
Abstract
Background:
Thoracic inlet (TI) tumors are rare, and can be particularly challenging to resect due to proximity to mediastinal vessels and nerves. Traditional resection is typically performed through “trapdoor” or sternoclavicular incisions. The purpose of our study was to evaluate the feasibility and effectiveness of thoracoscopic resection of this group of tumors.
Methods:
We performed a single-center retrospective chart review for children who presented with TI neuroblastic tumors between 2011 and 2020. Demographics, tumor characteristics, treatment, operative complications, and outcomes were collected and analyzed.
Results:
Eight patients were identified. The median age at diagnosis was 13 months (interquartile range [IQR] 6–32) with median tumor size at diagnosis of 4.1 cm (IQR 3.6–4.4). Neoadjuvant chemotherapy was given in 50% (4/8) with 38% (3/8) undergoing upfront surgery; 1 patient was observed without chemotherapy or surgery. Ultimately, 6 patients had thoracoscopic resection. For thoracoscopic resections, median intraoperative estimated blood loss was 15 mL (IQR 10–28), median operative room time was 199 minutes (IQR 152–259), and median hospital length of stay was 2 days (IQR 2–3). There were two complications: one recurrent laryngeal nerve injury and one new-onset Horner's syndrome. Complete gross total resection was achieved for all children and there were no recurrences or mortalities with a median follow-up of 3 years.
Conclusion:
Thoracoscopic resection for TI neuroblastic tumors is feasible with minimal morbidity and can lead to adequate oncological resection.
Introduction
Pediatric neuroblastic tumors arise from peripheral nerves or sympathetic ganglia and are characterized as ganglioneuroma (GN), ganglioneuroblastoma (GNB), or neuroblastoma (NB). 1 NB is the most common soft tissue malignancy of childhood, and thoracic NB occurs in ∼20% of all patients with NB. Compared with abdominal NB, thoracic NB is associated with an improved prognosis.2,3 For the past few decades, pediatric surgeons have adopted minimally invasive surgery (MIS) for paraspinal thoracic neuroblastic tumors and have demonstrated an associated decrease in hospital length of stay (LOS), operating room (OR) time, and estimated blood loss (EBL).4–6 However, similar adoption of MIS for thoracic inlet (TI) neuroblastic tumors has been limited with only one previously published study. 7 Traditional resection of TI neuroblastic tumors is approached through morbid incisions such as the modified Dartevelle sternoclavicular (Fig. 1), transmanubrial, and “trapdoor” with all of these approaches still common today.8–11 The purpose of our study is to report our institutional experience with a minimally invasive thoracoscopic approach for TI neuroblastic tumors.
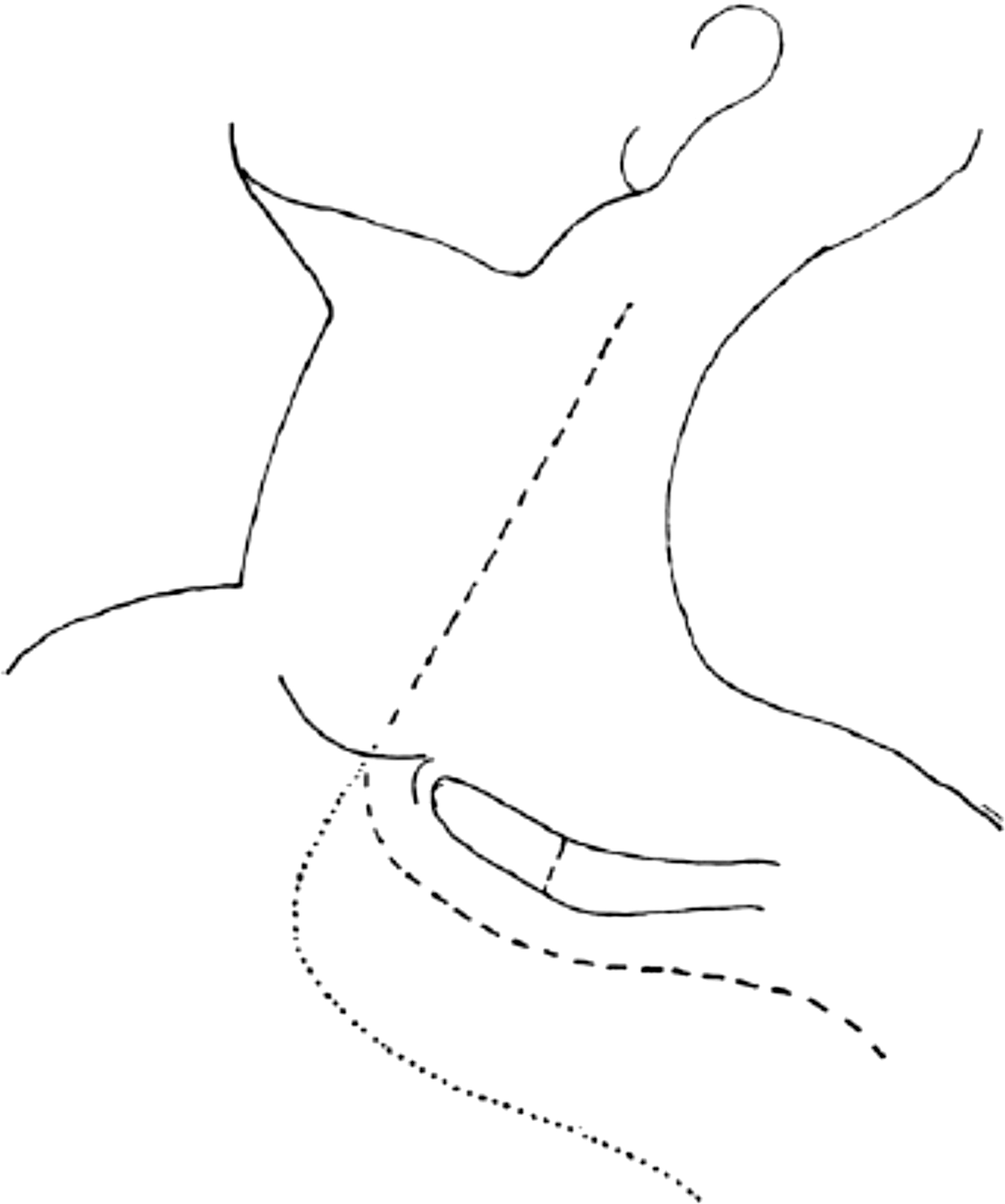
Modified Dartevelle's incision for exposure of TI neuroblastic tumors. The darker dashed line is the original author's modification of Dartevelle's incision. The line along the clavicle is the point of clavicular division. Reprinted by permission from Parikh et al. 9 TI, thoracic inlet.
Methods
Data source and study population
After Institutional Review Board approval, a single-center retrospective chart review was performed for all patients diagnosed with neuroblastic tumors between February 2011 and February 2020 (n = 266). Patients were excluded if the primary neuroblastic tumor was of intra-abdominal origin, such as the adrenal gland (n = 203). Computed tomography (CT) scans were reviewed for all thoracic neuroblastic tumors (n = 63) to determine if the tumor was located within the TI or paraspinal locations (Fig. 2). Ultimately, 8 patients were identified with thoracic tumors located within the TI.
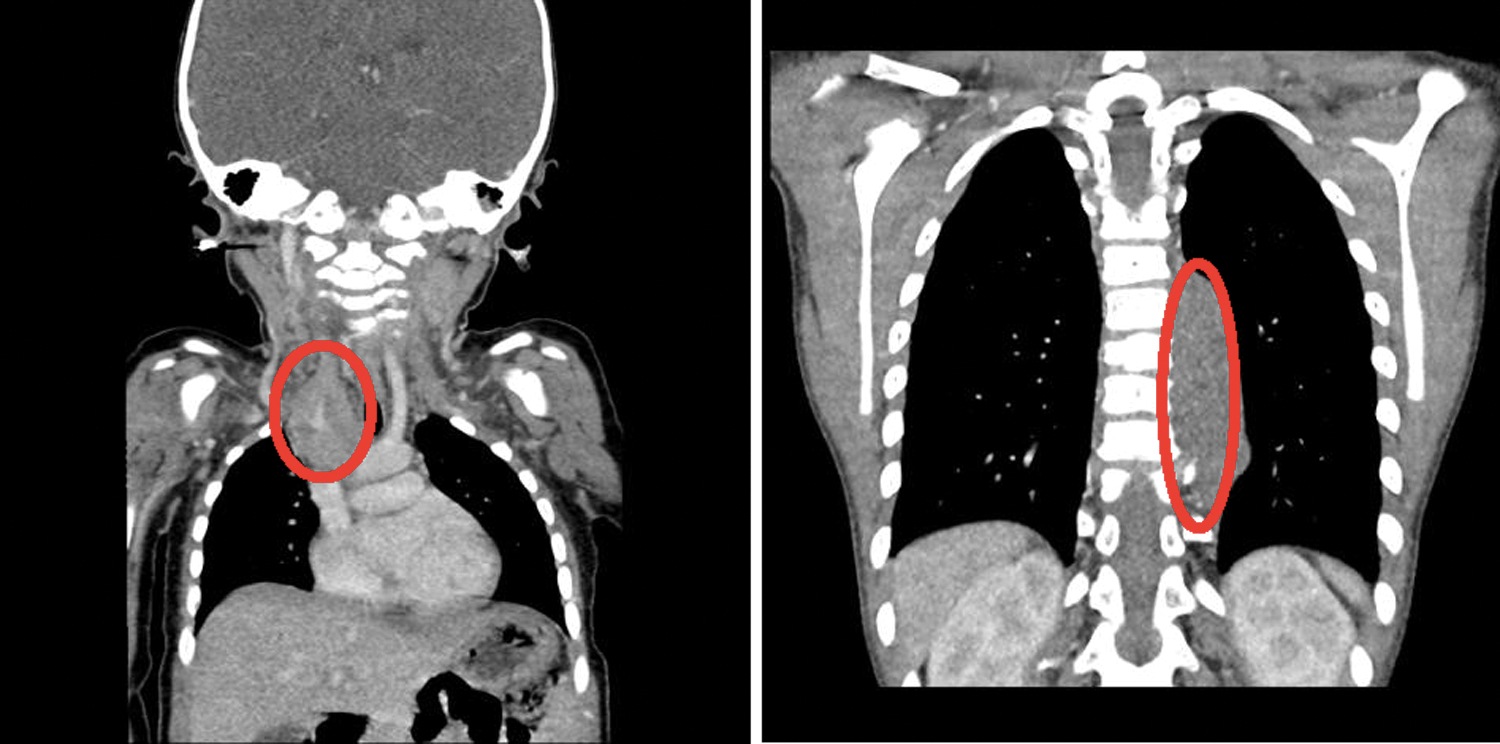
Examples of TI tumor (left) and paraspinal tumor (right). TI, thoracic inlet. Color images are available online.
Variables
Patient demographics collected included age and gender. Tumor characteristics included primary tumor diagnosis (GN, GNB, and NB), histological features, tumor size before therapy, image defined risk factors (IDRF), and risk group (low risk [LR], intermediate risk [IR], and high risk [HR]). Tumor size (i.e., maximum tumor diameter) and presence of IDRF were determined based on pretreatment CT scan. Treatment modalities included biopsy method (percutaneous and thoracoscopic) and neoadjuvant chemotherapy. Tumor size after chemotherapy was determined based on maximum tumor diameter with post-therapy CT. Primary outcomes evaluated were oncological outcomes (i.e., recurrence and gross total resection [GTR]) and overall mortality. Secondary outcomes were postsurgical hospital LOS, EBL, OR time, and postoperative complications. Continuous outcomes are reported as median with interquartile range (IQR) or range. Categorical outcomes are reported as percentages. Statistical analysis was performed using Stata version 16 (StataCorp, College Station, TX).
Results
Patient demographics, tumor characteristics, and neoadjuvant treatment
The median age at diagnosis was 13 months (IQR 6–32) with an equal number of male and female patients. An equal number of patients presented with Horner's syndrome (4/8) and respiratory symptoms (4/8). Median tumor size at diagnosis was 4.1 cm (IQR 3.6–4.4 cm). With regard to IDRF, a majority of tumors (5/8) were classified as L2 due to encasement of the subclavian, common carotid, and/or vertebral arteries. The remaining tumors (3/8) were classified as L1 with direct contact but not encasement of the subclavian, common carotid, and/or vertebral vessels. Diagnostic biopsy was percutaneous in 50% (4/8) and thoracoscopic in 38% (3/8) with 1 patient undergoing upfront resection. One tumor was a GNB and the rest were NB. Of the NB, 4/7 were IR, 2/7 were LR, and only 1 was HR. On histological analysis, no tumors had N-Myc amplification. Neoadjuvant chemotherapy was given in 50% (4/8) with 38% (3/8) undergoing upfront surgery. All 3 patients who underwent upfront resection had LR NB or GNB. A single patient (1/8) was observed without chemotherapy or surgery.
Specifically for patients who received neoadjuvant chemotherapy (4/8), the median age at diagnosis was 12.5 months (range 3–34 months) with a median tumor diameter of 4.3 cm (range 4.0–4.4 cm). Two of the patients presented with Horner's syndrome and the remaining 2 presented with respiratory symptoms. Tumor shrinkage after neoadjuvant chemotherapy was minimal (median 1.1 cm, range 0.1–4.4 cm), but one had complete regression. Chemotherapy was definitive for this patient due to a complete response on imaging. The remaining 3 patients proceeded to thoracoscopic resection after neoadjuvant chemotherapy.
Operative technique
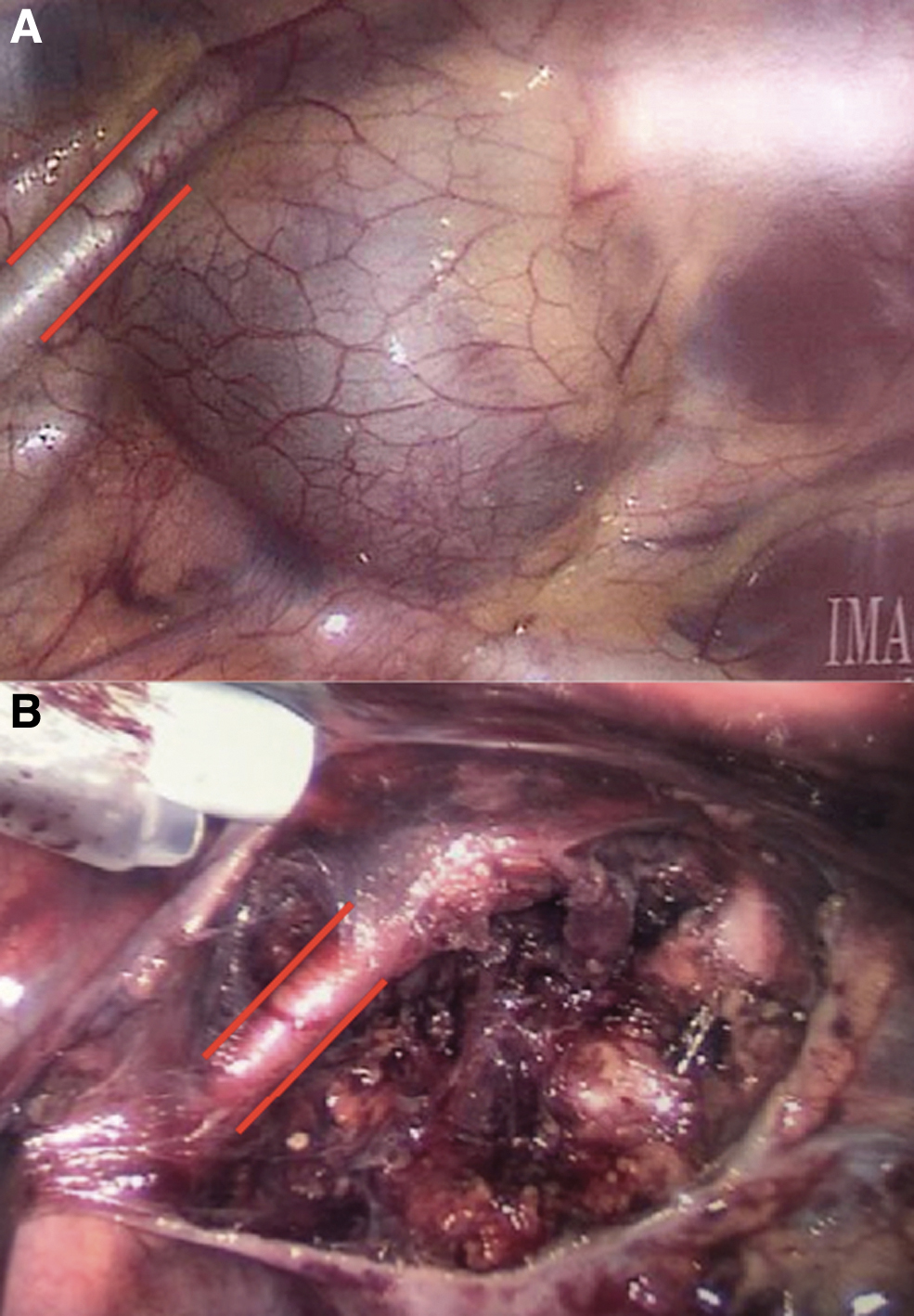
The surgical approach for thoracoscopic resection of TI tumors is as follows: the patient is placed in the supine position with a shoulder bump on the tumor side, and the ipsilateral arm is elevated and suspended above the patient's head (Fig. 3). The entire chest is prepped and draped with a sternal saw available in the OR in case the surgery is converted to open. Ports are inserted in the mid and anterior axillary lines at the second–fourth intercostal spaces. Lung isolation is generally not necessary. After incising the mediastinal pleura overlying the tumor, the tumor is carefully dissected away from surrounding vessels and nerves. Careful attention must be paid to the phrenic nerve as it enters the thoracic cavity and the recurrent laryngeal nerve on the right side as it crosses under the subclavian artery. Minimal cautery or alternate energy sources should be used, if possible, to avoid/limit nerve injury. If the tumor is tightly adhered to the vascular structures (more common after neoadjuvant therapy), then conversion to open approach may be considered. Once the tumor is dissected free, it can be placed in a glove finger, or a 5-mm endocatch bag if small to avoid inserting a 10-mm port. If larger, then a 10-mm port with an endocatch bag may be necessary. Figure 4A displays initial visualization of a TI neuroblastic tumor and Figure 4B displays the tumor bed after successful resection with the left subclavian artery skeletonized. A chest tube is placed to monitor for delayed bleeding or chyle leak.
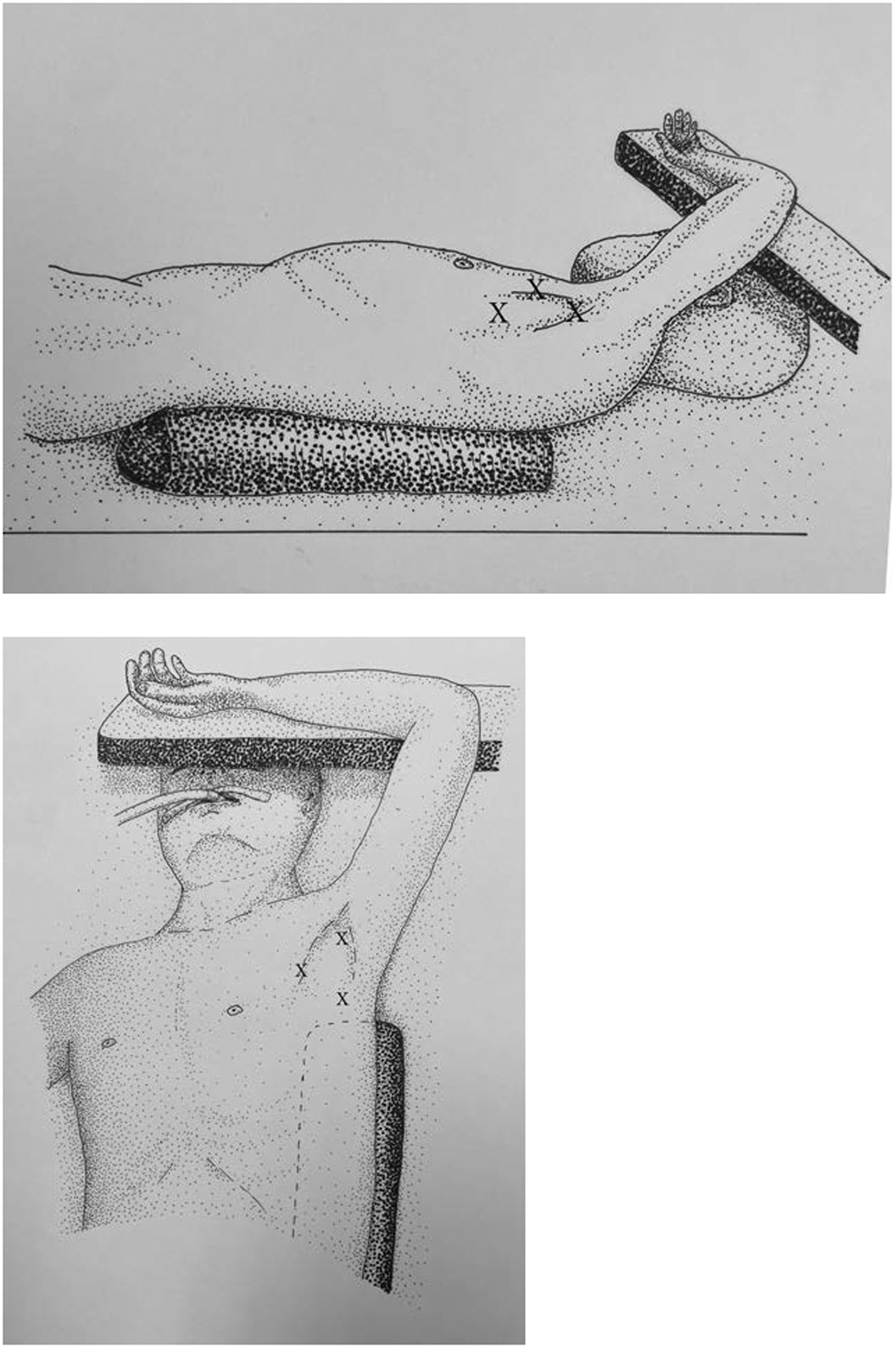
Patient positioning. Supine position with shoulder bump and ipsilateral arm elevated and suspended above the head. Port sites are represented by “X.”
Outcomes
In our series, the median intraoperative EBL was 15 mL (IQR 10–28 mL), median OR time was 199 minutes (IQR 152–259 minutes), and median hospital LOS was 2 days (IQR 2–3 days). There were two complications: one recurrent laryngeal nerve injury and one new-onset Horner's syndrome. Both patients have had complications managed conservatively with persistent miosis and ptosis at last follow-up (recurrent laryngeal nerve injury 65 months postresection and new-onset Horner's syndrome 24 months postresection). There were no bleeding complications, phrenic nerve injuries, or chyle leaks. Adjuvant chemotherapy (2/6) was started within 1–2 weeks after surgery. Complete GTR was feasible for all and there were no local recurrences or mortalities with median follow-up of 3 years (range 1.6–6.4 years).
Discussion
The purpose of our study was to describe our institution's experience with MIS resection of TI neuroblastic tumors. There are several important implications from our institutional experience. First, thoracoscopic resection for neuroblastic TI tumors is a feasible alternative to traditional open morbid techniques for surgeons with previous thoracoscopic experience. Second, the MIS approach for these tumors did not compromise oncological outcomes or GTR. And finally, our patients had minimal morbidity with complications successfully managed conservatively.
Traditional surgical approaches for resection of TI neuroblastic tumors are through morbid transmanubrial, sternoclavicular, or “trap-door” incisions.8–11 The transmanubrial approach has been reported in small case series but is associated with reduced shoulder girdle stability due to resection of the medial half of the clavicle. 8 Parikh et al. described a modification of this incision (i.e., Dartevelle's incision, Fig. 1), which re-approximated the clavicle and the periosteum after tumor resection, and was associated with improved range of motion around the shoulder joint. 9 In adult series, similar sternoclavicular incisions have been associated with shoulder girdle instability, prolonged recovery, and bony malunion in ∼40% of cases.12,13 Additional reported musculoskeletal complications after open approaches include scoliosis, elevation of the scapula, winged scapula, and nipple asymmetry with complications reported at an incidence of 30%–40%. 14 Another common incision reported at oncological centers of excellence (i.e., Memorial Sloan Kettering) within the past decade is the “trapdoor” incision. 10 Christison-Lagay et al. described their experience with “trapdoor” incisions for 13 patients with TI tumors of varying pathologies (primarily NB). 10 The authors reported five operative complications in their case series, including vocal cord paralysis (2), upper extremity neuropraxia (2), and hemidiaphragm paralysis (1), secondary to encasement of nerves by the primary tumor. One previous experience has also been reported for the successful management of TI neuroblastic tumors through an MIS thoracoscopic approach. 7 Based on our collective results, it appears to be a feasible alternative to the previously described open techniques for surgeons with thoracoscopic experience.
MIS was initially utilized in pediatric oncological surgery for biopsy, staging, and evaluation of resectability; however, for the past 20 years it has evolved to include therapeutic resection.15,16 Thoracoscopic resection of neuroblastic tumors is associated with decreased postoperative morbidity with shorter hospital LOS, decreased intraoperative EBL, and shorter OR times.4–6 An additional advantage for thoracoscopic resection is by decreasing postoperative LOS adjuvant chemotherapy can be resumed sooner. 5 As more articles have published the benefits and equivalent outcomes of MIS oncological surgery,1,5,6,8,15 experienced surgeons have incorporated this technique into oncological surgical practice, especially with paraspinal neuroblastic tumors.3,6,17 Disadvantages of oncological MIS are possibility of incomplete or compromised resection and inability to safely resect larger tumors. In all of our thoracoscopically resected tumors, >95% GTR was achieved. Furthermore, no patients had local recurrences after resection. Thus, our results show that thoracoscopic resection can be safely performed without compromising oncological outcomes for TI neuroblastic tumors.
A limiting factor for utilizing MIS approaches for all neuroblastic tumors is size. Phelps et al. identified tumors amenable to MIS resection usually have a volume <100 cc and have either had a substantial response to neoadjuvant chemotherapy or presented early with a paraneoplastic syndrome such as Horner's syndrome. 5 A benefit of the TI neuroblastic tumors is a majority of them will present early due to mass effect on adjacent neurovascular structures. Half of the TI neuroblastic tumors in our series presented with Horner's syndrome and the remaining patients presented with recurrent respiratory symptoms that prompted chest imaging. Owing to early presentation, tumor size at time of diagnosis ranged from 2.7 to 5.4 cm, which were all amenable to thoracoscopic resection. These results further emphasize the possibility to avoid morbid open surgical approaches for TI tumors due to early presentation.
Known postoperative complications after thoracic neuroblastic tumor resection include Horner's syndrome, chyle leak, pneumothorax, bleeding, and recurrence.1,4 As previously stated, Horner's syndrome is a common presentation of TI tumors and is a contributing factor to earlier diagnosis of this subset of neuroblastic tumors. In our series, new onset Horner's syndrome was diagnosed in 33% (2/6) of patients after thoracoscopic resection. This reflects the incidence reported in the literature of 3%–30%, 6 and is comparable, if not better, with the complication rate reported for open resection of TI tumors.10,11 Concurrent with the Horner's syndrome, 1 patient had an associated right recurrent laryngeal nerve injury due to an extensive dissection with proximity to the right subclavian and innominate artery. Fortunately, both of our patients' postoperative symptoms (i.e., miosis and ptosis) have had minimal effect on overall quality of life. In addition, despite proximity to major mediastinal vessels, there were no bleeding complications in our series. Although our sample size is limited, our results suggest an MIS approach for TI neuroblastic tumors can be performed with limited morbidity.
The most important and primary limitation of our study is its single-center retrospective nature. Furthermore, we were only able to identify 8 patients with TI neuroblastic tumors for the 9-year study period with only 6 requiring definitive resection. Although these numbers are limited, we were able to describe the feasibility and effectiveness of performing thoracoscopic surgery for neuroblastic tumors in the TI. This limitation can be rectified by the advent of a multi-institutional retrospective cohort study.
Conclusion
Traditional surgical technique for TI neuroblastic tumors is performed with sternoclavicular and “trapdoor” incisions, which have been associated with long-term morbidity and musculoskeletal issues in previous studies. For the past 20 years, oncological MIS has evolved from biopsy for staging to definitive resection. Our study shows the feasibility of applying MIS techniques for TI neuroblastic tumors, even in very young children.
Footnotes
Authors' Contributions
Study conception and design by S.C.M., R.S.W., S.A.V., J.G.N., and B.N.-M. Data acquisition by S.C.M. and R.S.W. Analysis and data interpretation, drafting of the article, and critical revision by all authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was used for completion of this study.