
Abstract
Background:
Minimally invasive surgery has a different visual and tactile perception compared with conventional surgery, which could lead to complications, especially in complex procedures. In these cases, flexible endoscopy can facilitate and prevent complications in minimally invasive procedures in children. The study aimed to clarify the utility of intraoperative endoscopy as an adjuvant to minimally invasive surgery in children.
Materials and Methods:
This retrospective study reviewed the medical records of pediatric patients who had undergone endoscopy during a minimally invasive surgery to treat an upper digestive pathology between January 2000 and December 2020.
Results:
The study included 83 patients who underwent a laparoscopic procedure with simultaneous endoscopy. The diagnosis was peptic stenosis in 9 patients, achalasia in 23, congenital embryonic tracheobronchial remnants in 4, re-fundoplication in 42, esophageal duplication in 2, superior mesenteric artery syndrome in 2, and giant gastric hemangioma in 1 patient. With adjuvant endoscopy, 7 digestive perforations were noted, 11 cases of short esophagus were diagnosed, and the permeability of the anastomosis was confirmed in 6 cases. No complications were related with the endoscopy procedures.
Discussion:
Minimally invasive surgery has a few special and tactile limitations that can lead to complications in certain procedures. Simultaneous digestive endoscopy in the upper gastrointestinal tract facilitates organ identification and dissection.
Conclusion:
Digestive endoscopy is an excellent adjunct to minimally invasive surgery in children because it facilitates and identifies complications and ensures safer minimally invasive surgeries. Future prospective studies are required to assess this conclusion.
Introduction
Minimally invasive surgeries in children are becoming more frequent and they are now the standard for several pathologies in children that require surgical resolution.1–4 Minimally invasive surgeries are used for notably complex procedures that have higher conversion and complication risk, 2 and they are performed with a different visual and tactile perception compared with conventional surgery. In these cases, flexible endoscopy can facilitate minimally invasive procedures in children and prevent complications.1,3
The benefits of adjunct endoscopy in laparoscopy, as a method to decrease complications, have been described in adults.5,6 In children, the usefulness and safety of endoscopy as an adjuvant to minimally invasive surgery in complex and high-risk procedures has been demonstrated mostly in clinical case reports.1,7–10 Davenport and colleagues demonstrated the usefulness and safety of endoscopy as an adjuvant or substitute to minimally invasive procedures in a group of 30 children. 1
This study aimed to demonstrate the usefulness of endoscopy as an adjuvant to minimally invasive surgery in the resolution of complex upper digestive pathology in children.
Materials and Methods
The study was conducted in the surgery department of a pediatric hospital. The retrospective and descriptive design of this study was approved by the institutional teaching committee. The study included children who underwent surgery between January 2000 and December 2020 and had undergone endoscopic assistance during a minimally invasive surgery to resolve an upper digestive pathology. The medical records of the treated patients were reviewed by the same surgical team who had experience in endoscopic and minimally invasive procedures. Age, gender, diagnosis, type of surgery, intraoperative findings, the procedure performed, modifications to the original procedure, complications, and postoperative evolution were analyzed.
This is a descriptive study; therefore, only an Excel sheet was used to analyze the data. No other software was used. The study was conducted in abidance of Hospital Infantil Privado's scientific committee policies, including obtaining informed consent from all involved subjects.
Results
Eighty-three patients who had undergone esophageal, gastric, and duodenal surgery using a minimally invasive approach with endoscopic assistance were studied (Fig. 1). The patients' ages ranged from 1 month to 20 years. The findings and procedures were grouped according to the following diagnoses:

Layout of the laparoscopy and endoscopy equipment, showing the monitors for the minimally invasive surgery and the endoscope. Color images are available online.
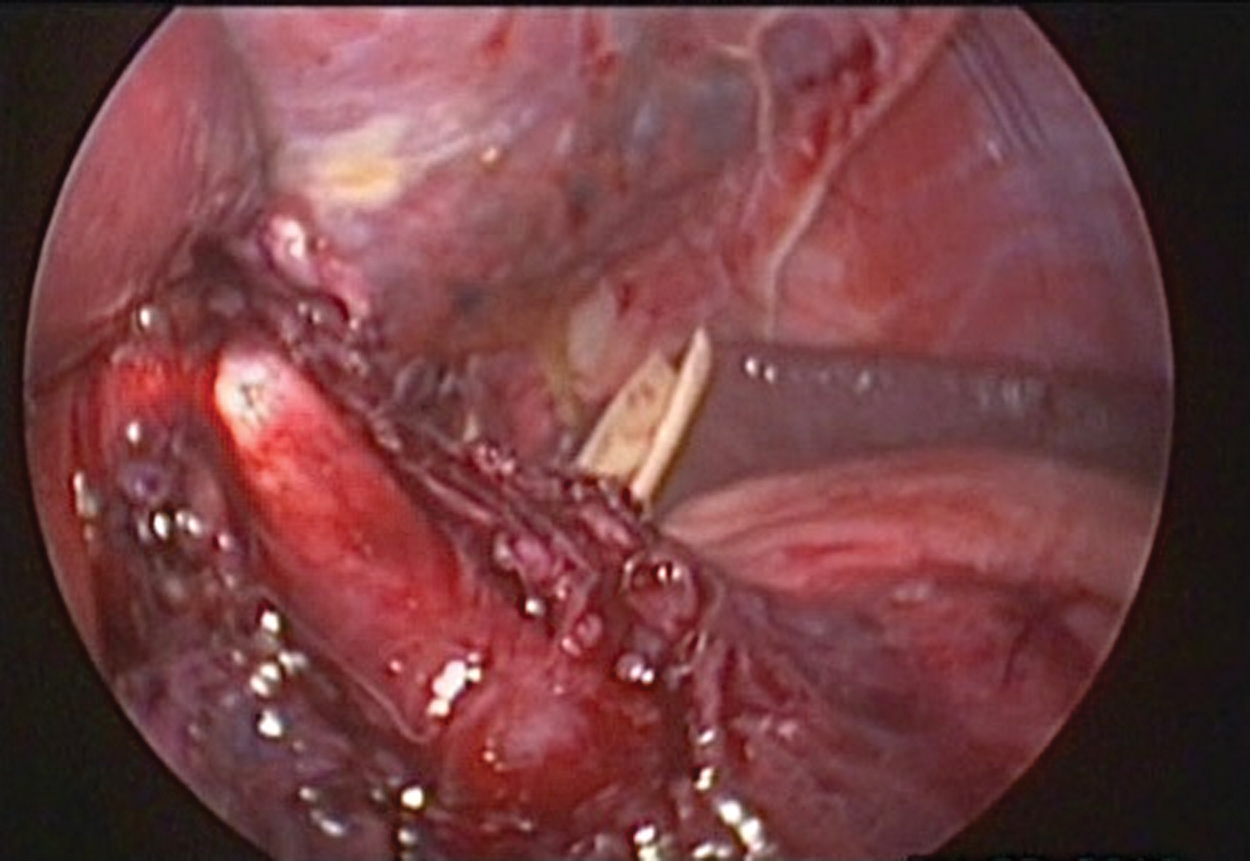
Peptic esophageal stenosis was diagnosed in 9 patients (6 male and 3 female) aged 4–15 years. Intraoperative endoscopy facilitated the esophageal dissection and identified the gastroesophageal junction below the diaphragm in 3 children who underwent a 360° Nissen fundoplication. In 6 patients, the gastroesophageal junction was located above the diaphragm; despite the extensive dissection of the hiatus, it was not possible to obtain 3 cm of free abdominal esophagus, leading to the diagnosis of a short esophagus. 11 A Collis–Nissen procedure 12 was performed through laparoscopy 8 with endoscopy assistance, and the gastroesophageal junction was identified. The endoscope was used as a splint in the minor curve to facilitate a Collis esophageal gastroplasty (Fig. 2). Furthermore, it helped in the identification and repair of leaks and was used to assess the efficiency of the neo-fundoplication built on the neo-esophagus. The operative time ranged from 120 to 150 minutes. No complications were associated with the flexible endoscopy.
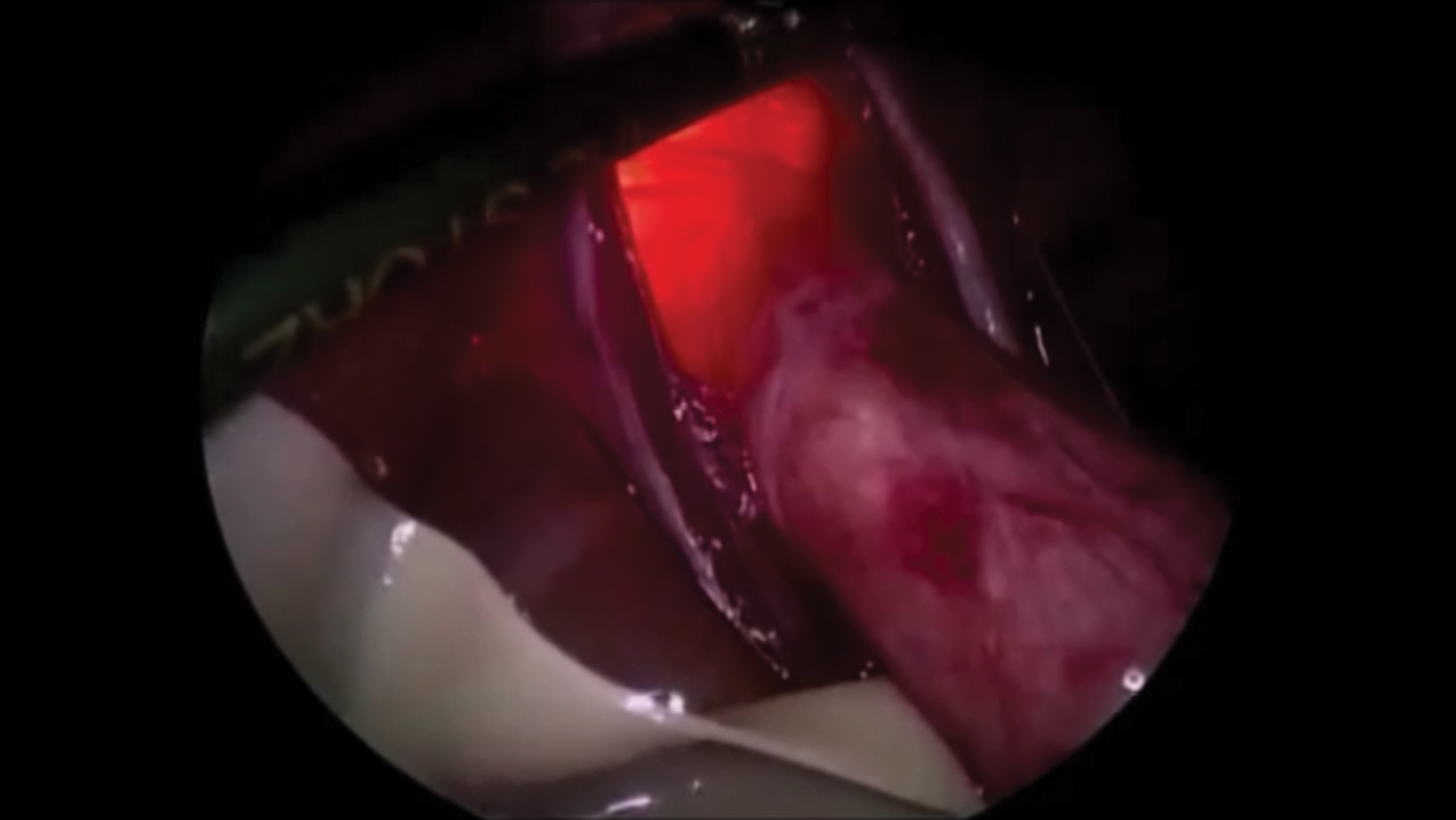
Achalasia was noted in 23 patients aged 1–20 years. The digestive endoscopy corroborated the diagnosis, allowing for the easy passing of the endoscope through a cardia that was not modified by the air insufflation. Thereafter, a laparoscopic Heller myotomy was performed 7 with endoscopy assistance, which verified the integrity of the mucous membrane (Fig. 3), as well as the adequate extension of the myotomy to the proximal area of the stomach. The air insufflation performed with an endoscope showed two perforations in the mucous membrane, which were repaired with absorbable suture 4-0. The average operative time was 78.33 minutes. No complications were associated with the endoscopy.
Paraesophageal hernia was noted in 42 patients (20 male and 22 female) aged 3 months to 16 years. Endoscopy allowed the identification and preservation of the esophagus located in a scarred area, as well as the identification of the gastroesophageal junction below the diaphragm in 37 patients. During the air insufflation performed with an endoscope, five gastric perforations were identified, and they were repaired before the construction of a new fundoplication. In 5 patients, the gastroesophageal junction was located above the diaphragm and a Collis–Nissen procedure was performed using an endoscope as a guide in the construction of the neo-esophagus and in the process of identifying and repairing leaks during the air insufflation. No complications were associated with the endoscopy.
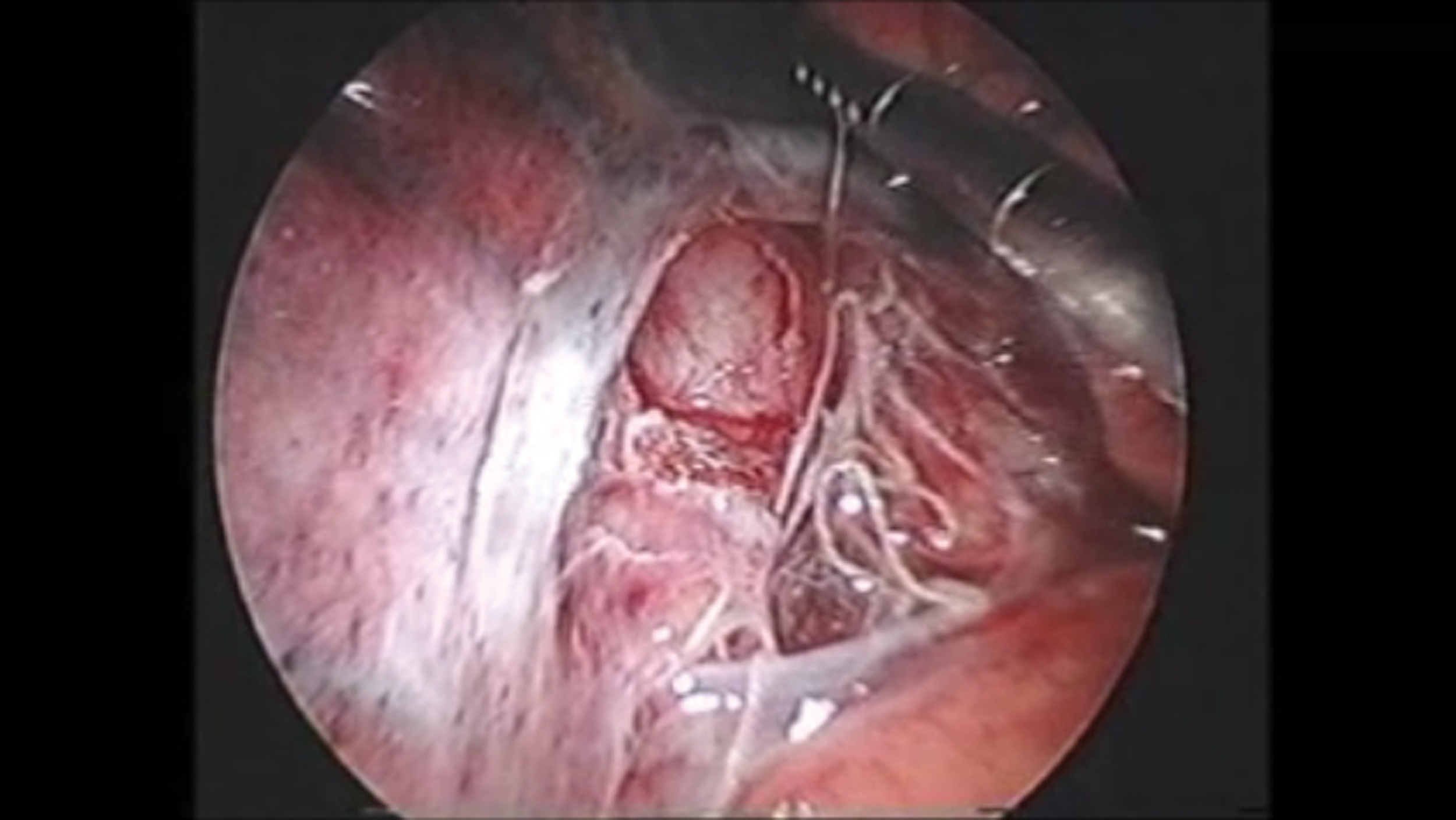
Congenital embryonic tracheobronchial remnants was noted in 4 patients (1 male and 3 female) aged 18–30 months. A resection and an anastomosis were performed; endoscopy showed permeability in the anastomosis and the absence of leaks through the air insufflation performed with an endoscope. The operative time increased from 2.3 to 3.1 hours, without secondary complications related to the flexible endoscopy (Fig. 4).
Esophageal duplication was noted in 2 patients (1 male and 1 female) aged 1 and 3 months old. A resection was performed in the duplication; endoscopy with air insufflation showed the integrity of the esophageal mucous membrane after the resection. The operative times were 60 and 85 minutes, respectively, with no complications associated with the endoscopy (Fig. 5).
Superior mesenteric artery syndrome was diagnosed in 2 patients aged 13 and 14 years, who both had severe neurological damage and secondary vertebral alterations and a previous Nissen fundoplication, performed 8 and 10 years, respectively, before the hospital admission. Abdominal distension, feeding intolerance, gastromegaly, and duodenal distension were noted. Preoperative endoscopy revealed an obstruction in the third part of the duodenum, and the air insufflation performed during the intraoperative endoscopy revealed a duodenal obstruction by the superior mesenteric artery. A gastrojejunostomy was performed on both patients without further complications (Fig. 6).
Giant gastric hemangioma was noted in a 7-year-old male patient with hematemesis and severe hypovolemic shock. A hemangioma located in the gastric fundus was resected. Intraoperative endoscopy showed that the permeability of the gastroesophageal junction was preserved during the gastric reconstruction. The operative time was 90 minutes, and there were no complications.

During the Collis–Nissen procedure, the endoscope helped to calibrate the diameter of the new esophagus. Color images are available online.
During a Heller myotomy, the integrity of the mucosa was appreciated with air insufflation. Color images are available online.
During the esophageal resection of embryonic remains, endoscopy revealed the extent of the disease. Color images are available online.
After resection of an esophageal duplication, endoscopy confirmed the integrity of the mucosa. Color images are available online.

Image of the dilation of the duodenum, secondary to the obstruction produced by the superior mesenteric artery. Color images are available online.
Discussion
The usefulness of endoscopy as an adjuvant to minimally invasive surgery in adults has been documented3,6,13,14; however, in children, there are only reports from isolated cases.7–10 Davenport et al. published a study of 30 children, 1 which suggested that endoscopy could be used to assist different procedures in non-seriously ill children. This article reports the use of endoscopy as an adjuvant to minimally invasive surgery in the upper gastrointestinal tract in 83 patients who underwent scheduled procedures.
Endoscopy as an adjuvant offered different advantages according to its uses in different pathologies in this study. In hiatal reoperations, it facilitated safe esophageal dissection, verified digestive tract integrity, and identified a few digestive tract perforations that were repaired. In children with esophageal stenosis, endoscopy facilitated the dissection and identification of the gastroesophageal junction while observing the Z line; this allowed the diagnosis of a short esophagus, and the planning of an esophageal elongation procedure. The endoscope worked as a splint in the construction of the neo-esophagus and by insufflating air, it helped to identify digestive tract integrity. In patients with achalasia and esophageal duplication, endoscopy was used to assess mucous membrane integrity. In congenital embryonic tracheobronchial remnants and gastric hemangioma cases, it was used to assess the resection extension and the functionality and impermeability of the repair. Endoscopy was also useful in the diagnosis of superior mesenteric artery syndrome after demonstrating duodenal dilatation due to an obstruction in the superior mesenteric artery.
Endoscopy as an adjuvant was only performed on stable patients. It is a safe method because there were no complications associated with the procedure in any patient. Furthermore, it prevented the development of complications by identifying secondary leaks from the dissection, which allowed their immediate repair.
In this study, we found that endoscopy as an adjuvant facilitates improved tissue dissection and diagnosis corroboration, and it makes it easier to ascertain the extension of diseases in some upper digestive tract pathologies.
Endoscopy also introduces increased safety to minimally invasive procedures in the upper digestive tract, while verifying the integrity of the dissected structures and the anastomosis.
For this study, endoscopy was only used in laparoscopic surgeries in the esophagus, stomach, and duodenum, but a broad spectrum of endoscopic procedures, such as bronchoscopy, gastroscopy, colonoscopy, and enteroscopy, can be used as adjuncts in other minimally invasive surgeries.
All the endoscopies were performed simultaneously by a pediatric surgeon from one surgical team that was trained in these techniques, and this facilitated their performance. Thus, we consider that pediatric surgeons must be trained to perform these procedures.
Conclusion
Digestive endoscopy is an excellent adjunct to minimally invasive surgery in the upper digestive tract in children because it facilitates and identifies complications, and ensures safer minimally invasive surgeries. This is a retrospective study; therefore, future prospective studies are required to assess these conclusions.
Ethical Responsibilities
The protocol for this research was approved by Hospital Infantil Privado, Teaching Department Headquarters. All patients provided signed informed consent.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.