
Abstract
Introduction:
Transanal total mesorectal excision (TaTME) is a novel technique that overcomes the problem of access to the deep pelvis during radical surgery for mid-rectal and lower rectal cancer. Although TaTME has several important steps, the creation of the distal purse-string suture following TaTME plays an important role in ensuring the integrity of the colorectal anastomosis. However, this procedure represents a major technical challenge for the surgeon. Robot-assisted surgery may make this suturing procedure easier than laparoscopic surgery because it permits intuitive wrist movements and a three-dimensional view. The aim of the present study was to investigate the usefulness of transabdominal robotic purse-string suture during anastomosis in TaTME.
Methods:
Twenty-seven patients, who underwent anastomosis using a single stapling technique (SST) during the TaTME of mid-rectal or lower rectal cancer, were enrolled in the study. The patients were allocated to two groups: 11 patients underwent transabdominal robotic purse-string suturing (the Robot group) and 16 patients underwent transanal purse-string suturing (the Transanal group). The characteristics and short-term surgical outcomes of the participants were compared between the two groups.
Results:
The Robot group tended to have a shorter purse-string suturing time (541 ± 206 seconds versus 729 ± 310 seconds; P = .07). Regarding the shape of the “donut” after SST anastomosis, in the Transanal group, 5 of the 16 participants had incomplete donuts with muscular defects and required additional suturing, whereas in the Robot group, all the participants had complete donuts (P = .04).
Conclusions:
Transabdominal robotic purse-string suturing may facilitate the suturing procedure and contribute to reliable anastomosis.
Introduction
Total mesorectal excision (TME) has been widely recognized as the standard treatment for patients with rectal cancer since the associated dramatic improvement in overall survival of patients with rectal cancer was first reported in 1982. 1 Transanal total mesorectal excision (TaTME), which was introduced in 2013, 2 is a technique that overcomes the problem of access to the deep pelvis during radical surgery for mid-rectal or lower rectal cancer. Several subsequent systematic reviews have suggested that TaTME is a viable alternative to open or laparoscopic TME, with similar or better oncological outcomes. In such studies, TaTME has been shown to be characterized by a longer circumferential resection margin (CRM), a lower incidence of tumor-positive CRM, and a larger distal resection margin.3–6
TaTME has several important steps, but the creation of the distal purse-string suture following TaTME plays an important role in ensuring the integrity of the colorectal anastomosis. However, it is a major technical challenge for the surgeon to master this technique, and this requires appropriate training. 7 The placement of an incomplete purse-string suture increases the risk of anastomotic leakage and can result in severe morbidity and mortality. In particular, long-term anorectal dysfunction can ensue, which increases the risk of local recurrence, 8 alongside reductions in overall and disease-free survival.9–11 The prevalence of anastomotic leakage following TaTME is reported to be 5.4%–15.7%,3–6,12–14 which requires improvement.
Robot-assisted TME surgery for rectal cancer was first reported in 2006, 15 and the number of such procedures being performed is increasing worldwide. Robot-assisted surgery makes the suturing procedure easier than laparoscopic surgery; this is because it permits intuitive wrist movements and a three-dimensional view. 16 Furthermore, a hybrid method that combines the robotic abdominal approach and conventional TaTME has been reported. 17 However, there have been no studies of the placement of purse-string sutures using a robotic abdominal approach. Therefore, the aim of the present study was to investigate the usefulness of transabdominal robotic purse-string suture placement during the anastomosis in TaTME.
Materials and Methods
Of the 47 patients who underwent TaTME for mid-rectal or lower rectal cancer between April 2017 and November 2020 at Tokushima University Hospital, those who underwent anastomosis by manual suturing were excluded, and the 27 patients who underwent anastomosis using a single stapling technique were enrolled in the study. The participants were allocated to two groups: those who underwent transabdominal robotic purse-string suture (the Robot group, n = 11) and those who underwent transanal purse-string suturing (the Transanal group, n = 16). The characteristics and short-term surgical outcomes of the participants were compared between the two groups.
Tokushima University approved the study protocol (ToCMS ID; 2389).
Surgical procedure
The medial-to-lateral abdominal approach and lymph node dissection were performed using a standard laparoscopic or robotic (da Vinci Xi surgical system; Intuitive, Inc., Sunnyvale CA) procedure. After abdominal and transanal TME had been performed and the rectum freed, it was exteriorized through the abdominal incision. Extracorporeal division of the proximal colon was then performed, and the anvil of the circular stapler was inserted into the stump of the proximal colon. A purse-string suture was placed in the distal stump using 2-0 Proline (Ethicon Inc., Cincinnati, OH), full-thickness bites of the rectal wall were taken, and 10–14 sutures were placed in both groups (Fig. 1).
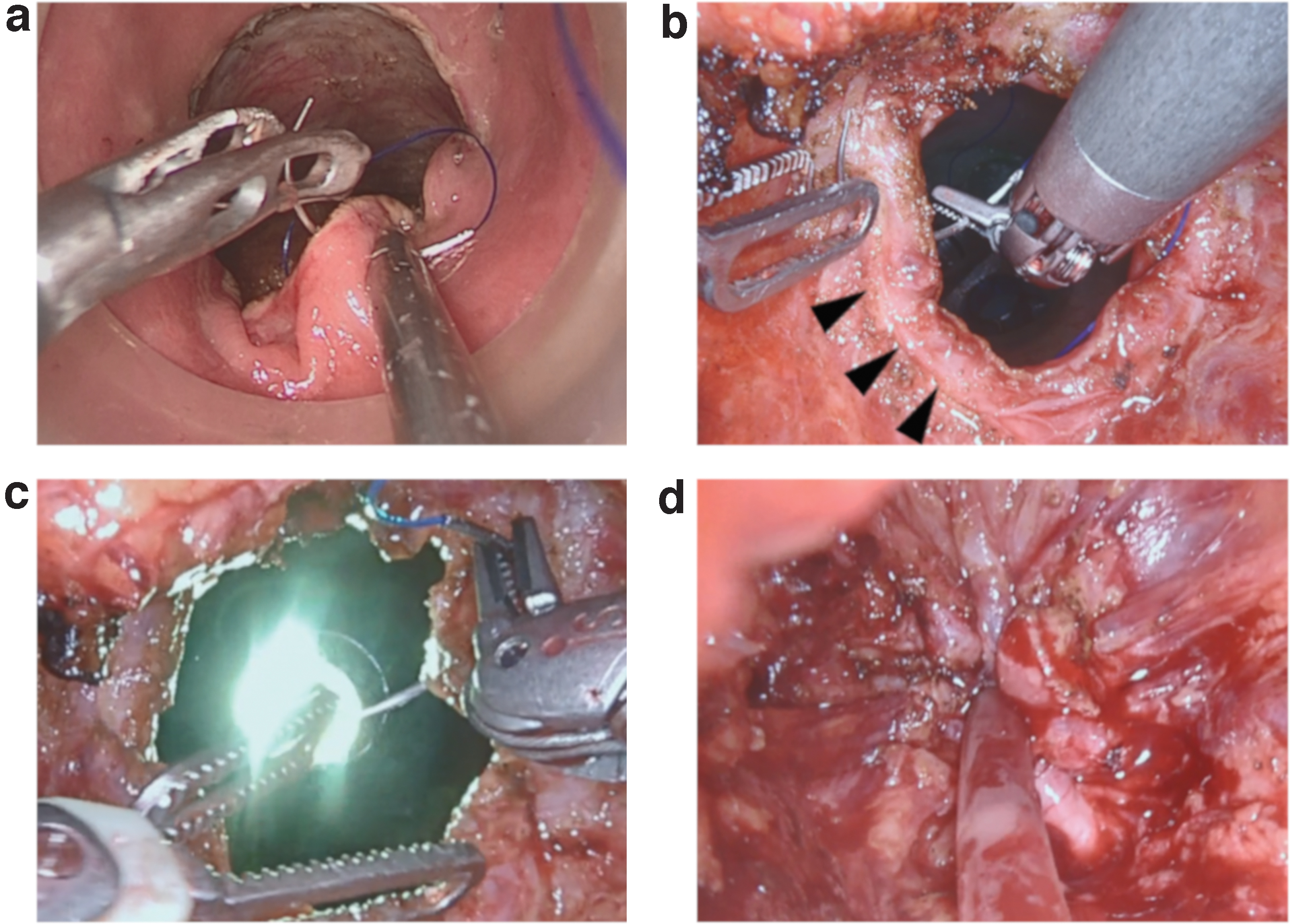
Placement of a purse-string suture in the distal intestinal stump.
After the purse-string suture had been placed, a 10-F Nelaton catheter was inserted transanally, through the purse-string suture, into the pelvis. The purse-string was then tied tightly around the catheter, and the shaft of the 28-mm EEA circular stapler (Medtronic Inc., Minneapolis, MN) was connected to the catheter. The shaft was then inserted into the pelvic space, using the catheter as a guide. Then, end-to-end single circular stapling anastomosis was performed. The shape of the donut was confirmed, and it was defined as a “complete donut” if the mucous and muscular layers were connected, and an “incomplete donut” if they were not fully connected. Reinforcing sutures were then added to incomplete donuts. Finally, a diverting ileostomy was placed in the right lower abdomen.
Robotic purse-string suture placement
The field of view was secured using a Tip-Up fenestrated grasper (Intuitive) that was inserted from the fourth arm in the lower right abdomen, fenestrated bipolar forceps (Intuitive) were attached to the first arm in the upper left abdomen, and a needle driver (Intuitive) was attached to the third arm in the lower right abdomen. The purse-string suture was started from the 9-O'clock position, the needle was passed from the mucous membrane into the muscular layer, and this was repeated in a counterclockwise direction (Fig. 1b). Then, from the 3-O'clock position, the needle was passed from the muscular layer toward the mucous membrane, until the entire circumference of the gut had been sutured (Fig. 1c). Finally, the needle was transanally collected and the suture material was cut at an appropriate length. The purse-string was then tied tightly around the inserted catheter (Fig. 1d).
The ethics committee of Tokushima University approved the study protocol (ToCMS ID; 2389), and all the participants gave their written informed consent.
Statistical analyses
The Wilcoxon two-sample test and χ 2 test were used to compare categorical data between the two groups. The results are presented as mean ± SD. All statistical analyses were performed using the JMP 10 software package (SAS Institute Inc., Tokyo, Japan). P < .05 was considered to indicate statistical significance, and P < .10 was considered to represent a tendency.
Results
Table 1 shows the characteristics of the participants in each group. No significant differences were found in these characteristics, which included age, sex, body mass index, tumor location, tumor diameter, and surgical procedure.
Comparison of the Characteristics of the Transanal and Robot Groups
The Wilcoxon two-sample and χ 2 tests were used.
AV, anal verge; BMI, body mass index; ISR, internal sphincter resection; Lap, laparoscopy; LAR, low anterior resection; LLND, lateral lymph node dissection; Pre-CRT, preoperative chemoradiotherapy.
No significant differences were found between the two groups in the number of bites taken or the number of times the needle was changed with the right hand (Table 2). However, the time taken for purse-string suturing tended to be lower in the Robot group (541 ± 206 seconds versus 729 ± 310 seconds; P = .07). In the Transanal group, 5 of the 16 cases had incomplete donuts, with muscular defects, that required the placement of additional sutures, whereas in the Robot group, all the cases had complete donuts (P = .04). Although the incidence of anastomotic leakage did not significantly differ between the groups, two minor leakages occurred in the Transanal group, whereas none occurred in the Robot group (P = .22). Neither of the affected participants required further surgery. The overall incidence of anastomotic leakage was 7.4%. Anastomotic stricture, requiring dilatation, did not occur in any of the participants, and the closure of the diverting ileostomy was performed in all the participants as previously scheduled.
Comparison of the Short-Term Outcomes in the Transanal and Robot Groups
The Wilcoxon two-sample and χ 2 tests were used.
CD, Clavien–Dindo; CRM, circumferential resection margin; LLND, lateral lymph node dissection.
Discussion
In the present study, we have shown that robotic purse-string suture placement facilitates the creation of a complete donut more reliably and quickly than conventional transanal purse-string suturing. This suggests that robotic purse-string suturing picks up the muscle layer more reliably and makes the placement of these sutures easier.
The creation of a distal purse-string suture plays a critical role in ensuring the integrity of the anastomosis in TaTME. Wu et al. have standardized and reported the technique for the placement of TaTME purse-string sutures, including with regard to needle orientation and bite interval. 18 However, it is difficult for surgeons to master this single-port laparoscopy procedure, and appropriate training is required. 7 Hardon et al. developed a training box for transanal purse-string suturing and reported that the force and torque measured at the entrance port and the tissue interaction force signatures provide risk-related insights into instrument handling, instrument loading, and tissue handling during purse-string suturing in this context. 19 Furthermore, Penna et al. reported that frozen cadaver training improves the quality of surgery and contributes to the safe introduction of TaTME. 20 Furthermore, Koedam et al. evaluated the learning curve for TaTME and reported that the incidences of significant complications and anastomotic leakage were reduced after 40 procedures had been performed. 21
Robot-assisted surgery has been reported to provide comparable perioperative outcomes and may be associated with a lower incidence of urogenital dysfunction than laparoscopic surgery.22,23 In robot-assisted surgery, the freer wrist movement and the three-dimensional view make the suturing procedure easier than during laparoscopic surgery. Leijte et al. reported that surgeons learned the technique of minimally invasive in a simulated setting more rapidly using robotic assistance than using laparoscopy. 16 In the present study, we found that the suturing time tended to be shorter in the Robot group, even though the number of bites and the number of times the needle was changed with the right hand were the same in each group. This suggests that robotic suturing is easier than single-port transanal anastomosis.
We also found that robotic suturing form more complete donuts than transanal anastomosis. In transanal suturing, it is difficult to confirm whether the needle is passed through the muscular layer because the suturing procedure starts from the mucosal surface (Fig. 1a). In contrast, in robotic transabdominal suturing, the muscle layer can be directly observed and the needle can be more reliably passed through the muscular layer. Therefore, transabdominal suturing that permits confirmation of the inclusion of the muscular layer is preferable to transanal suturing for the creation of a complete donut, and preferable to conventional laparoscopic surgery for suturing in the narrow pelvic space. However, in cases where the anastomosis is close to the anus and the pelvis is narrow, manually placed transanal sutures may be required because the pelvic wall prevents the correct operation of the robot arm.
In the Robot group, no anastomotic leakage was observed, which suggests that it may be an effective means of reducing anastomotic leakage. The small sample size was the principal limitation of the present study, which should be addressed by the inclusion of larger numbers of patients in future studies.
Conclusions
In conclusion, compared with single-port transanal purse-string suture placement, transabdominal robotic purse-string suturing may make the procedure easier and contribute to more reliable anastomosis.
Footnotes
Authors' Contributions
All authors are in agreement with the content of the article. In keeping with the latest guidelines of the International Committee of Medical Journal Editors, each author's contribution to the article is to be quantified.
Acknowledgment
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.