien–Dindo >IIIA), postoperative pancreatic fistula, and postpancreatectomy hemorrhage were significantly decreased as phases progressed. Postoperative hospital stay, 30-day mortality, and 30-day readmission did not significantly differ among phases.
Conclusions:
According to learning curve analyses, the LPD failure rate plateaued after 42 cases and stabilized after 73 cases.
Introduction
Laparoscopy is a technique that has gained widespread acceptance as a general surgical procedure because of shorter hospital stays and earlier recovery compared with open surgery. However, total laparoscopic pancreaticoduodenectomy (LPD) is one of the most difficult and high-risk abdominal operations. It is performed only in high-volume centers by a few highly experienced surgeons because of the extensivity of dissection and reconstruction of the digestive tract. Gagner and Pomp first reported LPD in 1994, 1 and a few studies suggested its technical feasibility and safety in terms of perioperative outcomes involving intraoperative blood loss, postoperative morbidity, and postoperative hospital stay.2–4 Consequently, with newer techniques and the increasing experience of surgeons, LPD is performed more often in recent years.5,6
However, a recent randomized controlled trial (LEOPARD-2) was halted because LPD, although performed by well-trained surgeons, was associated with more complication-related deaths than open pancreaticoduodenectomy (PD) in centers with 20 or more LPDs. Therefore, they concluded that experience, learning curve, and annual volume affected the findings. 7 To become technically competent in this operation, surgeons require a relatively long training period.3,8,9 For LPD to be widely applied in routine practice, studies on the learning curve are required.
This study analyzed the learning curve for LPD based on cumulative summation (CUSUM) and risk-adjusted CUSUM (RA-CUSUM) analyses using 115 LPDs performed by a single surgeon and compared clinicopathological and perioperative outcomes between groups according to the learning curve.
Materials and Methods
Patients
Data were retrospectively collected for 115 patients who underwent LPD by a single surgeon at the Hallym Sacred Hospital in Anyang, Korea, from August 2015 to August 2020. Demographic data (age, gender, body mass index, and the American Society of Anesthesiologists [ASA] classification), operative time, estimated blood loss, postoperative length of hospital stay, morbidity rate, mortality rate, and pathological results (pathological diagnosis, tumor size, harvested lymph node number, and R status) were reviewed.
Operative time was measured as the duration from the first incision to final closure. Open conversion was defined as laparotomy at any time during LPD, except during the extraction of the resected specimen. The weight of the swabs plus the blood removed during the operation was used to calculate the estimated blood loss. Postoperative complications were described according to the Clavien–Dindo classification. 10 Postoperative pancreatic fistula (POPF), postpancreatic hemorrhage (PPH), and delayed gastric emptying (DGE) were defined per the International Study of Pancreatic Surgery definitions.11,12 The institutional review board at our hospital approved this study (Hallym 2020-12-010).
Operative technique
The procedure is performed using a total of 5 trocars arranged in a semicircle in the lower and lateral aspects of the abdomen while the patient is in the supine position. Occasionally, for more adequate exposure, the falciform and lateral sections of the liver are sutured using 2-0 straight needle Prolene (Ethicon™; Johnson and Johnson, New Jersey). Owing to pneumoperitoneum, a diagnostic laparoscopy is performed by inspecting all visible peritoneal and visceral surface, especially liver surface. By using ultrasonic shears, the lesser sac is widely exposed, and then the gastrocolic trunk is dissected and divided. The gastroduodenal and right gastric arteries are ligated, clipped, and divided. The first portion of the duodenum is transected with a linear stapler 2–3 cm distal to the pylorus. The common hepatic artery and the gastroduodenal artery are isolated. The bile duct at the cystic duct insertion level is dissected, ligated superiorly, and divided. A Kocher maneuver is performed after the hepatic flexure of the colon is mobilized inferiorly. The portal vein is located at the superior border of the pancreatic neck, and the superior mesenteric vein at the inferior border. A tunnel is dissected behind the pancreatic neck, anterior to the superior mesenteric vein and portal vein. The pancreatic neck parenchyma is transected by ultrasonic shears, and the pancreatic duct is divided sharply with scissors. The pancreatic head and uncinate process of the portal vein, superior mesenteric vein, and superior mesenteric artery are also dissected using ultrasonic shears. The inferior pancreaticoduodenal and first jejunal artery are ligated, clipped, and resected. After putting patients in the Trendelenburg position, the fourth portion of the duodenum and proximal jejunum are mobilized, and the jejunum is transected 15–20 cm distal to the ligament of Treitz with a linear stapler. All peripancreatic lymphatic tissues are obtained en bloc with the specimen. The specimen is removed in an endo-bag through the umbilical trocar site extended 4–5 cm. Subsequently, the extended umbilical port is inserted through a single port (OCTO
Learning curve analysis
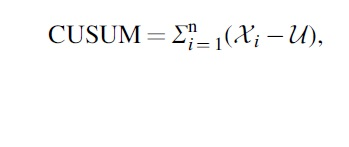
The CUSUM technique is a graphical tool used for detecting data patterns by measuring the sequential difference between the raw data and the mean value. In this study, cases were first ordered chronologically from the first to the last case, and the CUSUM of the operative time was defined as
with
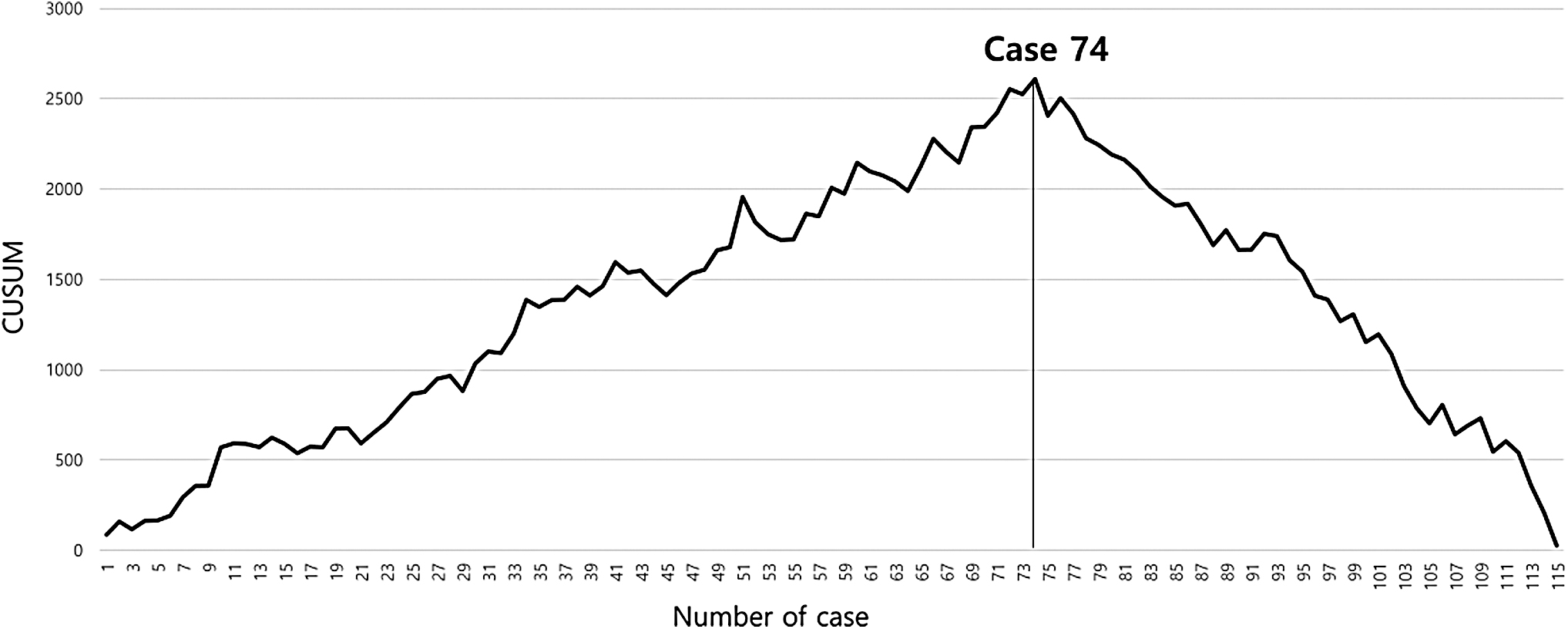
The RA-CUSUM was defined as

with  represents the event rate, and Pi is the expected LPD failure rate, which was calculated from the logistic regression model. Patients were classified into three groups based on the RA-CUSUM analysis.
represents the event rate, and Pi is the expected LPD failure rate, which was calculated from the logistic regression model. Patients were classified into three groups based on the RA-CUSUM analysis.
Statistical analysis
Continuous variables were represented as mean and standard deviation or median and interquartile ranges. All variables were tested for normality using a one-sample Kolmogorov–Smirnov test. To compare the three groups, a one-way analysis of variance, with Fisher's least significant difference correction for the post hoc analysis, was used for continuous variables, and Pearson's chi-square test was used for categorical variables. A chi-square test for trends was performed to assess whether there was an improvement in LPD among each phase. SPSS statistical software version 25.0 (IBM Corp., Armonk, NY) was used for all statistical analyses. P values were calculated using a .05 two-sided significance level.
Results
Basic characteristics of all patients
During this study period, 115 patients underwent LPD performed by 1 surgeon: 63 (54.8%) men and 52 (45.2%) women with a mean age of 65.1 ± 12.4 years and mean body mass index of 24.1 ± 3.3 kg/m2. Fifty-six (48.7%) and 59 patients (51.3%) were classified as ASA I/II and III/IV, respectively. LPD included malignant diseases (n = 76, 66.1%), and the R0 resection rate was 99.1%. The median operative time was 410.0 minutes (range 345.0–475.0 minutes), and the median estimated blood loss was 500.0 mL (range 300.0–600.0 mL). The intraoperative transfusion rate was 27.0%, and conversion to open PD occurred in 7 (6.1%) cases. Based on the Clavien–Dindo classification, there were 15 (13.0%) cases of grade II, 10 (8.7%) cases of grade IIIa, and 4 (3.5%) cases of grade IIIb postoperative complications. The 30-day mortality rate after LPD was 0.9% (n = 1) due to postoperative bleeding.
Learning curve analysis
For each of the patients, a graph of operative times was plotted in sequential order, demonstrating that operative times were slightly decreasing and that variances increased with experience (Fig. 1). The learning curve was identified using the CUSUM analysis. Based on the CUSUM graph for operative time, there was one peak point at 74 cases (Fig. 2). However, a reduction in operative time itself did necessarily imply LPD success. Therefore, the LPD learning curve was evaluated using the RA-CUSUM analysis method. Based on the RA-CUSUM analysis, 42 cases were required to achieve plateau performance, with 73 cases representing the minimal surgical failures for LPDs. Finally, three phases were assigned based on the learning curve for LPD: phase I (1st–42nd case), phase II (43rd–73rd case), and phase III (74th–115th case) (Fig. 3).

Graph for operative time against case numbers.
CUSUM analysis of the operative time. CUSUM, cumulative summation.
RA-CUSUM analysis for the surgical failure of LPD. LPD, laparoscopic pancreaticoduodenectomy; RA-CUSUM, risk-adjusted cumulative summation.
Comparison of patient characteristics and pathological outcomes between the three phases
Patient characteristics and pathological data among the three groups are summarized in Table 1. All groups were comparable in age at diagnosis and baseline body mass index and ASA classification. Regarding pathological data, there was no significant difference in tumor size, the rate of malignancies, and margin-positive resection between groups. Regarding the pathological diagnoses of heterogeneous tumor types, there were significant differences among phases (0.028); particularly, the pancreatic adenocarcinoma rate was 41.9% in phase II and 23.8% in phases I and III. Harvested lymph nodes increase constantly as phases progress and were significantly higher in phase III than in phase I (10.9 versus 14.6, P3 = .020). Portal vein resection was significantly better in phase II than phase I (4.8% versus 29.0%, P1 = .004), but there was no difference between phase II and phase III. Combined resection was also not different among the three phases.
Patient Characteristics and Pathological Data Among Three Phases
P1 indicates comparisons between phases 1 and 2; P2 indicates comparisons between phases 1 and 3; and P3 indicates comparisons between phases 2 and 3.
Others include gastrointestinal stromal tumors, chronic pancreatitis, and benign cystic neoplasm.
ASA, American Society of Anesthesiologists; BMI, body mass index; CBD, common bile duct; IPMN, intraductal papillary mucinous neoplasm; SD, standard deviation.
Comparison of intraoperative outcomes between the three phases
The mean operative time decreased with progressing phase (P < .001) (Table 2). The mean operation time was similar in phases I and II but was significantly decreased in phase III compared with that in phases I and II (348.5 minutes versus 444.6 minutes and 439.9 minutes, P2 < .001 and P3 < .001, respectively). The intraoperative transfusion rate, transfusion amounts, and estimated blood loss tended to decrease in all three phases, but there were no significant differences. However, the rate of the estimated blood loss >500 mL decreased significantly between the three phases (40.5%, 32.2%, and 16.7%; P = .017). The rate of open conversion also significantly decreased with phase progression (11.9%, 6.5%, and 0%; P = .023). Regarding open conversion, 5 patients in phase I required conversion to laparotomy due to adhesion (n = 1), bleeding (n = 2), acquisition for the surgical margin (n = 1), and vascular reconstruction (n = 1), whereas 2 patients in phase II required conversion to open surgery for the anatomical variation of the common hepatic artery from the superior mesenteric artery through the pancreas (n = 1) and vascular reconstruction (n = 1).
Perioperative Outcomes Among Three Phases
P1 indicates comparisons between phases 1 and 2; P2 indicates comparisons between phases 1 and 3; and P3 indicates comparisons between phases 2 and 3.
DGE, delayed gastric emptying; POPF, postoperative pancreatic fistula; PPH, postpancreatic hemorrhage; SD, standard deviation.
Comparison of postoperative outcomes between the three phases
The mean postoperative hospital stays tended to decrease in all three phases, with no significant differences (19.3, 15.1, and 14.2 days; P = .069). Overall complications and complications above IIIa, according to the Clavien–Dindo classification, were significantly lower as phases progressed (P < .001). Clinically relevant POPF was significantly different among the three phases (19.0%, 12.9%, and 4.8%; P = .046). PPH was also significantly lower as phases progressed (9.5%, 0% and 0%; P = .018). However, there were no differences in DGE, mortality, 30-day reoperation, and 30-day readmission.
Discussion
Since the first case of LPD was reported by Gagner and Pomp in 1994, studies reporting successful LPD in few specialized centers are steadily increasing. A recent meta-analysis presented the feasibility and safety of LPD compared with open PD in treating periampullary disease. 13 The benefits of LPD appear to be a simple and teachable demonstration of anatomy, reduction in blood loss, lower postoperative morbidity, quicker recovery, and shorter hospital stay.14–16 However, LPD remains the most challenging procedure for pancreatic surgeons because it requires not only extensive dissection around major blood vessels, but also the enhancement of multiple and complex anastomoses. Moreover, LPD was shown to have a long operative time and a steep learning curve. Nagakawa et al. reported that >30 cases are required for hepatopancreatobiliary surgeons to be proficient in performing LPD. They demonstrated that lymph node dissection, high visceral fat areas in patients, and cases of concomitant pancreatitis could all be avoided in the early stages of the learning curve. 17 Speicher et al. came to the same conclusion, stating that the learning curve for LPD could be represented by 10–50 cases. 18 Kuroki et al. reported a learning curve of 10 cases among 30 consecutive patients, suggesting that after overcoming the learning curve, operative time and blood loss were substantially reduced. 19 According to Wang et al., a minimum of 40 cases is required for laparoscopic surgeons with a certain level of experience. 20 However, these four reports had small sample sizes, included hybrid LPD, or used simple statistical methods. Moreover, a recent multicenter study on minimally invasive PD including 300 patients determined that 61, 32, and 68 cases were required for the operative time to plateau for the laparoscopic approach, the hybrid approach, and the robotic approach, respectively. 21 However, the heterogeneity of surgical approaches from the different surgeons in this study confounds objective analysis of the learning curve for this minimally invasive procedure.
In this study, the learning curve for LPD was determined using CUSUM analyses. CUSUM analyses are a useful tool that allows researchers to monitor operative time. The graphic displays obtained on CUSUM can be easily understood. An increasing trend indicates unacceptable surgical performance, and when this occurs, a careful review and modification of surgical procedures is necessary to achieve acceptable surgical performance. After 74 cases, the CUSUM graph started to descend in our study. However, since there is a limitation in evaluating the success and learning curve of LPD by simple operation time, an RA-CUSUM analysis that reflects open conversion, severe complications (Clavien–Dindo classification ≥IIIa), and POPF is required. The learning curve for LPD was determined to have three phases based on this analysis: phase I (1st–42nd case), phase II (43rd–73rd case), and phase III (74th–115th case). As phases progressed, the conversion rate, rate of complications graded Clavien–Dindo classification ≥IIIa, and POPF improved. In addition, the rate of estimated blood loss >500 mL also improved. However, there were no differences in the rate of intraoperative transfusion, transfusion amount, and estimated blood loss among the three groups. Our study showed also that the number of harvested lymph nodes improved as phases progressed, especially in phase III. The mean operative time was improved in phase III compared with that in phase I and phase II, but it was not significantly different in phase I and phase II, which is thought to be the result of performing more portal vein resections in phase II (29.0%) than in phase I (4.8%).
Recently, three single-center studies including >100 cases of LPD, exclusively, examined the learning curve with RA-CUSUM analysis. Our result is comparable with recently published studies. Song et al. showed that first-generation surgeons required 55 LPDs on the learning curve, with second-generation surgeons crossing the learning curve faster. 3 Yoon et al. reported that the reduction in the LPD failure was achieved within the first 60 cases and that the failure rate was stabilized at 84 cases. 9 Kang et al. reported that 40 LPDs were required to achieve technical competency and 100 LPDs were required to address extremely demanding cases. The same study recommend that patient selection, close observation, and expert advice were required for safe LPD in the first 40 cases. 8 The subsequent procedures included more challenging cases, such as portal vein resection, which comprised 11.3% of the total cases in phase III. Likewise, we performed LPD in phase I with careful patient selection and mentoring from an expert. However, 29% of all our portal vein resections were performed in phase II and our transition to phase III, at 73 cases, was slightly earlier.
The limitations of the study include its single-center single-surgeon design and the small number of cases. Heterogeneous tumor types may have also been a limitation of this study. In our opinion, a study performed in a single center has an advantage in measuring the learning curve because there are no variable factors (assistant, nurses, anesthesiologist, etc.) except the surgeon. This surgeon was trained at Asan Medical Center in a fellowship training program that included >500 cases of open or LPD. Based on the earlier experience, homogenous total LPD was possible from the first case without various trial errors or hand-assisted LPD. This surgeon had performed >100 open pancreaticoduodenectomies, 30 laparoscopic distal pancreatectomies, 12 laparoscopic bile duct resections, 35 laparoscopic hepatectomies, and >500 laparoscopic cholecystectomies in our center. Therefore, the results of this study might not be generalizable to other surgeons who have not achieved the same level of experience in laparoscopic hepatobiliary and pancreatic surgery.
Conclusion
In conclusion, LPD is safe and efficacious if performed by well-experienced laparoscopic hepatopancreaticobiliary surgeons. Conservatively, to plateau the LPD failure curve, at least 42 cases are required for these surgeons, and at least 73 cases are needed to stabilize the failure rate in difficult cases.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: study conception and design by H.K. and J.W.L.; data collection by H.K. and B.M.K.; analysis and interpretation of results by H.K. and H.Z.C.; draft article preparation by H.K. All authors reviewed the results and approved the final version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.