
Abstract
Perianal disease is a particularly morbid phenotype of Crohn's disease, affecting up to one third of patients, with a significantly diminished quality of life. Conventional medical therapy and surgical interventions have limited efficacy. Medical treatment options achieve long-term durable remission in only a third of patients. Therefore, most patients undergo an operation, leaving them with a chronic seton or at risk of incontinence with multiple interventions. Mesenchymal stem cell therapy is an emerging therapy without risk of incontinence and improved efficacy as compared with conventional therapy. Laser therapy is another new intervention. Unfortunately, up to 40% of patients still require a stoma related to perianal fistulizing disease.
Introduction
Crohn's Disease (CD) is an idiopathic disease of the gastrointestinal (GI) tract often presenting with fatigue, GI cramping and abdominal pain, and diarrhea. Characteristic transmural inflammation in CD can result in permanent bowel wall damage, and it manifests as a fistulizing phenotype. Perianal fistulizing disease has a varied presentation; some have one tract with minimal symptoms whereas others have numerous tracts, tracts involving the vagina, or tracts that are destructive to the anal canal, resulting in an element of incontinence. Due to its complexity and heterogeneity of symptomatology and classification symptoms, managing this disease phenotype is difficult, and it must be assessed on a case-by-case basis in a multidisciplinary fashion.
The incidence of perianal fistulizing disease varies from 5% to 40% among all patients with CD. 1 Patients with perianal fistulizing disease report poorer general health, vitality, social and physical functioning, and overall diminished quality of life. 2 For about 10% of patients, a perianal fistula is their first symptom of CD. Among these patients, the presence of these fistulas may precede a diagnosis of CD by 30 days to 20 years. 1 Though this is true, the presence of this fistula is indicative of a more serious manifestation of the disease itself, lending to vigorous medical care such as immunosuppressants, steroids, and surgery in nearly 83% of patients. 1 Disappointingly, up to 63% of patients with perianal fistulas present with refractory fistulas. 3 In addition, patients with perianal fistulas often have a recurrence within 2 years of the onset of their first fistula. 1 Risk for developing a perianal fistula increases with each year past the diagnosis of CD, settling around 50% at 20 years after the initial diagnosis. 1 New therapies, including laser treatment and mesenchymal stem cell delivery, have demonstrated promising results compared with conventional medical and surgical treatment.
Diagnosis
Among other morbidities involving CD, the presence of a fistula and its abscess are some of the most dreaded complications. Discharge, perianal redness, skin irritation, perianal pain, and pain when defecating are common symptoms of those with a perianal fistulizing CD (pCD). Before diagnosis, a thorough review of a patient's perianal and perineal regions must be conducted, paying particular attention to the presence of skin tags, hemorrhoidal tissue, rectal bleeding, and pain, as many of these are common symptoms of CD.
On conducting a full medical history and palpation and inspection of the fistula tract or abscess, a conclusion of the diagnosis can be made. Digital imaging is imperative to understand how to guide treatment for a patient after inspection of the area. Examination under anesthesia (EUA), magnetic resonance imaging (MRI) of the pelvis, and endoanal ultrasound (EUS), are the most promising imaging techniques with similar accuracies to diagnose and identify a fistula tract.
An MRI is often used for the initial diagnosis and follow-up to distinguish between the tract of a fistula and other structures in the pelvis. An MRI is best used to identify the openings of a fistula, and its extensions. 4 An EUS offers an ability to provide anatomical details about anal sphincter defects, which often is a sign of a perianal fistula.5,6 The EUA is also an assessment used to examine the perianal region and identify a fistula tract, usually preformed in the lithotomy or prone position, and it is quite useful when combined with MRI evaluation. Though there is no gold standard for diagnosing and identifying fistula tracts, a combination of imaging, and physical exam techniques provides excellent insight into guiding a treatment plan for patients with perianal fistulas.
Park's classification of pCD fistulas is a classification system used to diagnose a perianal fistula based on location in relation to the internal and external anal sphincter complex. Park describes four fistula presentations, including intersphincteric, extrasphincteric, suprasphinceric, and transsphincteric. Fistulas can also be described as complex, involving a high transsphincteric path, multiple external openings, and multiple tracts, and they may involve a rectovaginal path, or those with anorectal stricture, or active proctitis. Complex fistulas include all Crohn's and non-Crohn's fistulas. 7
Intersphincteric fistulas occur in 20%–45% of patients and do not penetrate the external anal sphincter. 8 A transsphincteric fistula, occurring in 30%–60% of cases, penetrates the external sphincter below the level of the puborectalis muscle, exiting within the ischiorectal fossa. Park's third classification, known as a suprasphincteric fistula, occurs in 20% of cases and describes a fistula tract that travels over the puborectalis, downward again to the ischiorectal fossa, and has an external opening in the perianal skin. An extrasphincteric fistula occurs in 2%–5% of cases, and it passes from the perineal skin through the ischiorectal fat and levator muscles into the rectum. 7 Due to the nature of complex fistulas involving the sphincter complex, surgical treatment has the risk of incontinence. 9
Medical Treatment Goals
A patient is considered healed of a perianal fistula when there is no drainage to the external palpation of the fistula tract, and the external opening is epithelialized. Radiographic healing may also be used in conjunction with clinical healing, and it is often defined as an MRI showing no abscess >2 cm in any two of three dimensions. Some patients may see improvement, rather than complete healing. However, the most critical definition of healing is to understand the patient's expectations and what defines healing according to their quality of life.
Poor quality of life is associated with poor social and physical functioning outcomes, and poor emotional status in patients with perianal fistulas. 10 More embarrassing for patients, sexual functional impairment is also associated with perianal fistulas and their treatment. 11 Communication on what a patient expects from a treatment and what they can and will not undergo is necessary to ensure satisfaction of treatment intervention.
Despite the wide range of treatment options available to treat a perianal fistula, only one third of patients undergo complete, lifetime remission on treatment of a complex fistula.1,12–14 For patients with simple fistulas, this number is higher at a range of 66%–88%.12,14 Fistula remission is positively associated with poorer quality-of-life scores. 2 Remission of a perianal fistula is defined by the closure of all fistulas after two consecutive examinations, at least 1 month after the treatment of the fistula. 15 Because for many patients, symptoms do not subside after treatment intervention, clinicians instead look for signs of improvement. Clinical resolution of a fistula tract is also concluded by radiographical imaging to identify scarring or the track that was closed on treatment. Successful treatment of a perianal fistula is most often determined via MRI post-intervention. The MRI provides the greatest acuity of fistula closure inside the anal canal.
Medical Therapy
Aminosalicyclates and corticosteroids are not effective for treating perianal fistulas, and they may even worsen symptoms of discharge. 16 Before the 1990s antibiotics were the standard for treating perianal fistulas, reducing drainage and the odds of fistula formation, but they were not effective for complete remission in most cases. 17 A small double-blind randomized control trial (RCT) did not demonstrate significant differences in the antibiotic ciprofloxacin 500 mg twice daily, compared with metronidazole 500 mg twice daily. Ciprofloxacin, however, was more effective than metronidazole in relieving symptoms in 40% of patients. 18 Today, antibiotics are nearly always used as an adjunct treatment to biologic therapy.
Biologic therapy is the current standard of care for patients with perianal fistulizing disease. In an RCT, 55% of patients had fistula closure in 3 months when taking infliximab, but this only offered complete closure in 36% of patients.19,20 Though the use of infliximab does not eliminate the need for surgery in many cases, it does prevent further hospitalizations and allows for fewer surgeries due to fistula complications. 21
Other anti-tumor necrosis factor (TNF) agents, adalimumab and certolizumab, have had no dedicated RCTs for patients with pCD only; however, they have been evaluated in generalized fistulizing disease. Adalimumab has been tested in two clinical trials, CLASSIC-1 and GAIN, where fistula closures did not differ significantly between patients given adalimumab versus placebo.22,23 In another RCT, CHARM, 30% of patients receiving adalimumab achieved closure at 26 weeks of treatment in comparison to 13% for patients given the placebo. 24 At 56 weeks, 33% of patients receiving adalimumab had achieved closure in comparison to 13% receiving the placebo. 24 One hundred percent of patients whose fistula had closed at 26 weeks remained closed at 56 weeks. 24
A retrospective analysis examining the efficacy of infliximab in comparison to adalimumab found infliximab to be more effective in treating pCD. Recurrence and aggravation rates were higher for adalimumab than in patients receiving infliximab. 25 Subgroup analyses of PRECiSE 2 examined fistula responses in patients receiving certolizumab. In patients with pCD, at 26 weeks, 36% of patients receiving certolizumab had closed fistulas compared with 17% in the placebo group. 26
Vedolizumab has been evaluated more recently on its clinical effectiveness to treat pCD from the GEMINI-2 clinical trial. 27 In an analysis of phase 3 results of the GEMINI-2 clinical trial, 34% fistula closure at 14 weeks was reported. 27 Interestingly, patients with pCD compared with a pooled fistulizing CD group experienced slightly faster closure rates when treated with vedolizumab compared with the placebo. 27 Ustekinumab is a newly approved immunosuppressant but has yet to have any dedicated RCT's to determine its clinical effectiveness. Open-label experiences in Spain and Canada do suggest clinical improvement in 50% of patients.28,29
Surgical Therapy
Given the limited efficacy of medical treatment alone, nearly 90% of patients with pCD will undergo at least one surgical intervention to close a perianal fistula.1,30 Unfortunately, surgery does not always achieve remission, and it has the dreaded potential complication of incontinence. 30 As many patients with CD inherently suffer from incontinence, sphincter preservation is necessary when possible to ensure a good quality of life postoperatively. 31 Several surgical treatment options exist to treat perianal fistulas, but a multidisciplinary approach with concurrent medical therapy achieves the most effective results of treating pCD. 32
Incision and drainage of abscess
Nearly 65% of patients with a perianal abscess will develop a fistula. 33 It is important to drain an abscess and/or fistula before bacterial invasion of surrounding soft tissue, which could lead to local sepsis. Incision and drainage of a perianal fistula is the most common preoperative intervention to treat an undrained fistula or abscess. 34 Small abscesses <1 cm may be treated with medical therapy alone, but they are not recommended unless patients have other comorbidities. Larger abscesses are drained by making an incision on the skin and allowing drainage of the abscess. Further packing may be necessary to prevent another infection. 35
Seton placement
A seton is most often a nonabsorbable suture tied through a fistula tract to encourage both excess drainage out of the tract and fibrosis of the tract (Fig. 1). Subsequently, sphincter continuity is preserved. 9 Removal of the seton is difficult to gauge, as if left in for too long, the tract will epithelize and remain open. When left in for too little amount of time, the fistula cannot heal properly, and local sepsis may return.
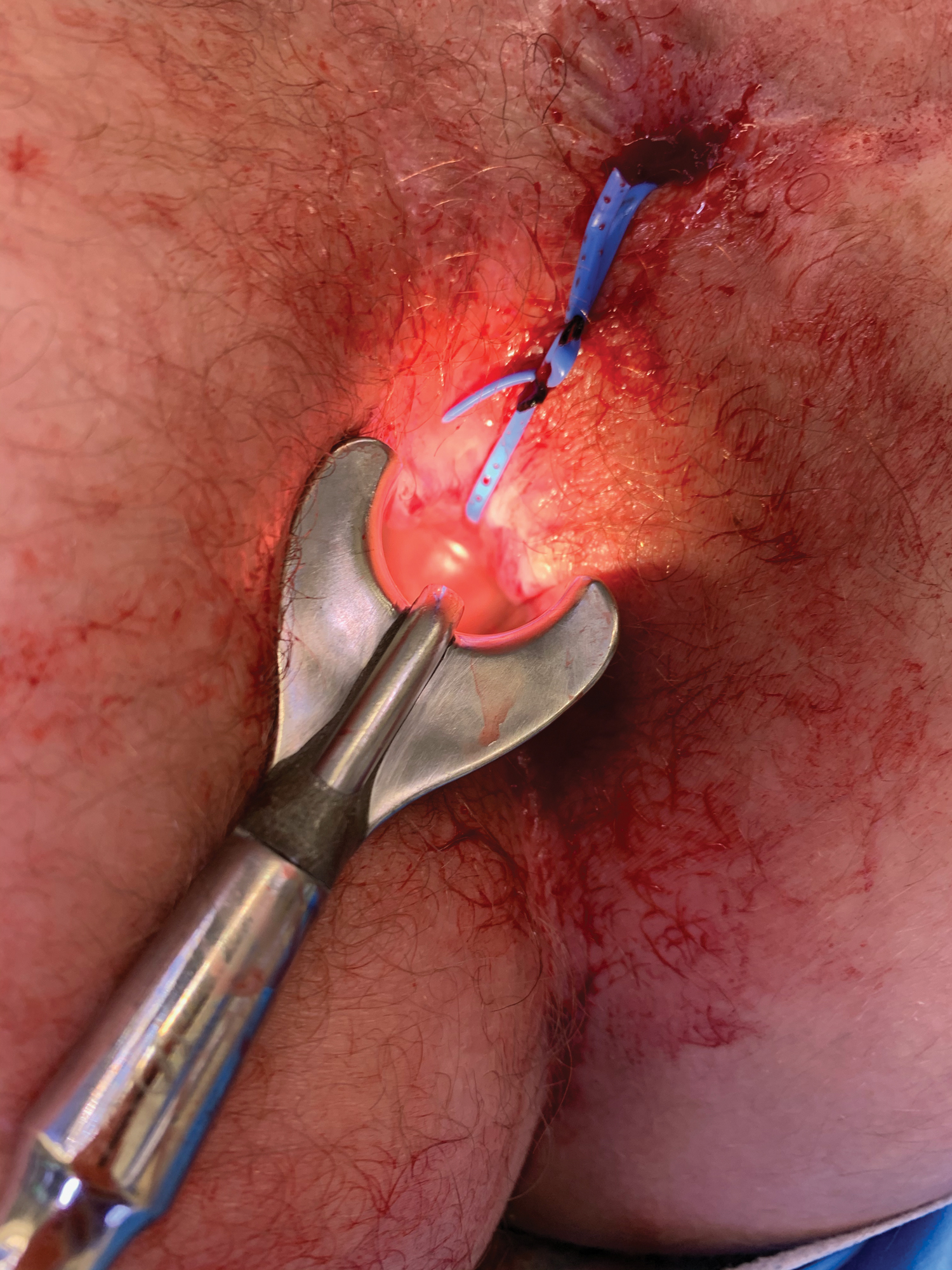
Placement of a seton in a transphincteric fistula tract. Color images are available online.
Seton placement is strongly recommended as an adjunct therapy to immunosuppressant agents or antibiotics in patients with a complex fistula. 32 Seton removal on its own reveals variable rates of recurrence and fistula closure. When alone and combined with other therapies such as anti-TNF agents, it is important to consider the timing of induction therapy in comparison to seton placement as this can influence abscess recurrence. 32 Moreover, seton removal leads to a recurrence of an abscess 70% of the time. The use of a cutting seton is discouraged, as it can lead to incontinence.32,36 If there is ongoing anal canal inflammation, it would be futile to remove the seton as the risk for perineal sepsis is nearly 100%. For patients with active proctitis, seton placement with concurrent medical therapy is currently the best treatment approach.
Fibrin glue and fistula plug
Fibrin glue use to treat perianal fistulas was initially popular due to early promising results. Fibrin glue is a mixture of both fibrinogen and thrombin, encouraging healing of the fistula tract by sealing the fistula tract and strengthening the final stage of the coagulation cascade. 37 However subsequent studies including a multicenter, open-label, RCT in France have found lower rates of fistula healing; 38% of patients were in complete remission at 4 weeks in the French study. Of note, studies have found that fibrin glue is more effective in treating simple fistulas (44% remission at 4 weeks) than complex fistulas (25% remission at 4 weeks). 38
Fistula plugs are bioabsorbable plugs inserted into a fistula tract and sutured into place. Over time, the fistula heals around the plug as the plug is slowly incorporated during the healing process. A large RCT found a success rate of 55% at 12 months post-intervention for patients with a fistula plug, consistent with larger systematic reviews of the efficacy of these plugs.39–41 Despite low closure rates in comparison to other treatments, reported incontinence rates are very low.
Fistulotomy
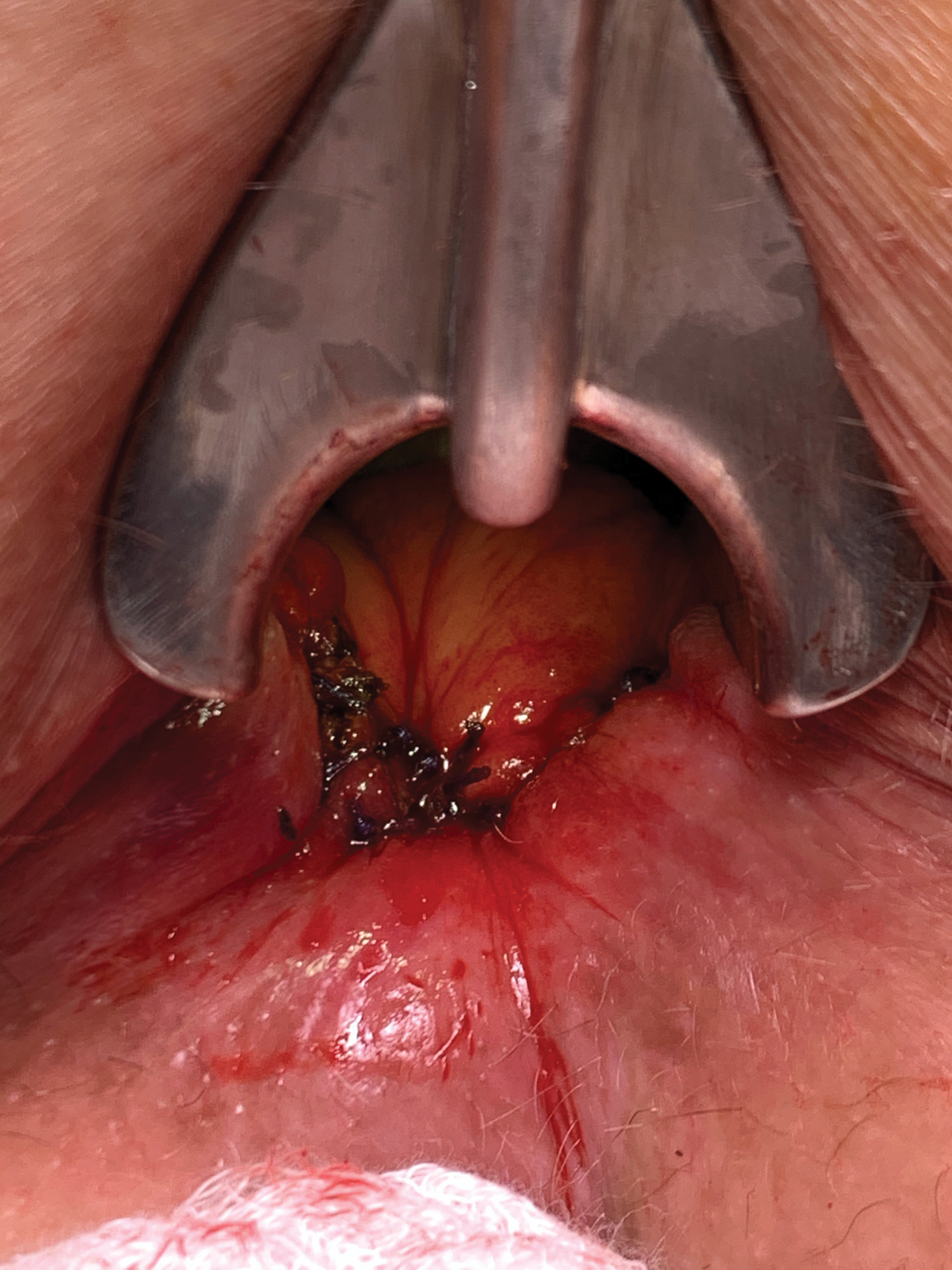
A fistulotomy is performed on patients with low or midlevel transsphincteric fistulas presenting without proctitis, or anal canal disease (Fig. 2). These highly select patients result in healing rates of 80%–100%.42,43 Rarely, this procedure is done in patients with CD due to sphincter involvement and incontinence risk, proctitis, anal canal disease, and diarrhea, in many patients. Moreover, patients with CD undergoing a fistulotomy with concurrent proctitis experience healing rates of 27%. 44 In patients with greater than one-third sphincter involvement, a fistulotomy should not be performed because >50% of patients express an increase in incontinence. 45

Fistulotomy. Color images are available online.
Endorectal advancement flap
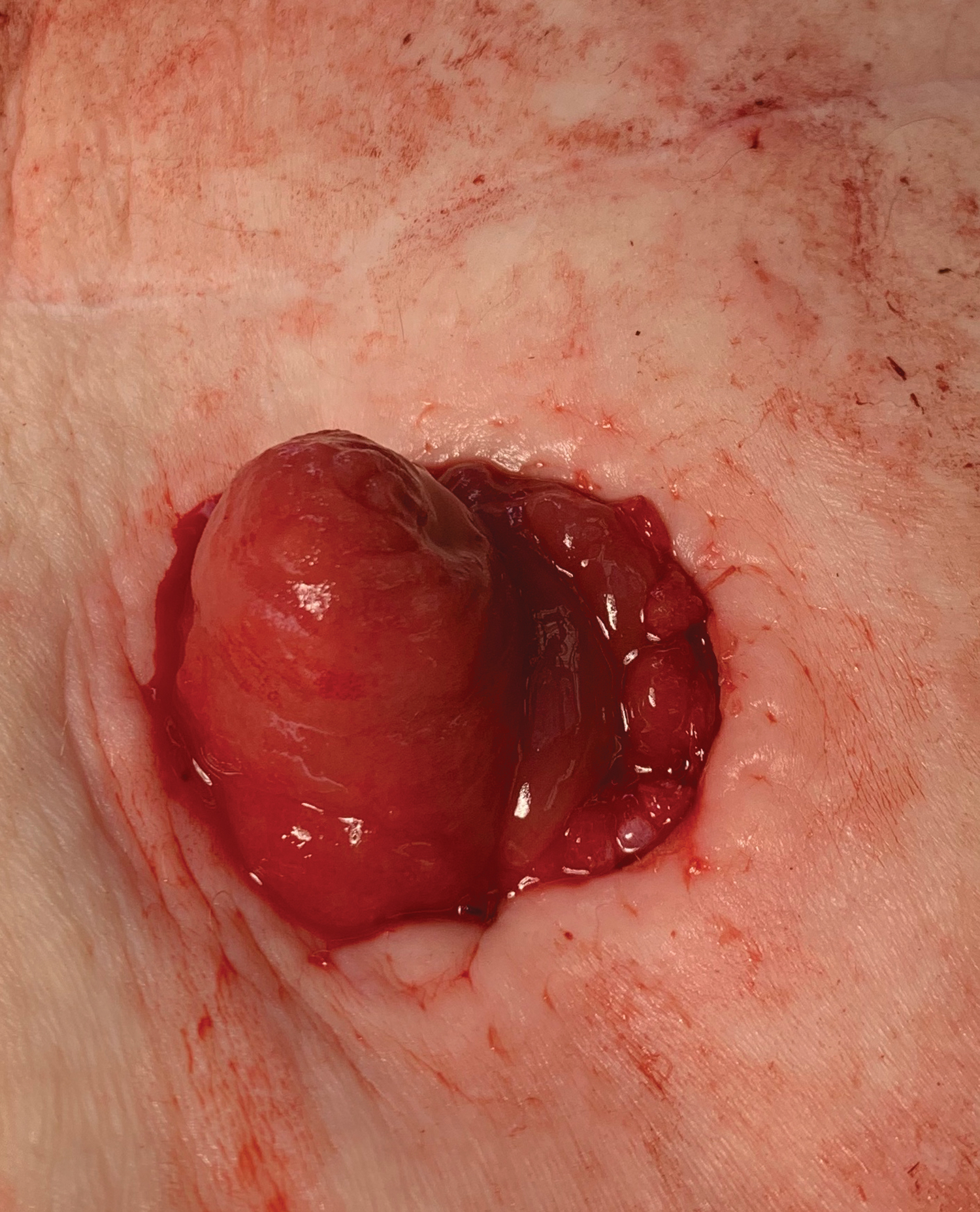
An endorectal advancement flap is a procedure involving removing a full or partial-thickness rectal mucosal flap of “U shaped” rectal tissue, covering the internal opening of the fistula tract. The external sphincter muscle is preserved (Fig. 3). Closure of fistula tracts from this procedure is variable, ranging from 33% to 92%. 46 Postoperative incontinence rates range between 0% and 28%, with an average of 9%. 46 Interestingly, in a multicenter retrospective review, patients undergoing an endorectal advancement flap procedure with some use of postoperative immunotherapy had a 92% success rate from their endorectal advancement flap. 47 Despite low incontinence rates and higher success rates of this procedure, careful patient selection must be taken into consideration. 47
Closure of an endorectal mucosal advancement flap using interrupted 2-0 vicryl. Color images are available online.
Ligation of the intersphincteric tract procedure
The ligation of the intersphincteric tract (LIFT) procedure involves closing the internal openings of the fistula(s) by making an incision at the intersphincteric groove, identifying the intersphincteric tract, ligating the ends of the internal and external openings, and disconnecting the fistula between the two openings (Fig. 4). Despite early signs of significant improvement in patients undergoing this procedure in 2009, reporting nearly 95% of patients healing of their fistula tract(s), more recent studies have reported much lower success rates of around 40% on initial surgery. 48 Other studies of LIFT's outcomes demonstrate variable results ranging from 57% to 83%. 49
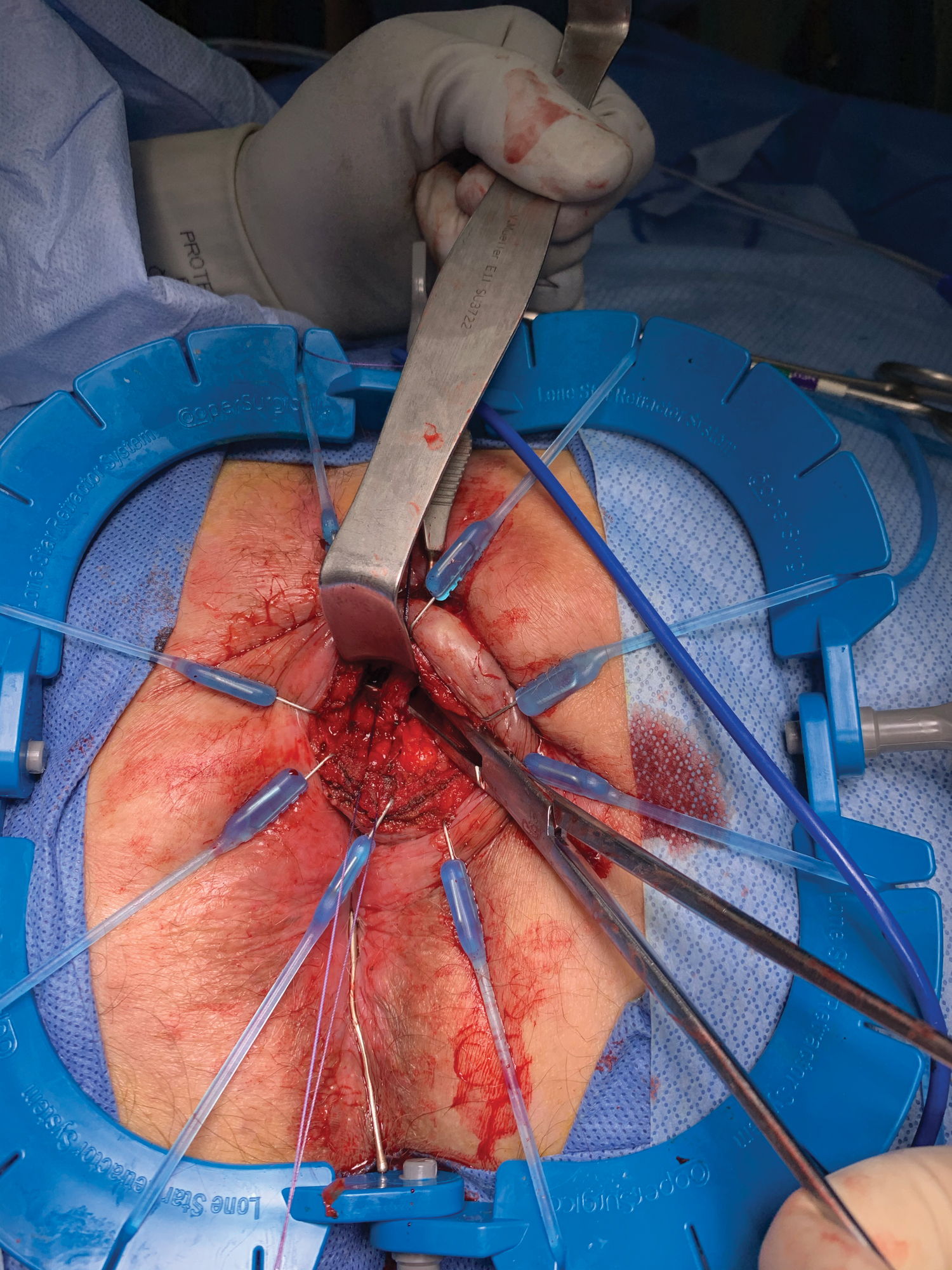
Exposure of a transsphincteric fistula during a ligation of an intersphincteric fistula tract. Color images are available online.
Significant factors for long-term LIFT site healing have been reported to be lateral versus midline location, and longer mean fistula tract length. 50 Gingold et al. found, in a single-center prospective study, that the LIFT procedure in patients with pCD was safe, and effective in reducing reoccurrence of new fistula formation, while preserving continence, and preventing wound-healing complications. 50 Intriguingly, in another single-center prospective study by Cedars- Sinai, Kamiński et al. found the LIFT procedure to be more successful in patients with small bowel CD than patients with colonic CD, most likely due to the nature of the location of colonic CD. 51 BioLIFT is a newer procedure described by Elliott in 2010, in which a standard LIFT procedure is done, while interpositioning a biological mesh in the intersphincteric plane. A retrospective study found the BioLIFT procedure to have a healing rate of 75% in comparison to the standard LIFT procedure at 59%. 52 Despite variable findings for the LIFT procedure, it seems to be a safe and effective surgical treatment option.
Proctectomy
In refractory cases where both medical management and surgical therapy have consistently failed, a proctectomy can be performed to eliminate the symptoms of the patient's fistula, but this leaves a patient with a permanent ostomy. Reported rates of proctectomy for patients with pCD range from 8% to 40%. 53 This rate is higher in patients with severe incontinence, multiple operations for perianal CD, previous temporary fecal diversion, 54 Crohn's colitis with rectal sparing, and Crohn's colitis with active proctitis. 55
Postoperative success is often determined by postoperative care and minimizing preoperative morbidities. Genua et al. found increasing success rates in patients whose perineum was healed as much as possible before the proctectomy, cessation of smoking preoperatively, and using a low Hartmann's procedure intraoperatively. 56 A low Hartmann's approach before a proctectomy was found to have an 88% success rate of perineal wound healing at a median follow-up time of 69 months. 56 Interestingly, use of the gracilis muscle in patients with refractory perianal disease after a proctectomy has demonstrated promising results with perineal wound healing in 72%–80% of patients.57,58
Fecal diversion
Fecal diversion is often used in patients with refractory pCD to prevent a proctectomy and improve the perianal sepsis before proctectomy to improve postoperative outcomes 54 (Fig. 5). Unfortunately, most patients with a fecal diversion end up having a permanent diversion, as diversion alone is not particular effective for long-term remission. Singh et al. reported in a large systematic review that 42% of patients with temporary diversion will ultimately undergo proctectomy to address their perianal disease, underscoring the limitations of diversion alone. However, 66% of patients demonstrate some signs of clinical improvement after undergoing a fecal diversion. 54 Unfortunately, 31%–49% of patients with pCD may need a permanent stoma after attempting a fecal diversion. 59
Diverting loop ileostomy. Color images are available online.
New Therapies
Stem cell therapy
Despite 56% of patients healing fistulas from infliximab and seton placement and 64% with optimized tissue flaps, 40% of patients are not healed after several therapies, and they may require a proctectomy later in life.46,53,60,61 Though disappointing, mesenchymal stem cell therapy has demonstrated promising results in phase I, II, and III clinical trials. Mesenchymal stem cells are multipotent adult cells isolated from adipose tissue and bone marrow. 62 Mesenchymal stem cells are delivered to patients via direct injection into the wall of the fistula tract. Aggressive curettage is necessary to clean the fistula tract earlier, ensuring that fibrotic tissue does not prevent the mesenchymal stem cells from penetrating the surrounding tissue. 63
The first reported successful treatment of a rectovaginal fistula was in 2003. 64 Since then, several lines of mesenchymal stem cells have been researched and used in phase I,65–68 II,69–71 and III 72 clinical trials. Namely, autologous and allogenic adipose and bone marrow stem cell therapies have demonstrated promising results. Overall, 75%–89% of patients have had fistula resolution with autologous adipose therapy, 88% 1 year after autologous bone marrow therapy, 59%–65% remission in patients receiving allogenic adipose therapy, and up to 85% healing in allogenic bone marrow therapy. 63
All clinical trials have reported therapies to be safe and feasible. In addition, there is no risk of incontinence. Given the success of clinical trials, future directions for these therapies will focus on the number of cells delivered per patient, need for repeat dosing, and optimal cell manufacturing to decrease the overall cost.
Laser treatment
Developed in Germany, a radial emitting laser probe, FiLAC™, destroys both the epithelium and crypt gland of a fistula track. Laser energy emitted by the probe demolishes both the internal and external fistula tract openings while preserving sphincter continuity in most cases. Therefore, this technique may provide a minimally invasive option for patients with pCD. Early studies demonstrated promising results, with 82%–92% of patients healed of their fistula 25 months post-intervention.73,74 This study found no difference in patients with cryptoglandular fistulas in comparison to Crohn's related fistulas. In a large FiLAC treated fistula series, the only predictor of healing was done with a intersphincteric fistula location. 74
Conclusion
The complexity and diversity of clinical presentations of perianal fistulizing disease rears a gold standard treatment that is nearly impossible. Combinations of medical and surgical therapy provide some relief to patients with pCD but are not very effective in achieving complete remission or preventing fistula recurrence. Emerging mesenchymal stem cell therapies should provide hope for providing permanent relief for patients with perianal fistulizing disease.
Footnotes
Disclosure Statement
A.L.L. is a consultant for Takeda.
Funding Information
No funding was received by either author for this manuscript.